Shoulder Pain
Rotator cuff injuries are very common. Over the age of 30, the rotator cuff is responsible for the shoulder pain that most of us experience.
Determining the cause of your shoulder pain and determining what the actual pain generator is in your shoulder is our job as a shoulder specialist. Until we know why your shoulder hurts, it’s hard to start a treatment plan.
The most common causes of shoulder pain will vary by age, your activities and whether or not you have suffered any trauma. Rotator cuff injuries are only one of the many sources of pain in the shoulder.
Shoulder Pain by Age
Children and teens tend to have overuse tendonitis … or shoulder dislocations and labral tears due to trauma or sports injuries.
“Young” Adults and “weekend warriors” tend to have shoulder pain due to rotator cuff injuries or rotator cuff changes (tendinosis). Tendinosis and other degenerative changes within the rotator cuff occur as a result of genetics, activities, and aging. In this age group rotator cuff injuries may also occur as a result of trauma or injuries, but rotator cuff degeneration is the most common reason we see you in our office.
Seniors tend to have shoulder pain due to arthritis, loss of cartilage, and small, medium or even very large chronic (old) rotator cuff tears from a lifetime of wear and tear. Sometimes the torn rotator cuff tendon will upset the tissues around the tendon and cause a bursitis. This secondary bursitis is a common cause of pain and discomfort.
The Most Common Cause of Shoulder Pain In Adults
In adults, the most common source of shoulder pain are injuries of the rotator cuff … a series of 4 small muscles that coordinate the motion of the shoulder. This post on what is the rotator cuff will clear many questions about its structure and function. Again … The most common cause of shoulder pain is actually rotator cuff tendinosis, or partial tears of the rotator cuff.
Rotator Cuff Tears
Let’s talk about rotator cuff tears (injuries). A lot of people say rotator cup tears— but it’s actually rotator cuff (C-U-F-F) tears.
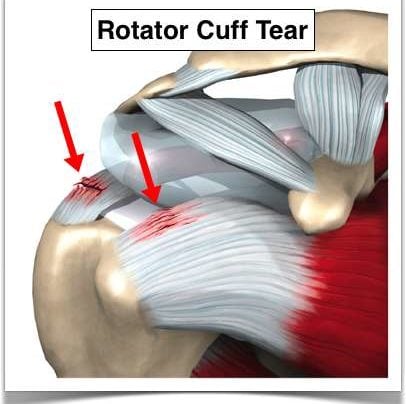
What is the rotator cuff?

The rotator cuff are four small muscles located around your shoulder and they link together to form a cuff that literally sits on top of the top of your humerus. It’s beneath your deltoid so you can’t actually see or feel the rotator cuff. The purpose of the rotator cuff is to take all the energy or strength derived from the larger muscles such as the deltoid or latissimus or your pec major or your chest muscles and turn it into meaningful motion or rotational motion so you can move the arm out, move the arm up, any way you want to place it in space.
[hr]
What causes rotator cuff tears?
