
 A recent article in the New England Journal of Medicine has attracted a lot of attention… and it should. The article focused on a group of patients with meniscus tears and osteoarthritis. The goal of the study was to determine whether or not surgery was necessary when compared to a group of patients who only had physical therapy. Although it was not the best study possible, the results are encouraging…. depending on your perspective :-) Physical therapy is equally effective at treating patients with both meniscus tears and osteoarthritis as surgery is. Imagine that!
A recent article in the New England Journal of Medicine has attracted a lot of attention… and it should. The article focused on a group of patients with meniscus tears and osteoarthritis. The goal of the study was to determine whether or not surgery was necessary when compared to a group of patients who only had physical therapy. Although it was not the best study possible, the results are encouraging…. depending on your perspective :-) Physical therapy is equally effective at treating patients with both meniscus tears and osteoarthritis as surgery is. Imagine that!
The issues, however, run deeper than those studied by the authors. Those issues include:
- Why were the MRIs performed in the first place?
- Why is it easier to get permission for an MRI and surgery than it is to get permission for physical therapy?
- Kudos to Dr Jen Gunter for her thoughts on this!
- Why do many patients expect an MRI for every joint ache or pain?
- Why do providers agree to order that MRI?
- Are we treating MRI findings— or are we treating patients?
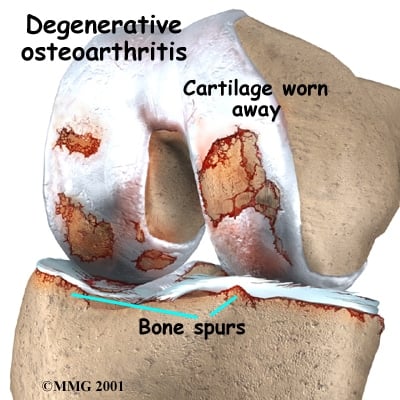
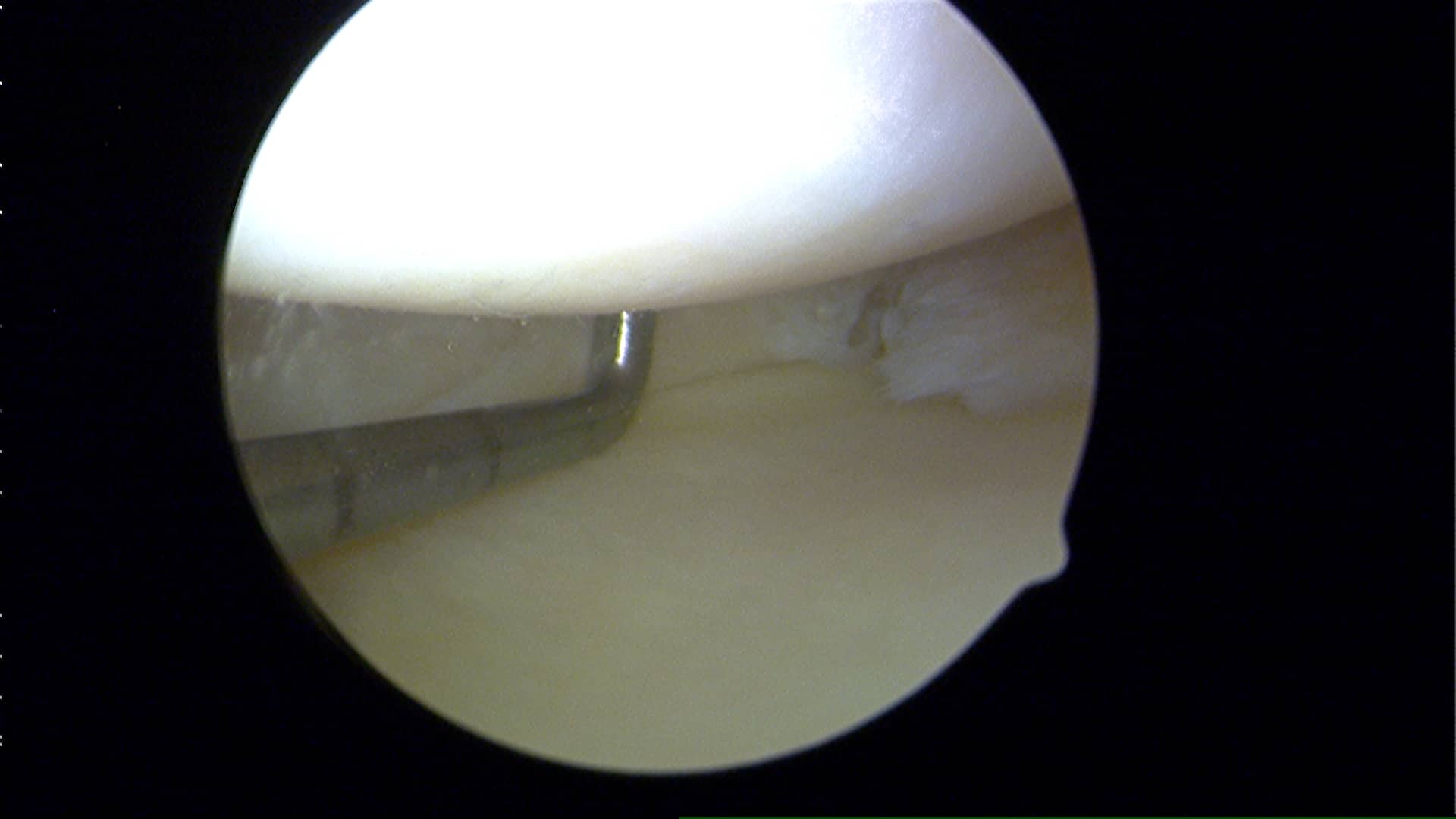 A meniscus is a cushioning disc found within our knee. We actually have two menisci. Osteoarthritis involves the loss of “articular” cartilage from the ends of our bones. As that cartilage erodes away our bones become exposed, and when the bones on opposing sides of the joint rub together… it hurts — occasionally it hurts A LOT.
