Shoulder pain at night is a prevalent and potentially debilitating problem. For some of you, the pain is sharp when you change your sleeping position. For others, you will complain of a constant dull ache that doesn’t seem to go away. Sleeping with your arm under your head can be very challenging if you have shoulder pain at night. Most of you eventually find that sleeping on your back, or even in a recliner is the only way to get some sleep. This post will explore the most common causes of night pain in your shoulder. We will also review some potential remedies for easing your shoulder pain that worsens at night.

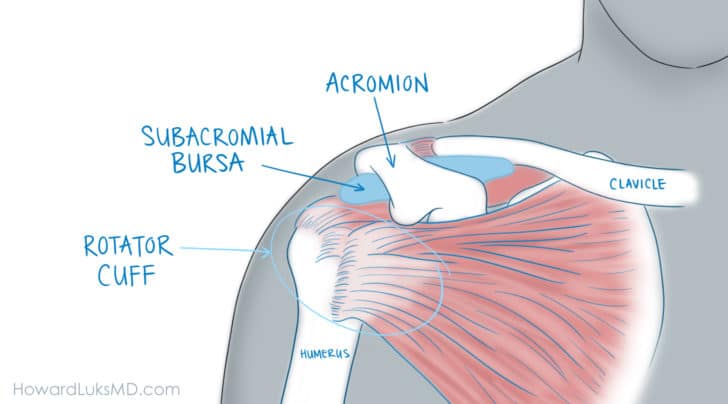
If you have shoulder pain at night, you know how disruptive it can be! Inflammation within your shoulder and usually in the region of the rotator cuff muscles is a leading cause of night pain. The specific structure that’s involved is called the subacromial bursa, a fluid-filled sac overlying the rotator cuff.
The 5 most common issues that can affect the rotator cuff and cause shoulder pain at night:
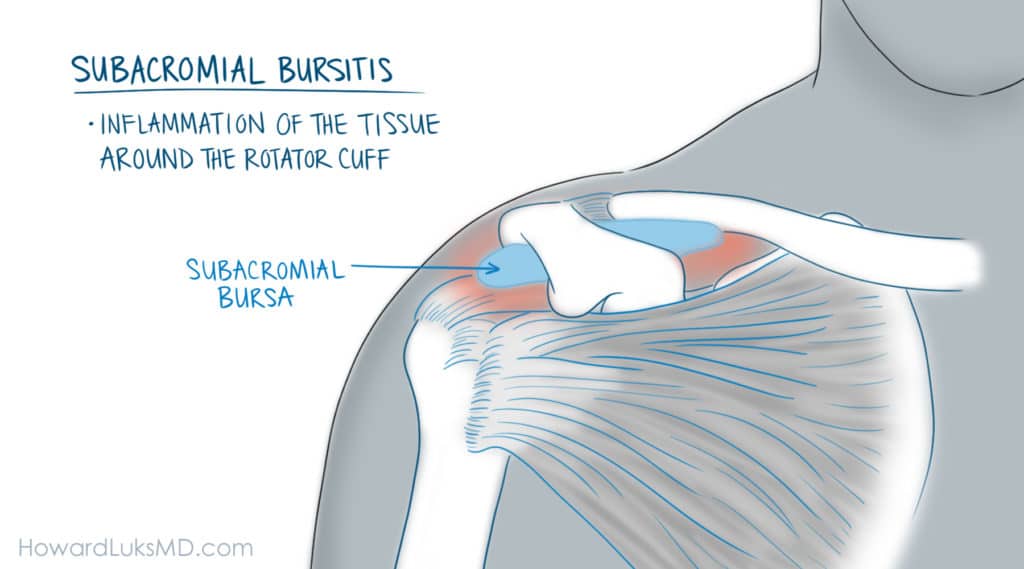
- Subacromial bursitis– inflammation of the tissue around the rotator cuff.