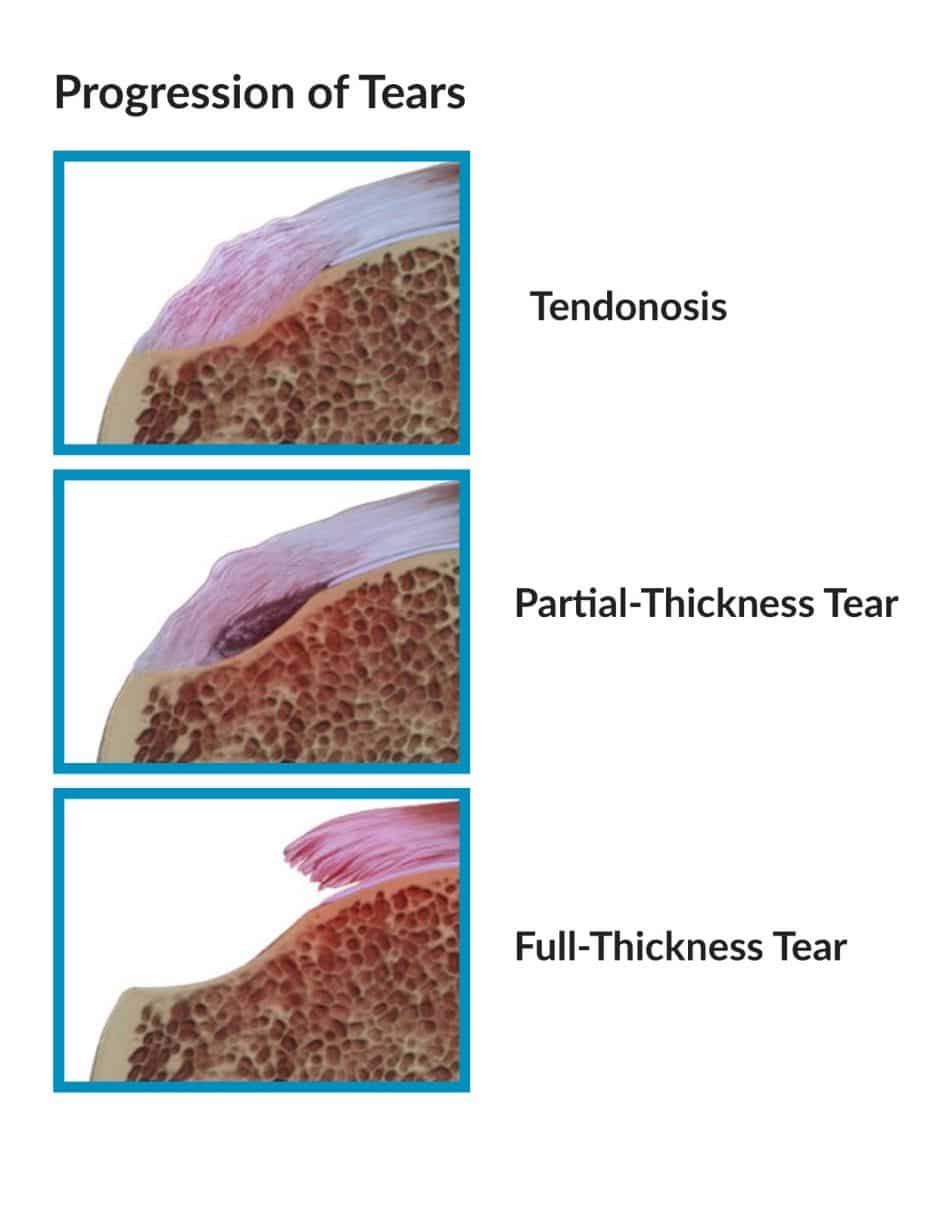 With time, sometimes with usual activities, sometimes with trauma, our tissues wear out, degenerate or tear. The vast majority of rotator cuff tears that we see in the office are attributed to attrition. Your tissues just wore out. Think of your favorite pair of blue jeans that you’ve had since high school if you could still fit in them that — think about the knees on the front of your jeans that that denim just wore out one day. You felt a breeze and looked down and there was a hole there. A portion of your rotator cuff tissue is not very different than that. It goes through a process of degeneration or something we call tendinosis which you can look up on my website. Tendinosis can progress from degeneration to fraying of the surface to a partial tear to a full-thickness tear where a portion of the tendon has detached from the bone.
With time, sometimes with usual activities, sometimes with trauma, our tissues wear out, degenerate or tear. The vast majority of rotator cuff tears that we see in the office are attributed to attrition. Your tissues just wore out. Think of your favorite pair of blue jeans that you’ve had since high school if you could still fit in them that — think about the knees on the front of your jeans that that denim just wore out one day. You felt a breeze and looked down and there was a hole there. A portion of your rotator cuff tissue is not very different than that. It goes through a process of degeneration or something we call tendinosis which you can look up on my website. Tendinosis can progress from degeneration to fraying of the surface to a partial tear to a full-thickness tear where a portion of the tendon has detached from the bone.
[hr]
Traumatic rotator cuff tears versus degenerative rotator cuff tears
There are also situations where you have a normal rotator cuff or a cuff with slight degeneration. You go outside. You play sports. You get tackled and knocked down or you slipped on the ice and fall on that shoulder or as you’re falling you reach for something to hold onto it and you yank your shoulder. Those situations can cause acute traumatic ruptures of the rotator cuff. Is there a difference between attritional and traumatic rotator cuff tears? Absolutely.
Most of us, and I mean academic physicians, believe that attritional rotator cuff tears can be managed in the majority of situations – non-operatively (without surgery). That means with physical therapy or doing nothing if doesn’t bother you too much, occasional injections, etc. If those non-operative modalities are unsuccessful in alleviating your pain AND you have significant pain with use or severe pain at night when you’re trying to sleep, then surgery is an option. But it is YOUR decision. Some tears will grow in size with time. So even if your tear feels better after therapy, you should see your surgeon every 4-6 months for a follow-up to see if the tear has become larger.
Acute or traumatic rotator cuff tears are a different story. Those should generally be repaired. (Again, not all acute tears need surgery and once again, my disclaimer applies and this is not medical advice. You should talk to your orthopedist.) But if you slip and fall and tear your rotator cuff, the likelihood of it being a large tear is fairly high. Those rotator cuff tears have a very good chance of healing after surgery. Should acute rotator cuff tears be fixed sooner rather than later? Yes.
