You turned to run upfield or avoid a defender and felt your knee pop and give way. In a short while, your knee is swollen, and you wonder, “Did I just tear my ACL?”
ACL tears are increasingly more common across many running sports. The management of ACL tears is constantly evolving. This comprehensive post will cover this severe knee problem from the time of injury through your post ACL surgery rehabilitation. This post contains links to many other posts about ACL tears, ACL surgery and recovery from ACL surgery.
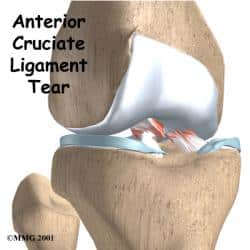
What is the ACL?
 The ACL is one of four major ligaments in the knee. The ACL is responsible for keeping your knee stable during activities such as turning, pivoting and twisting.
The ACL is one of four major ligaments in the knee. The ACL is responsible for keeping your knee stable during activities such as turning, pivoting and twisting.
Most people do not require an ACL for unidirectional (straight ahead) activities such as walking or even jogging on a track or road. Most athletes will require an ACL to participate in highly agile sports such as soccer, football, and lacrosse.
An ACL tear is the most common type of knee ligament tear. ACL injuries are also one of the most common ligament injuries in the human body. The incidence of ACL tears is increasing over the years due to many factors. Some research shows that young women are more prone to ACL tears than their male counterparts. This may be due to anatomical differences, landing and cutting mechanics, and some studies show that tears are more common during certain times of a woman’s menstrual cycle. In addition, the research has shown that year round single sports participation also increases an athlete’s risk of sustaining an ACL tear.
For those of you looking for a brief review of choices you have after an ACL tear read this post on ACL tear management Start to Finish.
What is an ACL Tear?
There are many ways to tear your anterior cruciate ligament or ACL. Although some injuries occur as a result of being struck on the side of the knee, most ACL tears are non-contact in nature. Most ACL tears or injuries occur during a rapid pivot to stop and change direction. Usually, the athlete was accelerating or decelerating rapidly; turning, pivoting or twisting. When the ACL tears, the knee buckles or gives out, and frequently a pop is felt or heard, and swelling occurs. If you sustained a knee injury while pivoting, turning or twisting rapidly, or heard a pop and experienced swelling, there is a very high probability that you tore your anterior cruciate ligament. The knee might not swell immediately; instead, it might swell after an hour or two – so get that ice on your knee as soon as possible. Ice should be applied 15 minutes on and 10 minutes off to minimize the risk of frostbite, and you should have a towel or something else between a bag full of ice and your skin.
What is the immediate treatment for an ACL tear?
If you suspect you have suffered a ligament tear in your knee, or more specifically, an ACL tear, you should immediately put ice on your knee. Next, apply compression via an ACE wrap (not too tight) and obtain a pair of crutches. You may need to see your orthopedist or visit an Emergency Room for these. The ice should be used 15 min on and 10 min off and you can continue this for the first two to three days to minimize swelling. Immobilization or bracing of the knee after an anterior cruciate ligament tear is typically not necessary and moving the knee helps prevent stiffness and muscle atrophy. Crutches are used after an ACL injury to be sure that you do not suffer any instability episodes where the knee gives out, and you fall. Your Orthopedic Surgeon will let you know when you can walk without crutches.
Related Post: Did I Just Tear My ACL?
You should have your knee examined and have X-rays taken within the first few days following a severe knee injury. Having a swollen knee is the most common finding in a severe knee injury. Usually, a physical examination alone will confirm the presence of an ACL tear. An MRI is useful to confirm the presence of a ligament tear, and it will also show if you tore your meniscus, or damaged your articular cartilage as well.
It is important for you to work on limiting swelling (ice, compression, and anti-inflammatories), and it is important to work on range of motion. The faster you gain back painless mobility – the less muscle atrophy and weakness you will have after a severe knee injury. Physical therapy can be useful after your initial ACL injury to assist in achieving these goals. Physical therapy before ACL surgery has been shown to improve the results after surgery.