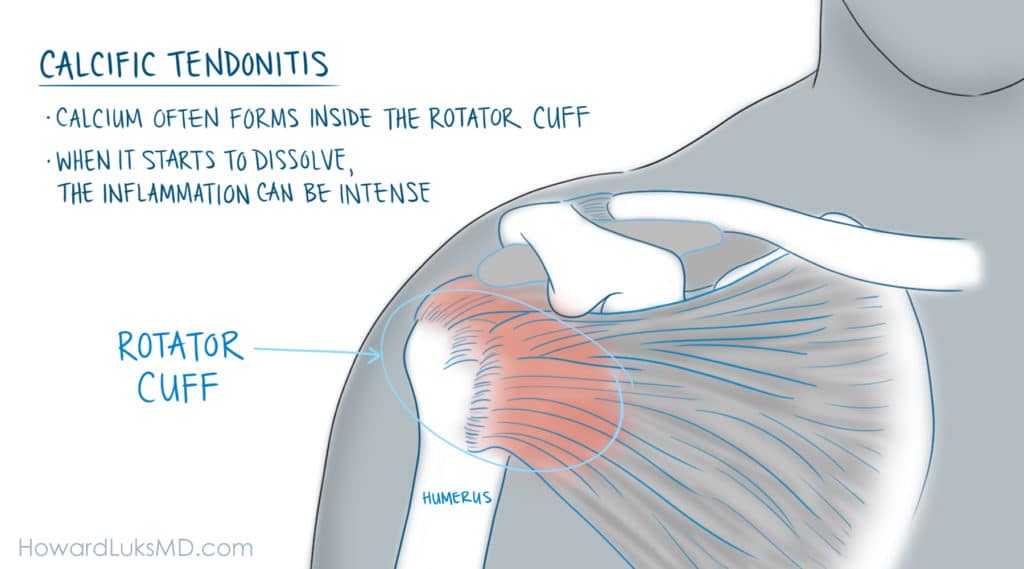
- Calcific tendonitis– calcium often forms inside the rotator cuff. When it starts to dissolve, the inflammation can be intense.
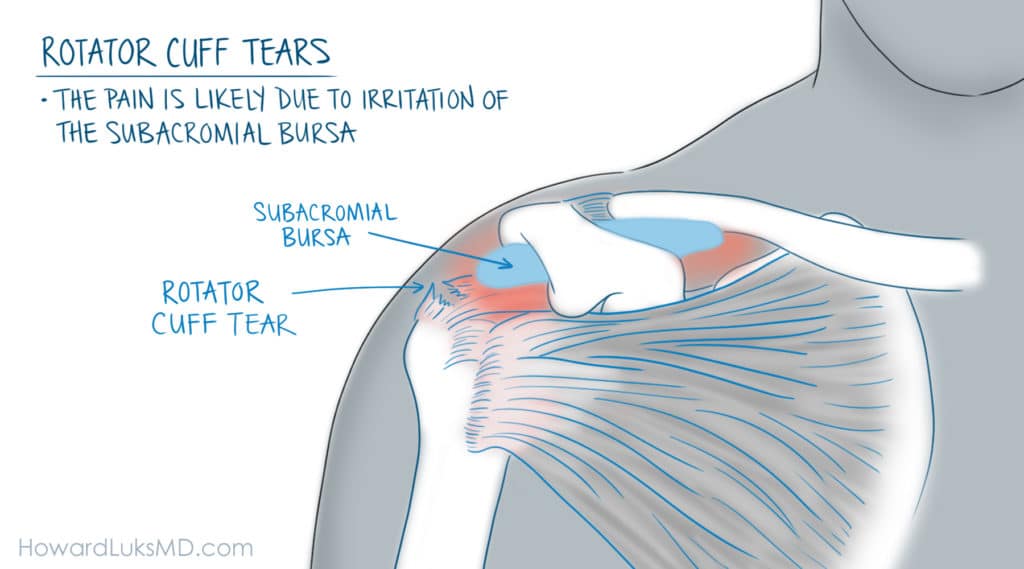
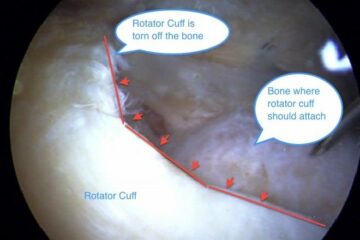
- Rotator cuff tears- the pain associated with rotator cuff tears is likely due to irritation of the surrounding subacromial bursa. See the pictures below.
- Rotator cuff tendonitis– Tendonitis of the rotator cuff can occur from an increase in activity that the shoulder is not used to.
- Frozen shoulder: inflammation throughout the shoulder joint, often leading to stiffness of the shoulder.
The most common cause of shoulder pain at night
As many of you know, no matter which side you try to sleep on, your shoulder pain wakes you up. Eventually, this will start to affect your quality of life and your psychological well-being significantly.
Inflammation of the rotator cuff and shoulder bursitis are probably the most common reasons why you cannot lay down and sleep through the night. The subacromial bursa is a small sack that sits on top of the rotator cuff tendons. A healthy bursa will lubricate the rotator cuff tendons in the shoulder to minimize friction between the rotator cuff and the bones of the shoulder.