A meniscus is a cushioning disc found within our knee. We actually have two menisci. Osteoarthritis involves the loss of “articular” cartilage from the ends of our bones. As that cartilage erodes away our bones become exposed, and when the bones on opposing sides of the joint rub together… it hurts — occasionally it hurts A LOT.
What most people in their 40s and up do not realize is that many of you have meniscus tears, and perhaps even a rotator cuff tear and yet you have no pain. Which meniscus tears hurt and why is an area we’re still studying. There are many different types of meniscus tears. Most tears are degenerative because our parts wear out… and surgery for degenerative tears without loose flaps is very rarely necessary.
If you sustain an injury and your knee hurts… you stand a really good chance of feeling better if you allow the body to heal itself. On occasion we need some assistance and that might mean a visit to your primary care doctor. Hopefully your provider can offer you some tips to set you on the path to recovery… but very rarely should an MRI be ordered (or asked for) soon after the initial injury. MRI’s should be used to confirm diagnoses… not to make a diagnosis. They are most useful if you have failed non-surgical treatment and we are considering surgery. Even in the realm of professional athlete injury management the issue of over-utilization of MRIs has gained a lot of attention .
Given the insight gleaned from this paper, your primary care doctor should likely start you in physical therapy if they suspect that you have suffered a meniscus tear, and your X-rays show evidence of arthritis. But our primary care docs are getting squeezed… they need to see too many people each and every day just to be able to keep their doors open. That leads to rushed visits, easy scripts for MRIs and premature referrals to specialists. That opens the door for a specialist to then recommend an operation based on the MRI findings… and not necessarily because they are treating you as a patient. Many variables need to be considered whenever surgery is being thought of as the primary treatment modality. Your MRI finding is but one small consideration in that “shared decision making process“.
The big picture… many patients will have meniscus tears that will marginally affect their quality of life, if at all. Not all weekend injuries require an MRI … time heals most injuries alone. Surgery is not necessary for all meniscus tears. Doctors need to commit to be willing to spend as much time talking about the non-surgical treatments for meniscus tears as they do trying to explain what the surgery entails. While surgery might ultimately prove to be the proper course of treatment to pursue for certain meniscus tear… it should only follow a course of failed non-surgical treatments for your meniscus tear and osteoarthritis.
Questions? Why don’t you come in and discuss your options. :-)











Thanks for your reply. Taking my example again. I have 2 small tears in the lateral meniscus and 1 of 1.2 cm on the posterior horn of the medial meniscus. All 3 were left in situ at surgery time, my surgeon mentioned that he might have to go back and do something about the medial meniscus tear if it propagate and become an issue. Why take this risky approach and not repair it or trim it at the time of surgery ? Is it better to keep a torn meniscus asymptomatic or with very little symptom or do a partial menisectomy ? I read that a meniscus tear can lead to Chondromalcia if left untreated ? Is a tear left in situ more protective of my join even if reasonably large like 1.2 cm than doing a partial menisectomy ?
My age again is 43.
I am 11 weeks out from meniscal repair. I have severe OA in both knees. My insurance has just approved Supartz (3 injection in each knee). I have had 16 PT sessions and there is conflict about how I should exercise,the PA says no walking unless I have to,the PT says to walk 2-3 miles a day. How do I know what to do without worsening the OA in the knees?
Your OA will worsen no matter what you do. That’s the natural history of it. Inactivity is very bad for your health.. and most arthritic knees actually like to move.
twisted my knee as I fell. ortho doc said treating meniscus makes oa worse. true?
It is possible …
I had surgery for it. Fixed it. Off of crutches in two days. Worth it.
Dr Luks,
i am 19 years old and have had a lateral meniscus tear for about 3 years. i am ok with light sports like running or gym exercizes but when i try to play football again. i get massive inflammation which leaves me in pain and unable to walk without a limp for about a week after playing. from reading many articles im am not sure what to do as i have read getting the meniscus repaired leads to early arthritis but not doing so can also do the same. would really appreciate your opinion on the matter. Thanks
Hi ! I would love to help you with your questions. You can find me on Curely where I can answer questions by text or email … Join me there. http://www.curely.co/
MRI shows a medial posterior meniscus tear, I am 80, one doctor says go as long as can before a total knee repair as orthoscopic would make it worse, another doctor ( fellowship train, and young) says a 15 minute orthoscopic surgery would keep the tear from getting worse. It catches and I walk stiff leg at times .There is pain. what is right? Primary doctor says PT. Time and travel is a problem. WHAT SAY YOU/
At 80… most arthroscopic surgeries do not end well. If there is significant arthritic change, then an arthroscopy has a chance of not working well. plus, the risk of stress fractures after surgery increase due to osteoporosis too. Difficult decisions, without examining you I can not offer specific advice