
Osteoarthritis of the knee can be a very disabling condition. Common treatments for arthritis of the knee includes anti-inflammatory medications, physical therapy, braces and injections. Those treatments are often effective for many years before you need to consider knee replacement surgery. For some of you , your knee pain does not respond to common treatments. That is when many of you will seek alternative treatments for your knee pain to avoid surgery.
Why some people have more pain than others isn’t always clear. The pain of arthritis can come from the bone itself, or from the soft tissue lining of the knee joint. That lining is the synovium. When the synovium becomes inflamed, your knee pain can be severe, and more difficult to treat.
You know the story… getting up from a chair, stiffness in the morning, trying not to have to go up or downstairs too often. Osteoarthritis of the knee is painful because of inflammation. Over the last 5 years a new treatment for knee arthritis pain has emerged. This new treatment for arthritic knee pain is capable of decreasing your pain for 6 or more years. That treatment is a selective arterial embolization. It sounds scary… scroll down and I’ll explain in more detail.

Synovitis and Knee Osteoarthritis Pain
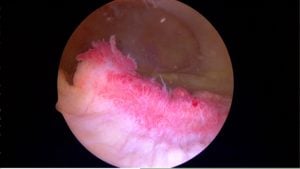
Synovitis of the knee occurs when the inside of the knee becomes inflamed. The tissue which lines the knee becomes inflamed, red, and angry appearing. The synovium, or the lining of the knee normally produces a little bit of fluid for lubricating the knee joint. When the synovium becomes inflamed it will produce a lot more fluid. That’s often why your knee will be swollen. If the fluid exits the back of your knee you will develop a Baker’s Cyst as well.
As you will see in the picture below, an increase in blood flow around the knee is causing the inflammation. This is why many of you might not feel relief of pain for very long after an injection into the knee. That’s because the excess blood flow is bringing more blood to the painful part of the knee. That often leads to more nerve growth as well. The blood feeds the synovium. If the synovium receives more blood then it can grow. As the synovium grows it becomes more irritated and causes more severe knee pain.
Arterial Embolization For Knee Arthritis Pain
Arterial embolization as an alternative treatment for knee osteoarthritis is a process where a Radiologist will inject a dye so they can see your blood vessels. Once the Radiologist sees the area where too many blood vessels have formed they will inject medication or microscopic spheres. Those little spheres will block the tiny abnormal arteries which are feeding your synovium and causing your pain. As demonstrated in this 2015 paper, selective geniculate artery embolization led to significant and long term relief of knee pain. In a recent (2017) follow up article, the authors noted that pain relief was sustained for more than 3 years.
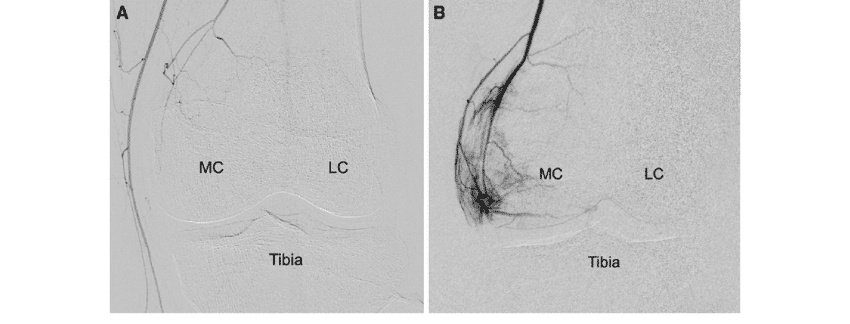
The image above shows a knee arterial embolization procedure. On the image labeled “B” you see many blood vessels in a small region along the inner side of the knee. The bones are barely visible due to “digital” subtraction. That area where the blood vessels are concentrated is often a very tender spot around the inner side of the knee in someone with severe arthritic knee pain. The picture on the left labeled ” A” shows the results after a selective geniculate artery embolization.

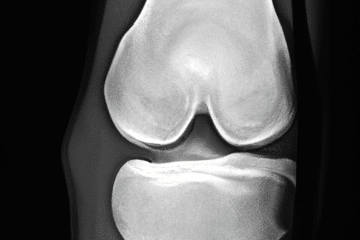
The picture on the right demonstrates the region of the knee which would correspond to the area of pain I showed in the images of the embolization procedure. Arthritis can affect many other areas within the knee. This was just one example where the patient had pain on the inner portion of the knee due to arthritis in that area. If your arthritis affects other areas then a different artery would be treated.
Recovery From Arterial Embolization
The patients who received a selective geniculate artery embolization for chronic knee pain due to osteoarthritis appear to have relief of pain almost immediately. For many that pain relief appears to last at least 6 years in some published reports. Of course your results might vary, but for now it appears that this is a procedure capable of helping restore your quality of life, improving your function and enables you to avoid knee replacement surgery. A selective geniculate artery embolization may be a great alternative treatment for pain from osteoarthritis of the knee.
Am I A Candidate For Embolization For My Knee Arthritis Pain?
Not everyone with arthritis knee pain will qualify for this procedure. Your knee X-rays should show that you suffer from mild to moderate osteoarthritis. This procedure is not likely to work well for those of you who have “bone on bone” or severe arthritis. This procedure should also be limited to those who have already tried other treatments such as medications, physical therapy, a compression sleeve and weight loss. A selective arterial embolization is a relatively low risk procedure, but that doesn’t mean that it should be the first treatment you try for your arthritic knee pain.
Images Attribution:
Okuno, Yuji & Mohamed Korchi, Amine & Shinjo, Takuma & Kato, Shojiro. (2014). Transcatheter Arterial Embolization as a Treatment for Medial Knee Pain in Patients with Mild to Moderate Osteoarthritis. Cardiovascular and interventional radiology. 38. . 10.1007/s00270-014-0944-8.









i am 85 years old and need a knee replacement. i would prefer this procedure. i live in fort myers florida. is there anyone nearby performing this procedure?
I’m not sure James… I am sorry.
I live in New Jersey.
My right knee is always swollen.
Have bone on bone on the medial side only.
Have minimal pain.
Have had knee injections and also cortisone
Injections serval times.
Just saw article about Genicular Artery Embolization.
Active Pickleball player.
Would hope that this could work for me.
I don’t know the answer to that… It’s only been used as a treatment for pain associated with osteoarthritis– not swelling alone.
Hi Dr. Luks,
I have severe osteoarthritis and have undergone lubricant treatments, cortisone shots, medication and vitamins for pain management of my condition. This occurred 8 months ago, the swelling has yet to cease, and I constantly find it extremely hard to walk and put pressure on my knee on a daily basis. Not sure if this is normal but this makes it difficult for weight loss results. I am only 40 so my specialist is against surgery for now. I am also looking for an alternative to avoid surgery all together. Do you know of any doctors in the NYC Metropolitan area that is performing this procedure? If not, are you doing the procedure?
Good Morning… The radiologists at the hospital system I work at perform the procedure. I see people in my office (914) 789-2735 to try and determine if they are an appropriate candidate, then I refer you to the radiologist if I feel there is a reasonable chance that the procedure will work.