The bursa can become inflamed because of various rotator cuff issues. Once angered, the bursa is likely responsible for a significant amount of your night pain.
Down below, we will cover ways to get this bursitis to quiet down.
The pain from bursitis is often on the outer side, or front of the shoulder. It is not usually on the top of the joint. Most people will complain of a deep dull ache. Some of you may feel a grinding or clicking sensation in the shoulder. The grinding is usually due to inflammation of the bursa and not a bone spur.

Very few of you will recall an injury that caused your night pain. Most of the time, there was no readily identifiable injury. That makes night pain in your shoulder very frustrating. You cannot identify an activity that caused it.
Most people who simply wake up with shoulder pain one day didn’t do anything wrong per se. The incidence of shoulder pain increases as we age. A frozen shoulder is a classic example. A frozen shoulder is a common cause of night pain. When you suffer from a frozen shoulder, you will find it difficult to sleep at night. That is due to intense inflammation within the shoulder joint itself. We often do not know what causes a frozen shoulder. The treatment of a frozen shoulder was discussed at length in this post.
Of course, recent sports injuries or overuse injuries to the rotator cuff can also cause significant pain at night. Injuries to the rotator cuff can also cause secondary inflammation of the bursa. Simply stated, if you suffered an injury from a fall and injured your rotator cuff muscle, the bleeding from that injury can cause inflammation in the bursa that abuts the rotator cuff.
Keep reading down below, and we will cover ways to get more comfortable and hopefully sleep through the night.
Why Does My Shoulder Hurt At Night?
Here is a list of the most common problems that cause shoulder pain at night. You can follow the links to read about each diagnosis, or you can keep scrolling down for remedies to try and get the pain to simmer down.
- Rotator cuff tear
- Rotator cuff tendinosis
- Calcific Tendonitis
- Tendonitis/Bursitis and inflammation.
- Frozen shoulder
- AC Joint Arthritis
- Tendonitis of the biceps
- Labral tears do not cause night pain.
 As you can see above, there are many different types of rotator cuff issues. One of the more common causes of rotator cuff pain is a process we call rotator cuff tendinosis. This implies that your rotator cuff is starting to wear out, fray, and degenerate.
As you can see above, there are many different types of rotator cuff issues. One of the more common causes of rotator cuff pain is a process we call rotator cuff tendinosis. This implies that your rotator cuff is starting to wear out, fray, and degenerate.
If the rotator cuff begins to degenerate enough, it may start to tear. A small tear is referred to as a partial rotator cuff tear. The rough surface of the rotator cuff tendons due to a partial tear can irritate or inflame the bursa sitting on top of the rotator cuff. Your shoulder might hurt with certain activities too… but it is the night pain that usually makes you call our office.
Some of you have injured yourself or fallen onto your arm, and now your shoulder pain is keeping you up at night. For those of you with night pain following an injury, a more severe full-thickness rotator cuff tear is possible. You should have your shoulder evaluated sooner rather than later.
What is the Treatment of Severe Shoulder Pain at Night?
The goal of treating people with severe night pain is to limit the inflammation within the shoulder, and more specifically, within the subacromial bursa. For most of you, this will be a temporary issue. Short term anti-inflammatory medications, perhaps an injection, and physical therapy, will have you sleeping well again in a few weeks. For some of you, the pain will persist, despite these often effective modalities.
It’s the middle of the night, and you’re having a hard time getting to or staying asleep. A combination of these treatments below can help ease your pain:
A heating pad
Yes, a heating pad. Used carefully (do not fall asleep with it on), and often, a heating pad can provide a surprising amount of relief. If your shoulder is not allowing you to sleep and you can’t get in to see your shoulder specialist, this is an excellent place to start. Many people think that ice is most appropriate for this type of inflammation… but a surprising number of you will feel better with a heating pad. They should be applied for 15 minutes, then taken off for 15 minutes… you can continue 15 minutes on/15 minutes off for as long as needed.
Sleeping in a reclining chair.
Sleeping in the semi-sitting position can help many people with severe shoulder pain get to sleep. You can also prop yourself up on a couch or in bed with many pillows to get yourself elevated at least 45 degrees. Putting a small rolled-up towel behind your shoulder to push it forward can also help minimize the pain you are experiencing.
Capsaicin:
Capsaicin is an over the counter ointment or rub. It functions as a counter-irritant. Capsaicin causes a burning sensation. In some people, it can cause an actual burn, so be careful and follow the instructions. When you rub capsaicin in the area where you have the pain, scientists believe that the skin irritation depletes a chemical from your nerves. By depleting that chemical, it is thought that this will quiet down the nerves around the bursa and the rotator cuff in the shoulder.