Related: 4 Key Considerations when choosing your ACL Surgeon
We ran a set of ACL Expert Series posts in 2015. I and four other sports medicine surgeons, as well as prominent physical therapists in this area, discussed many of the questions you have asked us over the years.
- Do you need ACL surgery?
- How to choose an ACL surgeon
- What are your ACL surgery graft options?
- Physical therapy after ACL surgery is critical
- Understanding the psychological aspect of recovery from ACL tear
Do I need surgery for my ACL tear?
Need for ACL Surgery in Adults:
First and foremost bear in mind – The indication for an ACL reconstruction is not merely the fact that you have an ACL tear! Please read that again!! Many adults think (or are told by friends) that since the ligament is torn, they need it repaired – this is simply not true, and this is not what the scientific literature on ACL tears reveals.
Overall, in adults, the indication for an ACL reconstruction is symptomatic instability (the knee gives way or buckles) after your recovery from the initial injury, and you complete your physical therapy program. This means that we strive to treat patients and not simply your MRI findings. If you complete your rehabilitation program and your knee is stable for your chosen activities of daily living, and you do not work on roofs, ladders, or are a rock-climber, etc. then non-surgical management of your anterior cruciate ligament tear is possible – and effective.
ACL tears in children or pediatric ruptures of the ACL are viewed differently. We’ll discuss considerations for injuries in children in a second.
Anterior cruciate ligament surgery to reconstruct a torn ACL is not emergency surgery –and IF ACL surgery is necessary, you should probably postpone it until your knee swelling has diminished and you have normal range of motion. The stronger and more flexible your knee is going into ACL surgery, the easier your recovery from an ACL reconstruction should be.
In adults, an intact or functional ACL is occasionally (but not always) necessary to compete in certain sports with cutting, pivoting, or twisting. Many adults with ACL tears do well without surgery. Many adults return to playing tennis, or even *gentle* skiing, etc. without needing ligament surgery. Professional athletes almost always opt for surgical repair of their ACL tear.
Surgery to reconstruct your ACL is necessary if you have instability which significantly affects your quality of life. That assumes that physical therapy and perhaps bracing do not improve your ability to return to your chosen activity. You always have the option to alter your lifestyle to suit your knee or change your knee to suit your lifestyle. If the PT fails to control your instability – and if your knee remains unstable following an injury and you do not wish to wear a brace, or do not want to alter your lifestyle – then an ACL reconstruction is the preferred method of managing complete tears in symptomatic individuals.
Unfortunately, once you have suffered an ACL tear, you run the risk of developing osteoarthritis…. regardless of whether or not you have it repaired. Surgery usually will not prevent knee arthritis from occurring.
Need for ACL Surgery in Children:
Unfortunately, ACL ligament surgery is usually *necessary* for most pediatric ACL tears. Recent studies (2010) have shown that an *early* ACL reconstruction can minimize the risk of your child developing “secondary” injuries such as meniscus tears. Unlike adults, most children simply do not, can not, or will not alter their activity patterns. Therefore they have been found to be at much higher risk of developing secondary injury patterns when their knee buckles or gives way. Certain secondary injuries, such as a meniscus tear raise the risk of developing knee arthritis at a relatively young age. Please note, arthritis can still occur following non-surgical management or surgical management of an ACL tear… but the risk of arthritis ( and its rate of progression) increases if your child goes on to further damage other structures within the knee.
How is an ACL tear repaired at the time of surgery?
ACL surgery involves a reconstruction or replacement of your torn ligament. The ACL is typically not repaired in a traditional sense. Some research on new ACL repair techniques is now underway, but it is too early to tell if that technique will become the standard treatment. If you want to read more about these potential new techniques, see these articles:
That means we probably cannot sew together the torn ends of the ACL. Instead, we need to replace or reconstruct a new ligament with a graft. This is called an Anterior Cruciate Ligament Reconstruction.
Reconstructive techniques have undergone significant modifications over the past few years. Many sports medicine physicians, especially academic sports medicine physicians, have started performing more “anatomic” ACL reconstructions. That means that the new ACL graft is placed exactly where your old ACL was. This makes perfect sense, no? But, this wasn’t (and still isn’t) the way most ACL reconstructions are performed.
