What is the cause of atherosclerotic heart disease? I reviewed this article for the sole purpose of improving my understanding of the etiology or cause of clinically relevant heart disease. Many people fail to understand how atherosclerosis forms; they think it is a disease of adulthood. They do not understand the importance of time and how a lifetime of exposure to cholesterol and the various lipoproteins (like LDL) is the driving factor that ends in a heart attack later in life. What we eat during our formative years impacts our risk for a heart attack 5 decades later. Should we be treating these LDL and ApoB levels earlier? Can heart disease be eradicated if we do? This paper raises interesting and important questions.
What causes Atherosclerotic heart disease, and how young should we start addressing it?
If you are active online, you may have read that some people believe that your LDL cholesterol levels don’t matter as much as we previously thought. First… that has not been proven, and that is not what the cardiology community thinks. Are you ready to roll the dice on the biggest wager of your life and not pay attention to your LDL or ApoB levels? I’m not. Read on, please… this is important.
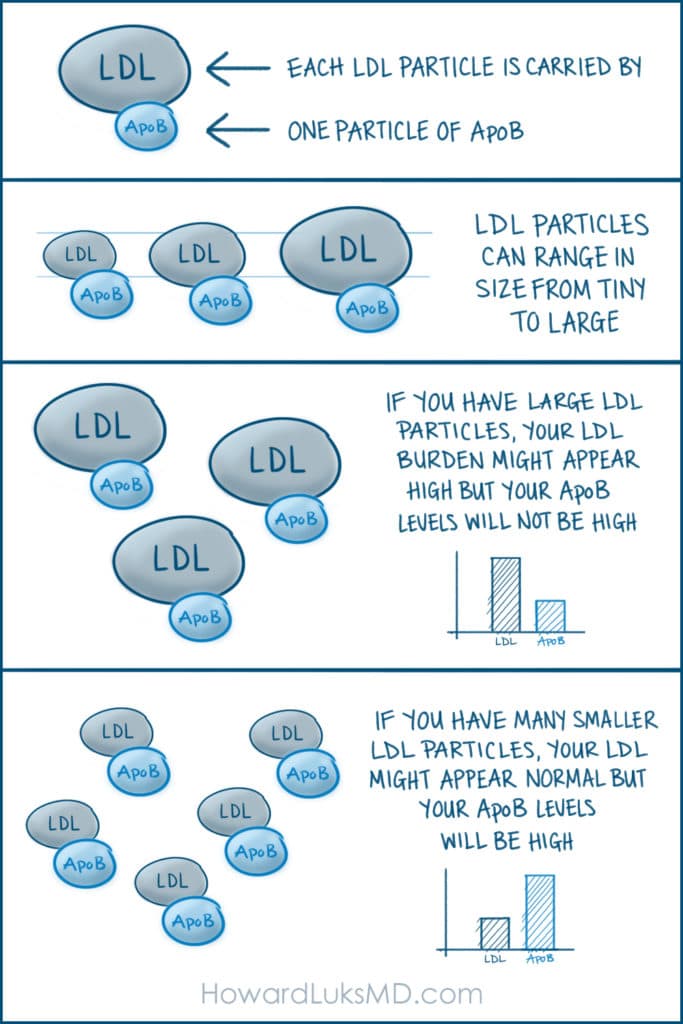
Each LDL particle is carried around in the blood by one particle of Apolipoprotein B (ApoB). Since LDL particles can be large, small, or even tiny remnants, it appears that your ApoB levels are the more important determinant of your overall risk of atherosclerotic heart disease. That’s because if you have large LDL particles, your LDL burden might appear high, but your particle number, which we determine by your ApoB will not be large. On the contrary, if you have many smaller LDL particles, your LDL level might be normal, but your ApoB will be high. Larger LDL particles, and thus a lower ApoB might be more “protective” or might minimize your risk of developing atherosclerosis at a young age. We are not sure of this… but this appears to be the trend for now. Science evolves, all facts have a half-life, and science is complicated— therefore, as the science changes, this post will change too ;-).
