Shoulder Pain
Rotator cuff injuries are very common. Over the age of 30, the rotator cuff is responsible for the shoulder pain that most of us experience.
Determining the cause of your shoulder pain and determining what the actual pain generator is in your shoulder is our job as a shoulder specialist. Until we know why your shoulder hurts, it’s hard to start a treatment plan.
The most common causes of shoulder pain will vary by age, your activities and whether or not you have suffered any trauma. Rotator cuff injuries are only one of the many sources of pain in the shoulder.
Shoulder Pain by Age
Children and teens tend to have overuse tendonitis … or shoulder dislocations and labral tears due to trauma or sports injuries.
“Young” Adults and “weekend warriors” tend to have shoulder pain due to rotator cuff injuries or rotator cuff changes (tendinosis). Tendinosis and other degenerative changes within the rotator cuff occur as a result of genetics, activities, and aging. In this age group rotator cuff injuries may also occur as a result of trauma or injuries, but rotator cuff degeneration is the most common reason we see you in our office.
Seniors tend to have shoulder pain due to arthritis, loss of cartilage, and small, medium or even very large chronic (old) rotator cuff tears from a lifetime of wear and tear. Sometimes the torn rotator cuff tendon will upset the tissues around the tendon and cause a bursitis. This secondary bursitis is a common cause of pain and discomfort.
The Most Common Cause of Shoulder Pain In Adults
In adults, the most common source of shoulder pain are injuries of the rotator cuff … a series of 4 small muscles that coordinate the motion of the shoulder. This post on what is the rotator cuff will clear many questions about its structure and function. Again … The most common cause of shoulder pain is actually rotator cuff tendinosis, or partial tears of the rotator cuff.
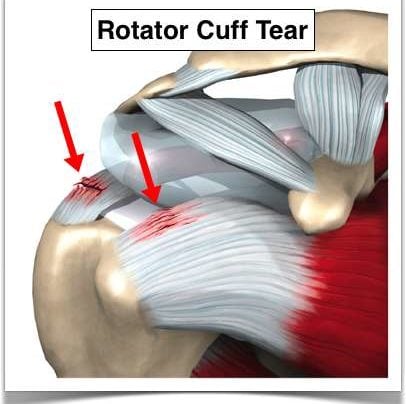
Rotator Cuff Tears
Let’s talk about rotator cuff tears (injuries). A lot of people say rotator cup tears— but it’s actually rotator cuff (C-U-F-F) tears.
What is the rotator cuff?

The rotator cuff are four small muscles located around your shoulder and they link together to form a cuff that literally sits on top of the top of your humerus. It’s beneath your deltoid so you can’t actually see or feel the rotator cuff. The purpose of the rotator cuff is to take all the energy or strength derived from the larger muscles such as the deltoid or latissimus or your pec major or your chest muscles and turn it into meaningful motion or rotational motion so you can move the arm out, move the arm up, any way you want to place it in space.
