Shoulder Pain
Rotator cuff injuries are very common. Over the age of 30, the rotator cuff is responsible for the shoulder pain that most of us experience.
Determining the cause of your shoulder pain and determining what the actual pain generator is in your shoulder is our job as a shoulder specialist. Until we know why your shoulder hurts, it’s hard to start a treatment plan.
The most common causes of shoulder pain will vary by age, your activities and whether or not you have suffered any trauma. Rotator cuff injuries are only one of the many sources of pain in the shoulder.
Shoulder Pain by Age
Children and teens tend to have overuse tendonitis … or shoulder dislocations and labral tears due to trauma or sports injuries.
“Young” Adults and “weekend warriors” tend to have shoulder pain due to rotator cuff injuries or rotator cuff changes (tendinosis). Tendinosis and other degenerative changes within the rotator cuff occur as a result of genetics, activities, and aging. In this age group rotator cuff injuries may also occur as a result of trauma or injuries, but rotator cuff degeneration is the most common reason we see you in our office.
Seniors tend to have shoulder pain due to arthritis, loss of cartilage, and small, medium or even very large chronic (old) rotator cuff tears from a lifetime of wear and tear. Sometimes the torn rotator cuff tendon will upset the tissues around the tendon and cause a bursitis. This secondary bursitis is a common cause of pain and discomfort.
The Most Common Cause of Shoulder Pain In Adults
In adults, the most common source of shoulder pain are injuries of the rotator cuff … a series of 4 small muscles that coordinate the motion of the shoulder. This post on what is the rotator cuff will clear many questions about its structure and function. Again … The most common cause of shoulder pain is actually rotator cuff tendinosis, or partial tears of the rotator cuff.
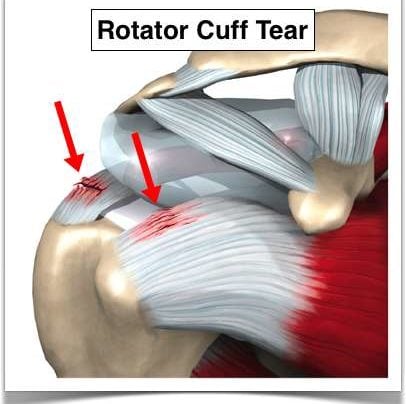
Rotator Cuff Tears
Let’s talk about rotator cuff tears (injuries). A lot of people say rotator cup tears— but it’s actually rotator cuff (C-U-F-F) tears.
What is the rotator cuff?

The rotator cuff are four small muscles located around your shoulder and they link together to form a cuff that literally sits on top of the top of your humerus. It’s beneath your deltoid so you can’t actually see or feel the rotator cuff. The purpose of the rotator cuff is to take all the energy or strength derived from the larger muscles such as the deltoid or latissimus or your pec major or your chest muscles and turn it into meaningful motion or rotational motion so you can move the arm out, move the arm up, any way you want to place it in space.