LDL particles and disease
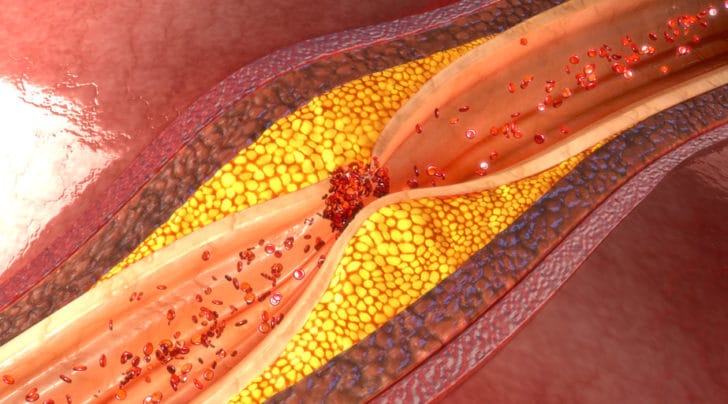
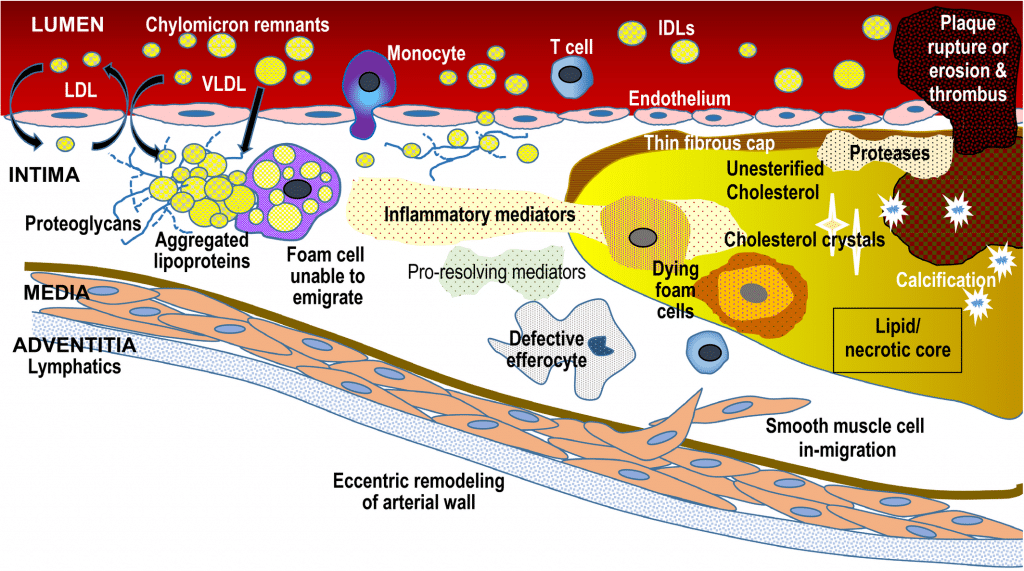
LDL causes heart disease because the LDL particle in your blood can cross into the wall of the blood vessels. Once in the wall, the LDL particle can be oxidized (OxPL). White blood cells called macrophages enter the wall to engulf these oxidized particles. These macrophages are now called foam cells. Those foam cells can die, and as the process continues, this causes a large “plaque” to form. This plaque is made up of cholesterol crystals and all the living and dead foam cells. That plaque initially forms and stays within the blood vessel’s wall. This will stiffen the wall of the blood vessel. That in and of itself can be a leading cause of hypertension or high blood pressure.
LDL by itself is not both necessary and sufficient to cause heart disease. Inflammation must also be present to create the changes to the LDL molecule within the blood vessel wall that leads to plaque formation.
A cell called the endothelium lines the inside of the blood vessel (lumen). The endothelium is a thin single layer of cells. A healthy endothelium keeps the blood in the vessel from clotting. If a plaque inside the vessel’s wall becomes large enough, it can rupture through the endothelial wall. Now the plaque is inside the blood vessel. That “plaque rupture” causes the blood to clot, leading to a heart attack.
Here is an important concept. Scientists find that plaque formation can start to occur in our early teens. Yes, our early teens. But we typically do not see clinically relevant events (heart attacks) until decades later. Why is that? It’s because LDL-related plaques take decades to become large enough to become a clinical burden. This is why this is a hard issue to study. Most drug trials last 6 mos or a few years at most. It’s hard to prove that an effect took place if the natural process takes decades to develop. So, if a new drug such as a PCSK9 inhibitor reports a 15% drop in cardiac events over a short time, imagine what a paper might show if that drug was pulsed (given for a year, then stopped and repeated) over someone’s lifetime.