An Ice Compression sleeve:
An ice compression wrap: These ice sleeves seem to be useful at minimizing your pain at night and allowing you to fall asleep. Many patients have commented over the years that these sleeves have been helpful. Again, heating pads are useful, as well. Some people prefer ice, and some prefer heat. There is little chance of harm, so try both until you find what works best for you. These ice compression sleeves are also useful and improve your pain following a rotator cuff overuse injury, or surgery.
Shoulder Injections for Night Pain:

When you are in our office, we will discuss options to improve your night pain. Not being able to sleep is very disturbing, so you may want to consider an injection. Injecting cortisone or a steroid into the bursa can be one of the fastest means of achieving meaningful pain relief.
Injections into the subacromial bursa, that area above your rotator cuff that tends to become inflamed, can be beneficial in some circumstances. We know that routine cortisone injections are not the best idea. Frequent injections near tendons can cause the tendons to degenerate further.
Injections of cortisone into the bursa, however, can be beneficial in people who are very unhappy because they cannot sleep. These injections often start working in one day and continue to work for a few weeks to months, so you can begin recovering from your loss of sleep.
Kinesio Tape:

Kinesio tape seems to work well with many conditions to calm down the pain that people experience at night and even with certain activities during the day. The tape likely functions through a complex feedback interaction with the nerves of the spinal cord and brain. The pattern of taping doesn’t appear to be critical. Kinesio tape can be purchased online without a prescription.
Physical therapy:
Physical therapy to address the rotator cuff is beneficial over the long term to help improve your shoulder pain. For patients without severe night pain, then we start with physical therapy and try to avoid injections. If the pain at night is severe, then we usually try an injection first to calm things down and follow that soon afterward with a course of physical therapy. That therapy is generally taken 2-3 times per week for 4-6 weeks.
Many of you can learn the exercises yourself so you can continue the exercises on your own. Maintaining the activities, even after the physical therapy is done is essential to decrease the risk of the pain coming back.
Medications :
Many patients with severe shoulder pain at night require medications to help get them to sleep. At least until the pain starts to improve. Most people will start with NSAIDs like Ibuprofen, Naproxen, and Naprosyn, which are available over the counter.
Those of you with heart disease, ulcers, kidney disease, asthma, or hypertension will want to speak with your doctor or cardiologist first. Those of you on “blood-thinners” should not be taking anti-inflammatory medications.
Combining an NSAID with Tylenol can be even more useful. The two medications together can be very effective at minimizing your pain. The maximum daily dose of Tylenol for a healthy adult with no liver issues is 3000 mg per day. Taking 1000mg every 8 hours is usually the most effective way to take it.
Rotator cuff surgery for night pain:
The vast majority of you will not require surgery to alleviate your night pain. If necessary, surgery has been proven to be effective at helping alleviate the night pain associated with many rotator cuff disorders.
Surgery should be your last choice. But if you do not respond to medications, injections, physical therapy, and changing your sleeping positions, then surgery might be appropriate to consider.

Surgery for night pain in the shoulder is arthroscopic. That means that the surgery is performed through small holes with a fiberoptic camera. The procedure we recommend to alleviate night pain is called an arthroscopic decompression. That name implies that we will be decompressing the space above your rotator cuff by removing the inflammatory tissue. During the surgery, we remove the inflammation due to the bursa that sits on top of your rotator cuff.
If necessary, we can also remove calcium from calcific tendonitis; we can release the capsule for a frozen shoulder or repair the rotator cuff if it is torn. The precise shoulder surgery to alleviate your night pain will ultimately be determined by what we believe is causing your night pain.