[hr]
What causes rotator cuff tears?
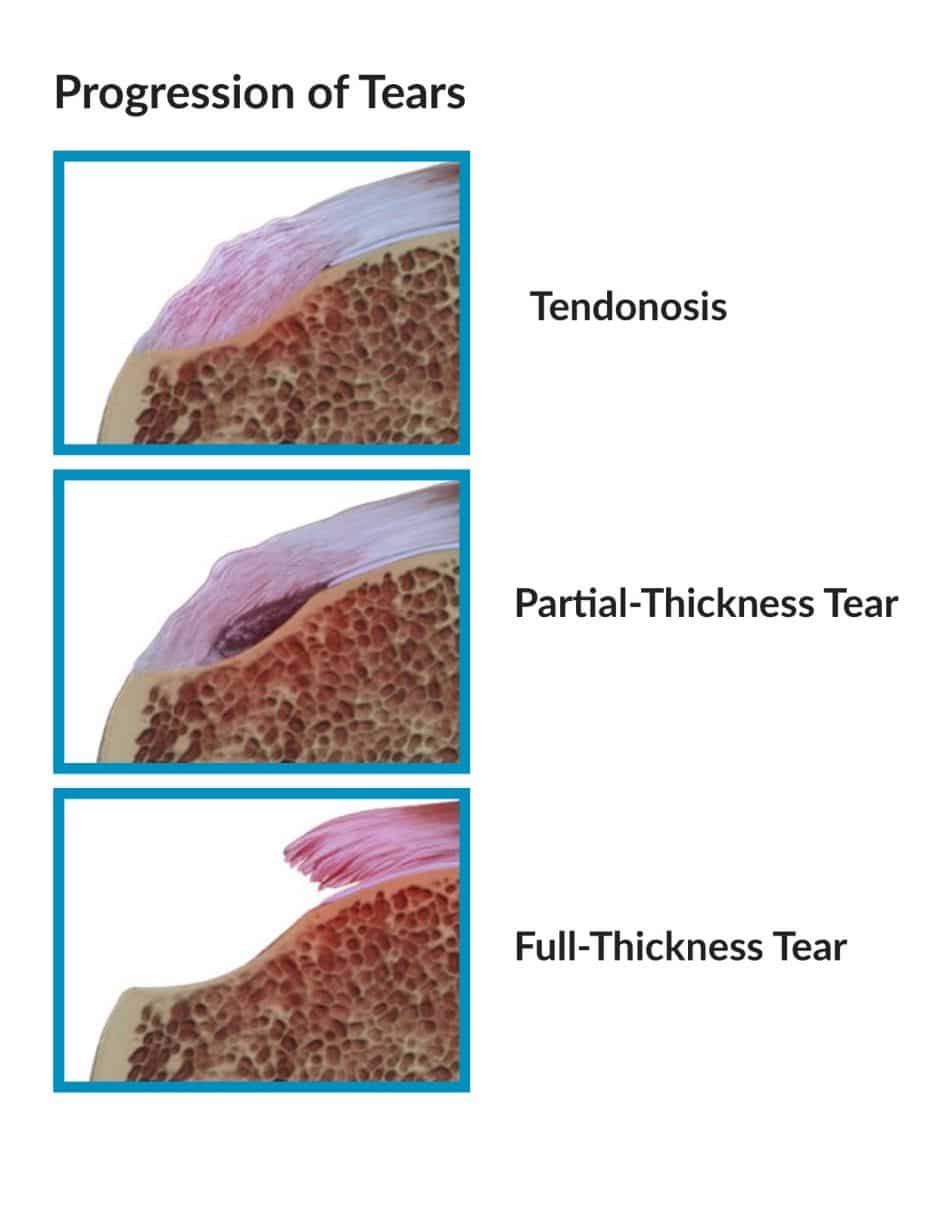 With time, sometimes with usual activities, sometimes with trauma, our tissues wear out, degenerate or tear. The vast majority of rotator cuff tears that we see in the office are attributed to attrition. Your tissues just wore out. Think of your favorite pair of blue jeans that you’ve had since high school if you could still fit in them that — think about the knees on the front of your jeans that that denim just wore out one day. You felt a breeze and looked down and there was a hole there. A portion of your rotator cuff tissue is not very different than that. It goes through a process of degeneration or something we call tendinosis which you can look up on my website. Tendinosis can progress from degeneration to fraying of the surface to a partial tear to a full-thickness tear where a portion of the tendon has detached from the bone.
With time, sometimes with usual activities, sometimes with trauma, our tissues wear out, degenerate or tear. The vast majority of rotator cuff tears that we see in the office are attributed to attrition. Your tissues just wore out. Think of your favorite pair of blue jeans that you’ve had since high school if you could still fit in them that — think about the knees on the front of your jeans that that denim just wore out one day. You felt a breeze and looked down and there was a hole there. A portion of your rotator cuff tissue is not very different than that. It goes through a process of degeneration or something we call tendinosis which you can look up on my website. Tendinosis can progress from degeneration to fraying of the surface to a partial tear to a full-thickness tear where a portion of the tendon has detached from the bone.
[hr]
Traumatic rotator cuff tears versus degenerative rotator cuff tears
There are also situations where you have a normal rotator cuff or a cuff with slight degeneration. You go outside. You play sports. You get tackled and knocked down or you slipped on the ice and fall on that shoulder or as you’re falling you reach for something to hold onto it and you yank your shoulder. Those situations can cause acute traumatic ruptures of the rotator cuff. Is there a difference between attritional and traumatic rotator cuff tears? Absolutely.