[hr]
What causes rotator cuff tears?
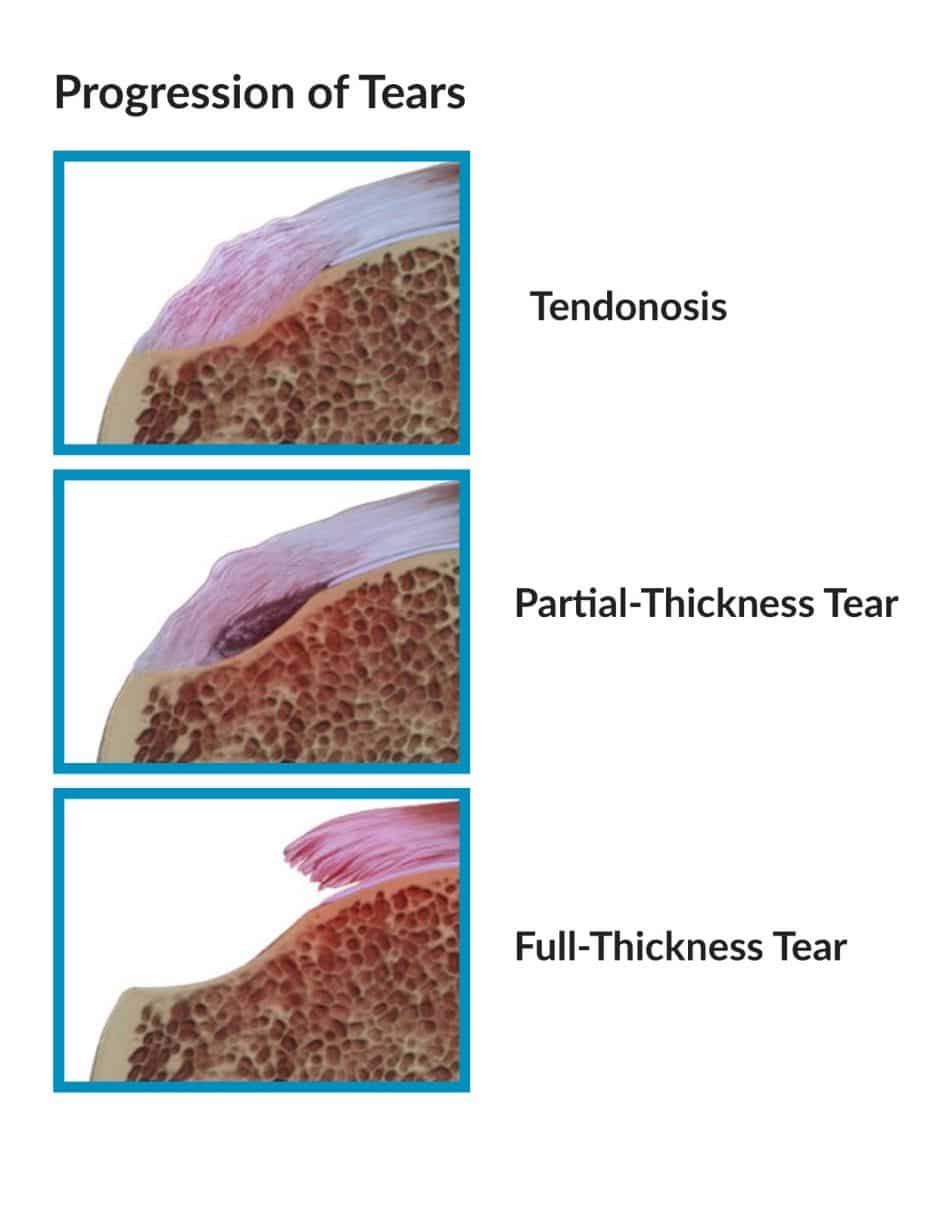 With time, sometimes with usual activities, sometimes with trauma, our tissues wear out, degenerate or tear. The vast majority of rotator cuff tears that we see in the office are attributed to attrition. Your tissues just wore out. Think of your favorite pair of blue jeans that you’ve had since high school if you could still fit in them that — think about the knees on the front of your jeans that that denim just wore out one day. You felt a breeze and looked down and there was a hole there. A portion of your rotator cuff tissue is not very different than that. It goes through a process of degeneration or something we call tendinosis which you can look up on my website. Tendinosis can progress from degeneration to fraying of the surface to a partial tear to a full-thickness tear where a portion of the tendon has detached from the bone.
With time, sometimes with usual activities, sometimes with trauma, our tissues wear out, degenerate or tear. The vast majority of rotator cuff tears that we see in the office are attributed to attrition. Your tissues just wore out. Think of your favorite pair of blue jeans that you’ve had since high school if you could still fit in them that — think about the knees on the front of your jeans that that denim just wore out one day. You felt a breeze and looked down and there was a hole there. A portion of your rotator cuff tissue is not very different than that. It goes through a process of degeneration or something we call tendinosis which you can look up on my website. Tendinosis can progress from degeneration to fraying of the surface to a partial tear to a full-thickness tear where a portion of the tendon has detached from the bone.
[hr]
Traumatic rotator cuff tears versus degenerative rotator cuff tears
There are also situations where you have a normal rotator cuff or a cuff with slight degeneration. You go outside. You play sports. You get tackled and knocked down or you slipped on the ice and fall on that shoulder or as you’re falling you reach for something to hold onto it and you yank your shoulder. Those situations can cause acute traumatic ruptures of the rotator cuff. Is there a difference between attritional and traumatic rotator cuff tears? Absolutely.