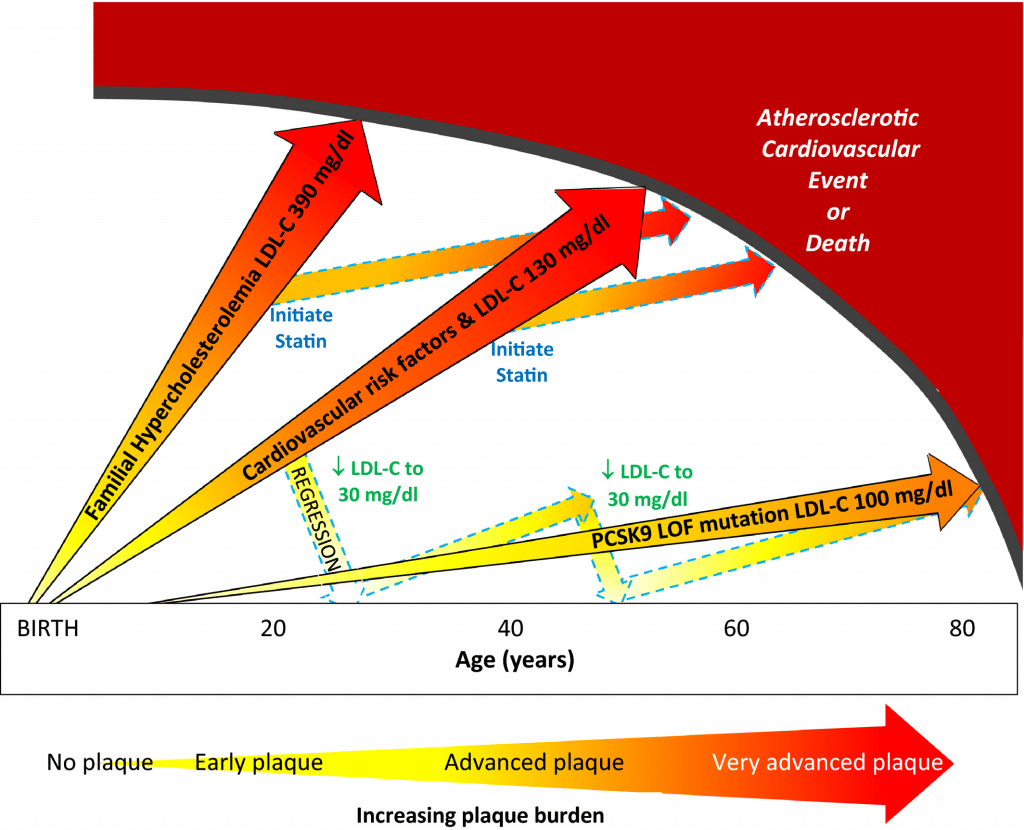
Your risk of heart disease is a time-dependent issue… it is your LDL or ApoB levels multiplied by the number of decades that your blood vessel walls have been exposed to it. This is what we refer to as an area under the curve (AUC) issue. The area under the curve which shows your LDL burden over the decades is the determinant of risk. Many chronic metabolic conditions such as insulin resistance, type 2 diabetes, and others are also AUC-related diseases. The longer you suffer from them, the higher your risk of having a clinically relevant complication.
So if you are 60, you have had 50+ years of these ApoB/LDL particles seeping into your vessel walls. This is how atherosclerotic heart disease evolves. This is why the younger we are when we sit up and pay attention, the better off we are. Some plaques, if the LDL/ApoB levels are dropped low enough, might regress. They will become smaller. That happens more easily when we are young. We are never too young to pay attention to what we eat.
What the paper below proposes is decreasing the LDL/ApoB burden starting at a younger age. The reasoning seems logical enough. It will take a long while until these studies are completed… so for now, keep in mind that your children do not have a free pass against an accumulated burden of LDL/ApoB-related plaque. What they eat when they’re young is affecting their artery wall now.
When you speak with your doctor about lab tests to determine your cardiac risk profile, it is important to ask them to check your ApoB levels. Many articles, including this recent one (November 2021), have shown that ApoB and not LDL better predict your risk for a cardiac event.
Here is the article… It’s worth reading.