Most of us, and I mean academic physicians, believe that attritional rotator cuff tears can be managed in the majority of situations – non-operatively (without surgery). That means with physical therapy or doing nothing if doesn’t bother you too much, occasional injections, etc. If those non-operative modalities are unsuccessful in alleviating your pain AND you have significant pain with use or severe pain at night when you’re trying to sleep, then surgery is an option. But it is YOUR decision. Some tears will grow in size with time. So even if your tear feels better after therapy, you should see your surgeon every 4-6 months for a follow-up to see if the tear has become larger.
Acute or traumatic rotator cuff tears are a different story. Those should generally be repaired. (Again, not all acute tears need surgery and once again, my disclaimer applies and this is not medical advice. You should talk to your orthopedist.) But if you slip and fall and tear your rotator cuff, the likelihood of it being a large tear is fairly high. Those rotator cuff tears have a very good chance of healing after surgery. Should acute rotator cuff tears be fixed sooner rather than later? Yes.
[hr]
Can I delay my rotator cuff surgery?
Yes, assuming you understand the implications of that decision. A few issues to consider.
(1) Retraction. The rotator cuff is like a loaded rubber band, all right? Imagine a rubber band between my two fingers. I release it on one end. What’s gonna happen? It’s gonna shoot over towards the other finger. The muscle is no different. If the rotator cuff retracts or pulls far enough away from the bone, it will make the repair difficult and the likelihood of a successful repair when all is said and done much lower.
The other issue with waiting: Fatty atrophy. Atrophy is simply put — picture a leg that goes into a cast. You take the cast off in four weeks and that leg has shrunk. What has happened? The muscles have atrophied or become smaller. What happens with rotator cuff muscles that are no longer attached to the bone? The body changes the muscle to fat. It’s very cruel because if you re-establish continuity of the tendon, it doesn’t turn the fat back into muscle. So if you wait on a large, retracted, acute rotator cuff tear and that tissue turns to fat, then it doesn’t matter if you get it fixed later, because you’re fixing a piece of fat and it no longer functions as a muscle.
[hr]
Night Pain and Rotator Cuff Tears
Most patients with rotator cuff tears simply have pain. A few may have weakness and loss of motion as well. Rotator cuff pain can be activity related — such as trying to reach overhead: trying to wash your hair; for women, trying to put on a bra; for men, trying to put on a belt, or even trying to reach back and pull something out of the backseat of your car.
What brings the majority of patients into an office for small rotator cuff tears? Night pain. You can’t get comfortable at night or you’re waking up at night. Larger rotator cuff tears that encompass at least one or two complete tendons — will complain of weakness. They simply can’t lift the arm up or if they do, they can’t lift it far.
It will take an examination by an orthopedist and perhaps an ultrasound or an MRI to determine the actual size of the tear. X-rays may be useful to reveal changes that we can see in the bone that are secondary to rotator cuff disease as well.
Do you have questions regarding an Orthopedic injury or longevity?
Do you want to talk to an expert who can listen to you for 45-60 minutes and explain the options in detail?
Dr. Howard Luks offers remote guidance sessions to review your X-ray or MRI images and explain your options.
Dr. Luks has also received hundreds of requests for educational sessions on the topics discussed in his book, Longevity Simplified.
So, bottom line take-home message:
Do all rotator cuff tears need to be “fixed”?
The answer is no. You can go much slower on the small attritional rotator cuff tears where the tissue simply wore out and try a course of therapy, injections, etc., However, we need to consider being much more aggressive with large acute traumatic tears after a significant incident or traumatic event.
We would love to see you if you have any lingering questions about your rotator cuff or shoulder injury:

Any questions? Please feel free to post them in the comments.
Remember, this for informational purposes and is not medical advice. Evidence changes frequently which makes some of these comments out-dated in the future and since it is a transcription I will not change them.






James Weir
Dear Dr. Luks, (leaving this comment twice, first time I think was the wrong place. thks)
First a hearty thank you for your site and the blog. Since I have learned that I will likely need surgery on the supraspinatus tendon, I have been reading online about this, and your site has been by far the most helpful.
I will (try to) be brief: 48 male who is very active and an avid swimmer. Four years ago I developed pain in my rt shoulder and saw several Drs and ended up in PT, but after month without success, had an MRI and learned that the supraspinatus tendon had come completely off the bone. Had pain, for a long time, but never terribly intense, and remained active.