Most of us, and I mean academic physicians, believe that attritional rotator cuff tears can be managed in the majority of situations – non-operatively (without surgery). That means with physical therapy or doing nothing if doesn’t bother you too much, occasional injections, etc. If those non-operative modalities are unsuccessful in alleviating your pain AND you have significant pain with use or severe pain at night when you’re trying to sleep, then surgery is an option. But it is YOUR decision. Some tears will grow in size with time. So even if your tear feels better after therapy, you should see your surgeon every 4-6 months for a follow-up to see if the tear has become larger.
Acute or traumatic rotator cuff tears are a different story. Those should generally be repaired. (Again, not all acute tears need surgery and once again, my disclaimer applies and this is not medical advice. You should talk to your orthopedist.) But if you slip and fall and tear your rotator cuff, the likelihood of it being a large tear is fairly high. Those rotator cuff tears have a very good chance of healing after surgery. Should acute rotator cuff tears be fixed sooner rather than later? Yes.
[hr]
Can I delay my rotator cuff surgery?
Yes, assuming you understand the implications of that decision. A few issues to consider.
(1) Retraction. The rotator cuff is like a loaded rubber band, all right? Imagine a rubber band between my two fingers. I release it on one end. What’s gonna happen? It’s gonna shoot over towards the other finger. The muscle is no different. If the rotator cuff retracts or pulls far enough away from the bone, it will make the repair difficult and the likelihood of a successful repair when all is said and done much lower.
The other issue with waiting: Fatty atrophy. Atrophy is simply put — picture a leg that goes into a cast. You take the cast off in four weeks and that leg has shrunk. What has happened? The muscles have atrophied or become smaller. What happens with rotator cuff muscles that are no longer attached to the bone? The body changes the muscle to fat. It’s very cruel because if you re-establish continuity of the tendon, it doesn’t turn the fat back into muscle. So if you wait on a large, retracted, acute rotator cuff tear and that tissue turns to fat, then it doesn’t matter if you get it fixed later, because you’re fixing a piece of fat and it no longer functions as a muscle.
[hr]
Night Pain and Rotator Cuff Tears
Most patients with rotator cuff tears simply have pain. A few may have weakness and loss of motion as well. Rotator cuff pain can be activity related — such as trying to reach overhead: trying to wash your hair; for women, trying to put on a bra; for men, trying to put on a belt, or even trying to reach back and pull something out of the backseat of your car.
What brings the majority of patients into an office for small rotator cuff tears? Night pain. You can’t get comfortable at night or you’re waking up at night. Larger rotator cuff tears that encompass at least one or two complete tendons — will complain of weakness. They simply can’t lift the arm up or if they do, they can’t lift it far.
It will take an examination by an orthopedist and perhaps an ultrasound or an MRI to determine the actual size of the tear. X-rays may be useful to reveal changes that we can see in the bone that are secondary to rotator cuff disease as well.
So, bottom line take-home message:
Do all rotator cuff tears need to be “fixed”?
The answer is no. You can go much slower on the small attritional rotator cuff tears where the tissue simply wore out and try a course of therapy, injections, etc., However, we need to consider being much more aggressive with large acute traumatic tears after a significant incident or traumatic event.
We would love to see you if you have any lingering questions about your rotator cuff or shoulder injury:

Any questions? Please feel free to post them in the comments.
Remember, this for informational purposes and is not medical advice. Evidence changes frequently which makes some of these comments out-dated in the future and since it is a transcription I will not change them.











Thank you for the informative web page…. The reason I am concerned about rotator cuff injuries is because I believe I have injured mine. I have twisted my arm while sleeping around 4 months ago. Since then the healing has been slow and jus recently I reinjured it tiring to catch myself from falling over backwards in a chair. Since I first injured it, it never really healed all the way. I would have to limit my mobility when reaching up in the air upper arm abducted half way, lower arm bent upwards in a 90 degree angle or reaching to get something from the back seat of my car. Even though it didn’t heal in 4 months it seemed that it given time it might get better because it felt like it was progressing very very slowly. But now, I am very concerned that maybe it won’t heal by itself and my time might be running out for a successful treatment. Could you please tell me if after 4 months there still is a good possibility to salvage the tendon?…………
Lots of appreciation David Dayan
I took quite a fall and was diagnosed as having a rotator cuff tear based on x-rays showing the shoulder high in the socket and the fact the pain and weakness (I can’t move my arm away from my body much at all. It is OK if someone else moves it, but sometimes it feels like the bones rotate and then it hurts a lot to get it back down until they shift out of the way.) The doctor wants to wait two weeks before doing anything else. I’m OK with that, but when I read about muscle atrophy and such, I worry about how long that actually takes. Is that too long, or is it OK to just wait the two weeks and then get a referral if the problem continues?