[hr]
Can I delay my rotator cuff surgery?
Yes, assuming you understand the implications of that decision. A few issues to consider.
(1) Retraction. The rotator cuff is like a loaded rubber band, all right? Imagine a rubber band between my two fingers. I release it on one end. What’s gonna happen? It’s gonna shoot over towards the other finger. The muscle is no different. If the rotator cuff retracts or pulls far enough away from the bone, it will make the repair difficult and the likelihood of a successful repair when all is said and done much lower.
The other issue with waiting: Fatty atrophy. Atrophy is simply put — picture a leg that goes into a cast. You take the cast off in four weeks and that leg has shrunk. What has happened? The muscles have atrophied or become smaller. What happens with rotator cuff muscles that are no longer attached to the bone? The body changes the muscle to fat. It’s very cruel because if you re-establish continuity of the tendon, it doesn’t turn the fat back into muscle. So if you wait on a large, retracted, acute rotator cuff tear and that tissue turns to fat, then it doesn’t matter if you get it fixed later, because you’re fixing a piece of fat and it no longer functions as a muscle.
[hr]
Night Pain and Rotator Cuff Tears
Most patients with rotator cuff tears simply have pain. A few may have weakness and loss of motion as well. Rotator cuff pain can be activity related — such as trying to reach overhead: trying to wash your hair; for women, trying to put on a bra; for men, trying to put on a belt, or even trying to reach back and pull something out of the backseat of your car.
What brings the majority of patients into an office for small rotator cuff tears? Night pain. You can’t get comfortable at night or you’re waking up at night. Larger rotator cuff tears that encompass at least one or two complete tendons — will complain of weakness. They simply can’t lift the arm up or if they do, they can’t lift it far.
It will take an examination by an orthopedist and perhaps an ultrasound or an MRI to determine the actual size of the tear. X-rays may be useful to reveal changes that we can see in the bone that are secondary to rotator cuff disease as well.
So, bottom line take-home message:
Do all rotator cuff tears need to be “fixed”?
The answer is no. You can go much slower on the small attritional rotator cuff tears where the tissue simply wore out and try a course of therapy, injections, etc., However, we need to consider being much more aggressive with large acute traumatic tears after a significant incident or traumatic event.
We would love to see you if you have any lingering questions about your rotator cuff or shoulder injury:

Any questions? Please feel free to post them in the comments.
Remember, this for informational purposes and is not medical advice. Evidence changes frequently which makes some of these comments out-dated in the future and since it is a transcription I will not change them.









Dr Lusk , my MRI shows partial tears of the supraspinatus and a full tear of the subscapularis with dislocation of the bicep . Can these be rehabilitated without surgery ?
Many thanks,
IM
The Subscapularis is considered by most to be the most crucial rotator cuff muscle. In addition, when it tears, the biceps will usually dislocate. The torn tendon, if complete will produce significant shoulder dysfunction… and the biceps will produce ongoing pain. This scenario is usually best treated surgically.
..
Dr. Lusk.
I am a retired on disability 65 year old Male with past history of knee surgery in 1971 and fusions both in the cervical and lumbar spine regions in 1994. Since there was nerve damage associated with the spinal fusions, I know I have unexplained, random “pains”. No known trauma to shoulder. 3/13 I began feeling pain when raising RT arm and problems sleeping. Saw Pain Management Doctor on 5/30/13, the exam on a Fluoroscope reveled a small Labral Tear of the right RC. Received cortisone injection. Was told if the condition continued to see an Orthopedic Surgeon. Pain return, on 11/11/13 saw an Orthopedic Surgeon. After physical exam, he did a shoulder x-ray and injected another shot of cortisone and set up an appointment for an MRI. The MRI showed:
1. Full thickness tear distal supraspinatus with 2.2cm proximal retraction.
2: Articular surface partial tearing critical zone anterior infraspinatus fibers.
3: Type III acromion with anterior spurring.
4: Degenerative chance at the AC joint with joint effusion and undersurface osteophyte formation.
5: Diffuse irregularity of the glenoid labrum suggests chronic degenerative tearing.”
The Doctor recommended RC surgery, but he only does the “open method”. I asked if Arthroscopic surgery was a option, he referred me to one of his younger associates. He also recommended I have surgery.
I live alone, do not have anyone close that can help me after the surgery. I was told Home PT and limited Home Health care services are available. I am worried the lack of other “help” will be a major drawback.
In your opinion, with this limited information, should I get a Second Opinion? Is there a possibility surgical repair may not be the only answer?
Thank you for your blog and sharing your training and experience.