More recently, regularly swim long distances (avg 2 miles and i.e. thus far rt shoulder surgery worked) and started to develop some pain a few months back in left. As I continued to swim the pain grew but is very tolerable. To be safe I had 2 MRIs, and the second with ink inserted into the rotator cuff. Results:
Glenoid labrum: Conscious material extending into the super laburm posterior to the biceps anchor compatible with a SLAP lesion.
Supraspinatus tendon: Near full-thickness tear at the footprint of the supraspinatus. with contrast material extending through essentially the full thickness of the tendon, but not entering the subracromial-sub-deltoid bursa. On the sagittal images, the tear measures approx 1.8 cm in anteroposterior diameter, involving most of the supraspinatus footprint. Contrast in is extending deep into the substance of the tendon nearly to the level of the myotendinous junction. Normal ….. muscle belly.
The rest unremarkable
Except: Type II acromion with concave undersurface. No evidence of os acromiale. The AC joint is not widened. (Paraphase here) Relationship of acromion and clavicle is maintained. Trace fluid in acromioclavicular joint. Near joint, near skin surface, small 9 x 4 mm cyst, presumably arising from the AC joint.
Impression: 1. near full thickness tear of supraspinatus, sparing bursal fibers, without contract entering the subacromial-subdeltoid bursa. 2. Type II slap lesion. 3. Small AC joint cyst.
Insurance Codes for surgery for this Sat, June 7, 29827, 29807, 23430, 29826.
fyi I still swim regularly without much pain, but perhaps slowly increasing. I am about to lose a job by the end of June and thus insurance. My primary concern is that the tendon is likely to come off completely and than require surgery.
Thanks so much for bothering to read. Do you agree surgery is necessary? Regards and appreciation for this service you provide. Dr. Jimmy Weir – anthropologist.
James… I think you should seriously consider another opinion or two. SLAP lesion repairs are rarely necessary at our age… and even if the surgeon feels it may be the source of your pain, a repair is not the recommended procedure for it. In addition, surgery on partial thickness tears is recommended more as a quality of life issue than anything else. I would take your time, talk to your doctor and perhaps another shoulder specialist.
Good Luck
Howard Luks
Dana
Dr. Luks,
Not sure how to get to Dr. Luks, but I hope he reads this…..I had a rotator cuff repair in August of 2013 and 4 months later could not raise my arm at all. An MRI showed I had a tear again, the doctor said it looked like it wasn’t a fast tare but a slippage. He did another rotator cuff repair and said he put so many anchors in it that my shoulder will never tear. Again at 5 months I can not rise my shoulder. He wants to do a nerve study of my shoulder and a neck MRI. I really want an MRI of my shoulder. What do you think?
Dana …
Without examining you I can not really comment on what is wrong. Weakness can be due to a massive tear of the rotator cuff or a nerve that’s not functioning well.
You can always seek another opinion.
Good Luck to you!
/hjl
Charles
..
Dr. Lusk.
I am a retired on disability 65 year old Male with past history of knee surgery in 1971 and fusions both in the cervical and lumbar spine regions in 1994. Since there was nerve damage associated with the spinal fusions, I know I have unexplained, random “pains”. No known trauma to shoulder. 3/13 I began feeling pain when raising RT arm and problems sleeping. Saw Pain Management Doctor on 5/30/13, the exam on a Fluoroscope reveled a small Labral Tear of the right RC. Received cortisone injection. Was told if the condition continued to see an Orthopedic Surgeon. Pain return, on 11/11/13 saw an Orthopedic Surgeon. After physical exam, he did a shoulder x-ray and injected another shot of cortisone and set up an appointment for an MRI. The MRI showed:
1. Full thickness tear distal supraspinatus with 2.2cm proximal retraction.
2: Articular surface partial tearing critical zone anterior infraspinatus fibers.
3: Type III acromion with anterior spurring.
4: Degenerative chance at the AC joint with joint effusion and undersurface osteophyte formation.
5: Diffuse irregularity of the glenoid labrum suggests chronic degenerative tearing.”
The Doctor recommended RC surgery, but he only does the “open method”. I asked if Arthroscopic surgery was a option, he referred me to one of his younger associates. He also recommended I have surgery.
I live alone, do not have anyone close that can help me after the surgery. I was told Home PT and limited Home Health care services are available. I am worried the lack of other “help” will be a major drawback.