Massive rotator cuff tears should be evaluated and managed in a “timely” manner. A few weeks wait should not matter… but the tear is not going to heal itself during that time. The high riding head is a concern. That might mean there was a tear present before your fall which will complicate the treatment decision.
Good Luck
Howard Luks
I fell running two days ago – I tucked and rolled and landed mostly on my right shoulder. The deltoid is very tender to the touch and I have pain when raising my arm above shoulder height. I am very active and fear I have an acute rotator cuff tear. I have a fairly high tolerance to pain, but I don’t want to ignore this if it will not heal on its own. My plan is RICE and NSAIDS for a week and see how it feels. How much longer should I wait after that to see an orthopedist? Does this sound like it will heal on its own or should I get it looked at ASAP? Thank you very much for your help.
Emily … with an injury mechanism like that you should see someone sooner. Just to make sure nothing is broken or torn. Good Luck!
Hi. I fell climbing almost 2 years ago and since then my shoulder has been weak, with a nagging pain, it pops on movement and even looks like it’s pushed forward and generally feels like it’s not sitting right. I saw a Physio soon after the injury for some months, but nothing helped and I felt like it was worse after. I stopped seeing the Physio and hoped that rest would improve things, and it did for a while, but over the last 6 months it has been getting progressively worse. I have spoken to a dr who has referred me on to a specialist, but my question to you, as I am concerned, do you think if there is a tear to the rotator cuff that is could have turned to fat already? My concern is that is will never be fixed now. What are the options if surgery is pointless? Is it likely I will get strength back in my shoulder again?
Many thanks,
Em
Sounds like an MRI is warranted. That will show if a tear exists, and if it does, it will show if their is any fatty infiltration or atrophy. Feel free to stop back after your study is completed.
Dr. Luks,
I really would appreciate your help in deciphering the results of the MRI from my right shoulder. I really did not get an understanding of it as it was relayed to me. Not having a full understanding of the predicament or how to move towards a resolution is really frustrating. To provide background, back in the last week of April of this year I sustained some injury to my right shoulder during whitewater rafting. A week prior to this I was so excited at the opportunity to get back into my physique training after taking time off to concentrate on finishing an advanced degree! I finally went to see an orthopedic surgeon in July. I am 35 by the way.
The highlights of this report (about 6 weeks ago) are as follows:
1) supraspinatus demonstrates mild bursal surface fraying and mild tendinosis with no full thickness or significant partial thickness tear.
2) infraspinatus shows mild bursal surface fraying with no tendon tear.
3)subscapularis demonstrates insertional tear (approx. 1 cm) at the superior facet of greater tuberosity
4) rotator cuff musculature is normal in appearance
5)mild hypertrophy of the AC joint– type 2 acromial contour is demonstrated.’
6) Localized fatty infiltration is demonstrated at the musculotendinous junction (no edema in this region)
Can you explain this on a “layman’s” level and what it means with regard to moving forward as well as getting back into meaningful resistance training without fear of causing irreparable damage?
Sincerely
I’ll try my best :-)
This is a very “routine” set of findings for a shoulder MRI in an active individual. Like I say in many posts sometimes our tissues simply wear out and show their age. It’s like your fav pair of blue jeans. The fabric lightens, frays, then might even begin to tear. That is what the process of tendinosis is. It is a common degenerative change that occurs in tendons throughout our body. It can be the cause of pain too. Tennis elbow is tendinosis of the elbow, Achilles pain is usually due to tendinosis as well. A jumpers knee — or patella tendinosis occurs in basketball players of all ages.
These are very common findings for a shoulder MRI and usually can be treated with physical therapy. Tendinosis can progress… but resting or even laying in bed can lead to progression as well. These findings would NOT lead the majority of shoulder docs to recommend eliminating activities or changing your active lifestyle.
Hope this helps!
Howard Luks