Thanks for stopping.. and thank you very much for the kind comments about the blog! The American Academy of Orthopedic Surgeons recently published a guideline approach to rotator cuff tears… http://www.aaos.org/news/aaosnow/oct13/cover1.asp It is worth reviewing. It clearly shows that a trial of non-surgical treatment with physical therapy, injections, oral medications etc is very much worthwhile before considering surgery. Having surgery while living alone is very very difficult because of the limitations we impose on your activity. It can be done.. but it’s not easy.
Good Luck
Howard Luks
Dr. Lusk,
I greatly appreciate your thought and response to my questions. Both Doctors are members of AAOS. To my knowledge, they did not ask the questions to evaluate my condition completely using the new AAOS AUC. I in no way would ever disrespect a Doctor with an attitude questioning their ability. In your opinion, would I be out of line to make another appointment and simply ask if they use the new AUC? I do have other questions I need to ask before treatment continues.
Thanks,
Charles
Charles…
Physicians are well aware that 80+% of patients are researching their diseases, injuries, doctors, etc. If they are not willing to entertain a patient’s questions about a procedure or treatment recommendation then it may be time to seek a another opinion. You would not be insulting me if you asked me what my thoughts were on the new treatment recommendations put forth by the AAOS.
Good Luck
Howard Luks
Dr. Luks,
Not sure how to get to Dr. Luks, but I hope he reads this…..I had a rotator cuff repair in August of 2013 and 4 months later could not raise my arm at all. An MRI showed I had a tear again, the doctor said it looked like it wasn’t a fast tare but a slippage. He did another rotator cuff repair and said he put so many anchors in it that my shoulder will never tear. Again at 5 months I can not rise my shoulder. He wants to do a nerve study of my shoulder and a neck MRI. I really want an MRI of my shoulder. What do you think?
Dana …
Without examining you I can not really comment on what is wrong. Weakness can be due to a massive tear of the rotator cuff or a nerve that’s not functioning well.
You can always seek another opinion.
Good Luck to you!
/hjl
Dear Dr. Luks, (leaving this comment twice, first time I think was the wrong place. thks)
First a hearty thank you for your site and the blog. Since I have learned that I will likely need surgery on the supraspinatus tendon, I have been reading online about this, and your site has been by far the most helpful.
I will (try to) be brief: 48 male who is very active and an avid swimmer. Four years ago I developed pain in my rt shoulder and saw several Drs and ended up in PT, but after month without success, had an MRI and learned that the supraspinatus tendon had come completely off the bone. Had pain, for a long time, but never terribly intense, and remained active.
More recently, regularly swim long distances (avg 2 miles and i.e. thus far rt shoulder surgery worked) and started to develop some pain a few months back in left. As I continued to swim the pain grew but is very tolerable. To be safe I had 2 MRIs, and the second with ink inserted into the rotator cuff. Results:
Glenoid labrum: Conscious material extending into the super laburm posterior to the biceps anchor compatible with a SLAP lesion.
Supraspinatus tendon: Near full-thickness tear at the footprint of the supraspinatus. with contrast material extending through essentially the full thickness of the tendon, but not entering the subracromial-sub-deltoid bursa. On the sagittal images, the tear measures approx 1.8 cm in anteroposterior diameter, involving most of the supraspinatus footprint. Contrast in is extending deep into the substance of the tendon nearly to the level of the myotendinous junction. Normal ….. muscle belly.
The rest unremarkable
Except: Type II acromion with concave undersurface. No evidence of os acromiale. The AC joint is not widened. (Paraphase here) Relationship of acromion and clavicle is maintained. Trace fluid in acromioclavicular joint. Near joint, near skin surface, small 9 x 4 mm cyst, presumably arising from the AC joint.
Impression: 1. near full thickness tear of supraspinatus, sparing bursal fibers, without contract entering the subacromial-subdeltoid bursa. 2. Type II slap lesion. 3. Small AC joint cyst.
Insurance Codes for surgery for this Sat, June 7, 29827, 29807, 23430, 29826.
fyi I still swim regularly without much pain, but perhaps slowly increasing. I am about to lose a job by the end of June and thus insurance. My primary concern is that the tendon is likely to come off completely and than require surgery.
Thanks so much for bothering to read. Do you agree surgery is necessary? Regards and appreciation for this service you provide. Dr. Jimmy Weir – anthropologist.
James… I think you should seriously consider another opinion or two. SLAP lesion repairs are rarely necessary at our age… and even if the surgeon feels it may be the source of your pain, a repair is not the recommended procedure for it. In addition, surgery on partial thickness tears is recommended more as a quality of life issue than anything else. I would take your time, talk to your doctor and perhaps another shoulder specialist.
Good Luck
Howard Luks