In your opinion, with this limited information, should I get a Second Opinion? Is there a possibility surgical repair may not be the only answer?
Thank you for your blog and sharing your training and experience.
Thanks for stopping.. and thank you very much for the kind comments about the blog! The American Academy of Orthopedic Surgeons recently published a guideline approach to rotator cuff tears… http://www.aaos.org/news/aaosnow/oct13/cover1.asp It is worth reviewing. It clearly shows that a trial of non-surgical treatment with physical therapy, injections, oral medications etc is very much worthwhile before considering surgery. Having surgery while living alone is very very difficult because of the limitations we impose on your activity. It can be done.. but it’s not easy.
Good Luck
Howard Luks
Charles
Dr. Lusk,
I greatly appreciate your thought and response to my questions. Both Doctors are members of AAOS. To my knowledge, they did not ask the questions to evaluate my condition completely using the new AAOS AUC. I in no way would ever disrespect a Doctor with an attitude questioning their ability. In your opinion, would I be out of line to make another appointment and simply ask if they use the new AUC? I do have other questions I need to ask before treatment continues.
Thanks,
Charles
Charles…
Physicians are well aware that 80+% of patients are researching their diseases, injuries, doctors, etc. If they are not willing to entertain a patient’s questions about a procedure or treatment recommendation then it may be time to seek a another opinion. You would not be insulting me if you asked me what my thoughts were on the new treatment recommendations put forth by the AAOS.
Good Luck
Howard Luks
Ivan Mendez
Dr Lusk , my MRI shows partial tears of the supraspinatus and a full tear of the subscapularis with dislocation of the bicep . Can these be rehabilitated without surgery ?
Many thanks,
IM
The Subscapularis is considered by most to be the most crucial rotator cuff muscle. In addition, when it tears, the biceps will usually dislocate. The torn tendon, if complete will produce significant shoulder dysfunction… and the biceps will produce ongoing pain. This scenario is usually best treated surgically.
Scott Ellis
Dr. Luks,
I really would appreciate your help in deciphering the results of the MRI from my right shoulder. I really did not get an understanding of it as it was relayed to me. Not having a full understanding of the predicament or how to move towards a resolution is really frustrating. To provide background, back in the last week of April of this year I sustained some injury to my right shoulder during whitewater rafting. A week prior to this I was so excited at the opportunity to get back into my physique training after taking time off to concentrate on finishing an advanced degree! I finally went to see an orthopedic surgeon in July. I am 35 by the way.
The highlights of this report (about 6 weeks ago) are as follows:
1) supraspinatus demonstrates mild bursal surface fraying and mild tendinosis with no full thickness or significant partial thickness tear.
2) infraspinatus shows mild bursal surface fraying with no tendon tear.
3)subscapularis demonstrates insertional tear (approx. 1 cm) at the superior facet of greater tuberosity
4) rotator cuff musculature is normal in appearance
5)mild hypertrophy of the AC joint– type 2 acromial contour is demonstrated.’
6) Localized fatty infiltration is demonstrated at the musculotendinous junction (no edema in this region)
Can you explain this on a “layman’s” level and what it means with regard to moving forward as well as getting back into meaningful resistance training without fear of causing irreparable damage?
Sincerely
I’ll try my best :-)
This is a very “routine” set of findings for a shoulder MRI in an active individual. Like I say in many posts sometimes our tissues simply wear out and show their age. It’s like your fav pair of blue jeans. The fabric lightens, frays, then might even begin to tear. That is what the process of tendinosis is. It is a common degenerative change that occurs in tendons throughout our body. It can be the cause of pain too. Tennis elbow is tendinosis of the elbow, Achilles pain is usually due to tendinosis as well. A jumpers knee — or patella tendinosis occurs in basketball players of all ages.
These are very common findings for a shoulder MRI and usually can be treated with physical therapy. Tendinosis can progress… but resting or even laying in bed can lead to progression as well. These findings would NOT lead the majority of shoulder docs to recommend eliminating activities or changing your active lifestyle.
Hope this helps!