During surgery, we drill tunnels which enter and leave the knee joint where the ACL used to be. We then pass the “graft” through the tunnels and lock the graft in place – under tension. There has been a lot of research lately on the importance of obtaining an anatomical reconstruction of the ACL. This was the teaching decades ago and it did NOT reproduce the proper anatomy of the knee. The academic sports medicine community has been at the forefront of offering their patients anatomic ACL reconstructions which restore the normal ACL ligament location. During anterior cruciate ligament surgery, this is critical to restore proper mechanics and to restore stability as close to normal as possible.


Which ACL graft should I choose?
The choices for which tissue to use as a graft comes down to two basic options; allograft or autograft. An allograft is taken from a cadaver and autograft is your own tissue. If choosing your own tissue for an ACL reconstruction, we have the quadriceps tendon, hamstring tendons or the patella tendon as a choice for grafts. With allografts, we have a multitude of options available. Autograft is typically favored over allograft. Allografts carry a slight risk of disease transmission. To minimize that risk, many companies will radiate grafts, which could weaken them in the long run. For a primary ACL reconstruction autograft is probably your best choice. There are plenty of research papers which show that allograft (cadaver) ACL reconstructions fail more often than autograft ACL reconstructions.
After ACL Surgery:
What to expect after an arthroscopic repair of your ACL Tear:
- Pain: Unfortunately, even though this is an arthroscopic procedure, there is still a fair amount of pain to be expected. Usual techniques to minimize the pain after ACL surgery include:
- Ice
- ELEVATION – keeping the leg elevated, so the knee is above your heart
- Pain medication
- crutch walking
- Slowly moving your knee to keep it mobile
- Wound Management:
- Most surgeons prefer that you keep your surgical dressing intact for the first 3-5 days after ACL ligament surgery
- Remove the bandage after 3-5 days (check with your surgeon).
- Report any redness, drainage or other worrisome issues.
- Bathing, hot tubs and swimming pools are forbidden until the stitches are removed.
- Keep the wound covered, so the stitches do not rub on your clothing or bedding.
- Showering may be allowed by many doctors — check with them first
- Standing on the leg in the shower is OK. You will not injure your new ligament after ACL surgery
- Physical Therapy:
- Expect to be placed into physical therapy within the first week or two after surgery.
- Do not pivot, turn or twist on the leg after ACL surgery – let your new knee ligament heal first.
- Many surgeons follow the Moon protocol… but many surgeons have different approaches to therapy after ACL surgery – so check with them first.
- It is OK to bend the knee after ACL surgery, but concentrate initially more on getting the leg perfectly straight. It’s difficult, so many do not enjoy this, but it is a key milestone after ACL surgery.
- Return to activities:
- Your new ACL ligament in your knee requires a lot of time to heal after your ACL surgery.
- Avoid turning, side to side motion, twisting or pivoting for months after the surgery
- I allow cycling, and elliptical training soon after ACL surgery, but check with your surgeon.
- We will slowly advance your activity each time we see you… DO NOT start a new activity until your doctor gives you the green light after ACL surgery.
- BRING A LIST of questions with you… otherwise, you will forget to ask your questions about your restrictions after ACL surgery.
Related: Do I need a brace after ACL surgery?
What is a Double-Bundle Reconstruction?
A regular “native” ACL is composed of two bundles. An anteromedial and a posterolateral bundle. 99.9% of reconstructions performed today only recreate the AM bundle. Dr. Freddie Fu, 5 or so years ago proposed that we should be reconstructing both bundles to better control rotational instability that some patients continue to complain of after a routine ACL reconstruction.
A double-bundle recon involves four tunnels and two separate grafts…usually hamstring grafts to recreate both AM and the PL bundles.
I stumbled upon a fascinating site: ACL Surgery. This site is put together by a patient who underwent the procedure and found that the information available to them was incomplete. I do not condone nor advise that you take anecdotal notations as medical advice and in no way do I offer this as medical advice. But if you are seeking to learn what an ACL reconstruction is like from the patient’s perspective, I think you may find this site useful.
An evolving yet important area of research is in the prevention of ACL tears…. although technical, this is a very interesting paper.