Howard Luks
Em
Hi. I fell climbing almost 2 years ago and since then my shoulder has been weak, with a nagging pain, it pops on movement and even looks like it’s pushed forward and generally feels like it’s not sitting right. I saw a Physio soon after the injury for some months, but nothing helped and I felt like it was worse after. I stopped seeing the Physio and hoped that rest would improve things, and it did for a while, but over the last 6 months it has been getting progressively worse. I have spoken to a dr who has referred me on to a specialist, but my question to you, as I am concerned, do you think if there is a tear to the rotator cuff that is could have turned to fat already? My concern is that is will never be fixed now. What are the options if surgery is pointless? Is it likely I will get strength back in my shoulder again?
Many thanks,
Em
Sounds like an MRI is warranted. That will show if a tear exists, and if it does, it will show if their is any fatty infiltration or atrophy. Feel free to stop back after your study is completed.
Emily
I fell running two days ago – I tucked and rolled and landed mostly on my right shoulder. The deltoid is very tender to the touch and I have pain when raising my arm above shoulder height. I am very active and fear I have an acute rotator cuff tear. I have a fairly high tolerance to pain, but I don’t want to ignore this if it will not heal on its own. My plan is RICE and NSAIDS for a week and see how it feels. How much longer should I wait after that to see an orthopedist? Does this sound like it will heal on its own or should I get it looked at ASAP? Thank you very much for your help.
Emily … with an injury mechanism like that you should see someone sooner. Just to make sure nothing is broken or torn. Good Luck!
Dana
I took quite a fall and was diagnosed as having a rotator cuff tear based on x-rays showing the shoulder high in the socket and the fact the pain and weakness (I can’t move my arm away from my body much at all. It is OK if someone else moves it, but sometimes it feels like the bones rotate and then it hurts a lot to get it back down until they shift out of the way.) The doctor wants to wait two weeks before doing anything else. I’m OK with that, but when I read about muscle atrophy and such, I worry about how long that actually takes. Is that too long, or is it OK to just wait the two weeks and then get a referral if the problem continues?
Massive rotator cuff tears should be evaluated and managed in a “timely” manner. A few weeks wait should not matter… but the tear is not going to heal itself during that time. The high riding head is a concern. That might mean there was a tear present before your fall which will complicate the treatment decision.
Good Luck
Howard Luks
David
Thank you for the informative web page…. The reason I am concerned about rotator cuff injuries is because I believe I have injured mine. I have twisted my arm while sleeping around 4 months ago. Since then the healing has been slow and jus recently I reinjured it tiring to catch myself from falling over backwards in a chair. Since I first injured it, it never really healed all the way. I would have to limit my mobility when reaching up in the air upper arm abducted half way, lower arm bent upwards in a 90 degree angle or reaching to get something from the back seat of my car. Even though it didn’t heal in 4 months it seemed that it given time it might get better because it felt like it was progressing very very slowly. But now, I am very concerned that maybe it won’t heal by itself and my time might be running out for a successful treatment. Could you please tell me if after 4 months there still is a good possibility to salvage the tendon?…………
Lots of appreciation David Dayan
Cynthia
Hi Dr. Luks, I had an MRI back in August because my orthopedic surgeon thought I might have a rotator cuff tear in my right shoulder. I am 64 and my physician believes it was probably from deteriozation. I had an MRI and it showed that I have a full-thickness inseritonal posterior supraspinatus tendon tear measuring about 1.2 cm in AP dimension. There is approximtely 2 cm retraction of supraspinatus tendon and appears to be “scar down to coracoacromial ligament.” “. . no signifcant surprasphnatus muscle volume loss or fatty infiltration.” “There are mild osteoarthric changes of acromioclavicular joint with capsular hypertrophy. There is mild subacromial subdeltoid bursitis, thickening of coracoarcromial ligament and interior acromion enthesophyte . .” I have been told that the tendon is detached from the bone and the only way to fix this would be with surgery. I don’t have a lot of pain and a lot of time I have no pain. I can lift my arrm over my head without pain and I sleep well at night; however if I lie on my right side there is some tenderness. It really only bothers me during the weekend when I do a lot of cleaning around the house but the pain is usually gone the next day. I have seen 2 doctors and both think that surgery is the only way to fix my shoulder since it is a full-thickness tear and detached from the bone. My doctor is concerned if I don’t have surgery I will have problems in the future with arthritis, spurs, and if I wait too long he might not be able to perform the surgery. Do you think surgery is warranted and if I don’t have surgery what do you think my consequences will be? Since I don’t have a lot of pain and I can function well, it is hard from me to make a decison about surgery, which will cause me to be in more pain and extensive recovery time.
I look forward to hearing what you think — this is a tough decision for me to make.
Thank you Cynthia
Cynthia… The scientific literature shows that most of the “attritional” or degenerative tears (our tissues simply wear out) do not get bigger with time. Only certain tears do. Many many people your age have these small degenerative tears and do not even know it. Most of the time it is the bursitis which is bothering you and not the tear itself. As physicians we need to treat the patient and not their MRI findings. While I am prohibited from offering you specific treatment advice the recommendations are pretty clear. Many if not most of these degenerative tears do not need to be fixed unless you have a quality of life issue, and significant pain which drives you to consider surgery. If you have little pain and your quality of life is not affected it is a well accepted treatment to simply watch you and perhaps re-image the tear in 6-12 months to look for signs of progression.
A second opinion or further search of the science of the treatment of rotator cuff tears might by worthwhile.
Try the AAOS.org site as well as others which can help you make the right decision for you.
Good luck.
Howard Luks
Linda
Dear Dr. Luks, I plan on seeing a sports medicine doc asap but it is killing me: what the heck happened: I am an active 49 year old female and have been shooting archery for a year. 2 weeks ago I turned up the poundage on my bow and could feel the joint strain but I kept shooting anyway ( yes dumb). Then 2 nights ago I awoke with horrible shoulder pain. It has not gone away and nsaid’s don’t seem to touch it. Nothing does: laser, acupuncture, ultrasound, dmso, all of it seems ineffective. I am wondering, what the cause could be? The pain is severe, unrelenting and non-responsive to any treatment. I am totally incapacitated in that arm and miserable too. Any advise would be appreciated, Thanks, Linda R DVM
Most common cause of pain in this situation is rotator cuff tendinosis or perhaps even a partial tear… very very common issue… and the night pain really changes people :-(
Good luck!
Keep us informed.
Howard Luks MD
Hawthorne NY
Danielle Duggar
Hi, I’m 28 years old and had 2 full thickness tears due to impingement syndrome from whiplash. I had the right cuff repaired in 2008 and now they’ve discovered the left has a full thickness tear as well. My problem is this; I have a 21 month old son and no family or friends nearby to care for the child post surgery. I need to postpone surgery until I no longer need to lift my son in and out of his many apparati, ie., high hair, car seat, bath tub, changing table, crib. I’d prefer to wait until he is in Kindergarten so I could be at home resting, healing and going to PT while he is in school without having to care for him as well or bring him with me. I don’t know however, if I can wait that long. My pain is sometimes intolerable and I’m afraid of further damage that can occur. Do you have any advice or recommendations for me?
Also, most of my pain is deep in my back right underneath my shoulder blade on the affected shoulder side. Is this common? This pain is constant and ranges from a (4-6) on the pain scale . Besides ice, heat, and Ibuprophin what can be done to live with this pain?
gayle
shoulder hurt in fall…mra of shoulder said 50%thickness tear ifndistal posterior supraspinatus tendon.
I have only raised my arm above my head twice in six months. Should I agree to have a repair of the tendon or just try to exercise and stretch shoulder and arm? Will the tear enlargen if it is not addressed quickly. My shoulder hikes up when I lift my arm to the side. If I have the repair, will I be able to lift my arm above my head and reach behind my back?
Gayle… partial thickness rotator cuff tears, are not in and of themselves a reason to consider surgery. Many many many people over 40 have partial tear and don’t even know it. That said, there are occassions when surgery is an option if non-surgical measures such as physical therapy, injections, moist heat, etc have not been successful at improving your quality of life. Your decision should be based on your quality of life and lack of improvement with non-surgical rotator cuff injury management …. there is no literature that shows that tears will always become larger. So throw the idea of what if surgery out the window :-)
Good Luck and keep us informed.
https://www.howardluksmd.com/education/common-injuries/rotator-cuff-tears-shoulder-injury/
Howard Luks
Orthopedic Surgery – Rotator Cuff Injury
Westchester County, NY
dana carnes
How long does it take for for your joints to turn to fatty infilitration after a trauma? Dana
Dana… the joint itself doesn’t undergo fatty infiltration, the rotator cuff muscles do, after they have torn from the bone. Usually it takes a complete tear of the entire muscle to lead to fatty degeneration, however, many of us have seen fatty degeneration occur with smaller tears too. Bottom line, it is unpredictable, but the larger the tear, the more likely it is to develop fatty atrophy or degeneration.
sandra davenport
I have a complinet rotator cuff tear,this happen febuary10th. had MRI in March ,having surgery June 9. will my joint already be turn into fat, and can’t be fixed
Your surgeon should be able to tell you by looking at the MRI. The radiologist should have also made a comment about whether or not there was atrophy or “fatty infiltration”.
Eric
Hi doc I had a traumatic injury at work(firefighter) one ultrasound showed a 1.5 cm tear with bursal fluid and bicep tendosynovitis. Another ultrasound(different tech) saw no defect. I am experiencing a deep seated ache and lack of strength. There is Definetely something going on in there. Would an MRI be the test of choice? If a partial tear is found would surgery be recommended due to my occupation? any advice is much appreciated.
Eric,
The US is only as useful as the tech performing it and radiologist reading it. In general, an US can be just as useful as an MRI to visualize the rotator cuff. If discrepancies exist an MRI might be useful to better delineate what the status of your rotator cuff is.
In general, the first line of treatment of partial thickness tears is not surgical. Physical therapy, injections, etc can return most patients to full function.
Some partial tear can progress to full thickness tears, but *we* are not able to predict whose tear might progress and whose tear will not. The academic shoulder community does not talk about surgery on partial tears to prevent progression to full tears. *We* only consider surgery on patients with partial thickness tears once they have failed a thorough course of non-operative treatment. Unfortunately, both non-surgical and surgical management of rotator cuff disorders can require many weeks to many months to recover from.
Hope this helps.
Debbie Adams
Debbie Adams [email protected]
52 years old with severe night pain from left shoulder. Had right rotator cuff repaired Feb/2010
Mri ofr left shoulder shows severe totator cuff tendinosis small anterior thickness tear. The MRI also shows abnormal bone marrow at thelevel of the humeral shaft with relative decrease signal on t1 and increased signal on fat supppressed T2 images Appearence may be related to reconverted hemopoittic bone marrow secondary to anemia, hematological disorders of it’s marrow inflitration related to neoplastic process. Correlate clinically and further evaluation recommended. received one steroid shoit last week. Starting PT today. Ortho has nit spoken to me about the marrow changes. I am a smoker so there is a possiblility this is all related to my smoking. Can you further explain what theissue may be and do I need to worry about a cancer diagnosis.
Thx for the post. Suggest you talk with your primary care doctor before doing anything else re: the shoulder. Need to treat WHOLE patient… not just the rotator cuff. “Red marrow conversion” not very common in humerus. In general, atypical edema patterns shoulder be evaluated.
Sandra
Dr. Howard J. Luks, MD,
How common is tendon tears with people with RA ?
Thanks for any info you can share.
Sandra Van Zandt
In general you run the same risk as the general population.
mimi
I like the demeanor of your responses. I am 64, fell on my shoulder (bowling) in March, had x-ray to determine any fx., told “if not better, in two weeks”, see an ortho. On exam, sent for MRI, after two weeks, had to call 6x for result.. (Crystal Run Health Care, Middletown, NY) nurse tells me “hi-grade-rotator cuff tear. It’s been approx. 50days from injury, too late for repair work?? (¬ there)
mimi
Hi doc, glad your’e there. I’m 64 yr. old fem. fell bowling end of Feb., on my right upper arm. I’ve had exam, x-ray, & MRI. Only know report read ‘hi-grade rotator cuff tear’, still have not heard from Dr.’s regarding course of treatment. Has too much time gone by for surgical intervention? Pain on certain movements. It took a 1 1/2 weeks to find out this much.
Mimi… I’m sorry you had to wait so long to hear of your results. There are many many variables we need to consider when contemplating a rotator cuff repair. As I always say, we treat patients, and not MRI findings. Before offering an opinion about the repairability of a tear, or even if a tear needs surgery I like to look at the report, possibly the films, talk to the patient and examine the patient. Then we have a complete picture and we can talk about the options available.
Howard Luks
Thanks Eric… hope all is well.
Eric Weisler
As always, well said. You have a gift for speaking to patients and not at them. Thanks.