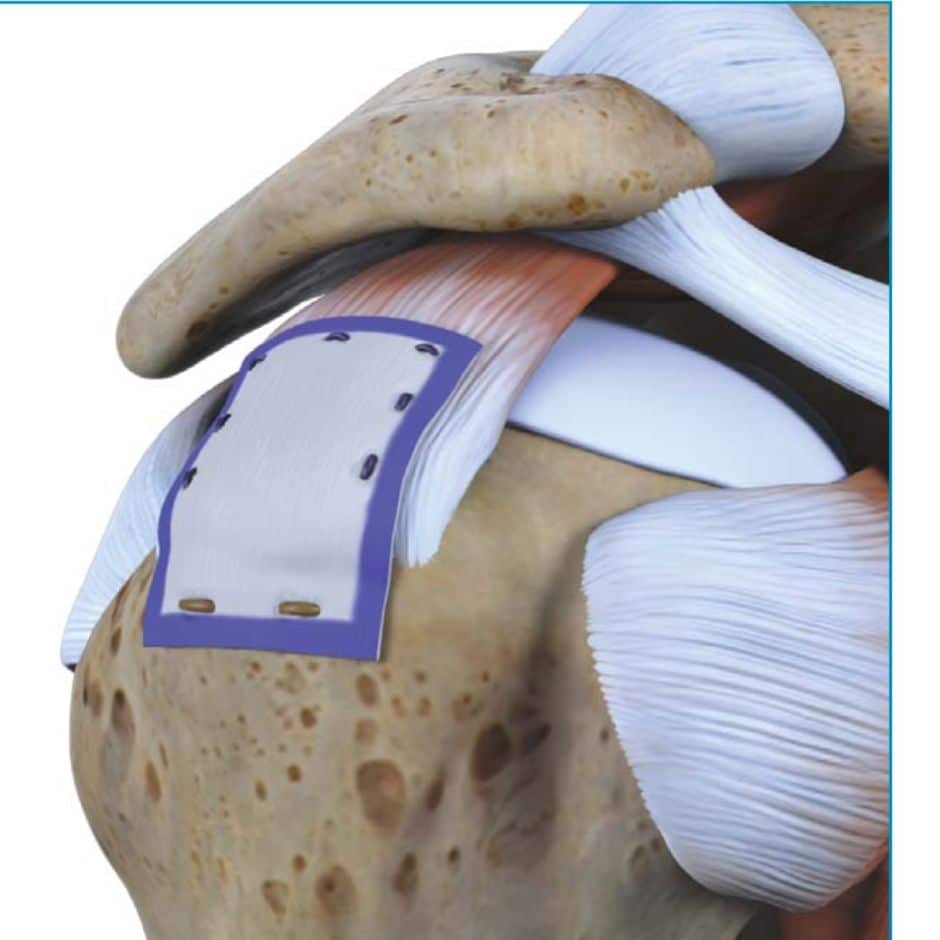
During the arthroscopy, we also inspect and evaluate the rotator cuff. If the rotator cuff has damage such as a partial tear, then we may consider placing a biological patch that might help to repair a worn-out rotator cuff. That patch is placed after the inflammation is removed, and the rotator cuff is smoothed out to eliminate the degenerative/frayed tendon, which might be irritating your shoulder.
Not everyone who has partial tears or fraying of the rotator cuff will require a patch. Many of us have seen issues in some people after the patch is placed. There is a chance that you will react to the patch– so we tend to use it in people with certain types of deep partial tears, or if we are repairing a degenerative rotator cuff tear.
I Tried Therapy, and My Shoulder Still Hurts At Night
 Non-surgical treatment of rotator cuff related night pain is very often effective. Most patients will be able to sleep comfortably after an injection and a course of physical therapy.
Non-surgical treatment of rotator cuff related night pain is very often effective. Most patients will be able to sleep comfortably after an injection and a course of physical therapy.
A small percentage of people will not respond to non-surgical treatment. I find that people with severe night pain are usually ready to have surgery sooner. They are miserable …as are those who live with them. Because we have a surgical option proven to diminish or eliminate night pain in your shoulder, it may be a reasonable option for you to consider if you do not respond to non-surgical or conservative treatment.
Research has shown that surgery on your rotator cuff to repair a rotator cuff tear or to treat tendinosis can dramatically improve or eliminate your night pain.
“Sleep disturbance is common in patients undergoing rotator cuff repair. After surgery, sleep disturbance improves to levels comparable with those of the general public. Preoperative and prolonged postoperative use of narcotic pain medication negatively affects sleep.”
Source: Sleep Disturbance Associated With Rotator Cuff Tear
 Surgical options for patients with night pain and injuries to the rotator cuff depend on the type of damage you have. The possible types of injuries we are dealing with include rotator cuff tendinosis, bursitis, a partial rotator cuff tear, or a full-thickness rotator cuff tear.
Surgical options for patients with night pain and injuries to the rotator cuff depend on the type of damage you have. The possible types of injuries we are dealing with include rotator cuff tendinosis, bursitis, a partial rotator cuff tear, or a full-thickness rotator cuff tear.
For those of you who injured your rotator cuff from a fall and have developed weakness, as well as night pain, then a repair of your rotator cuff might be your best option.
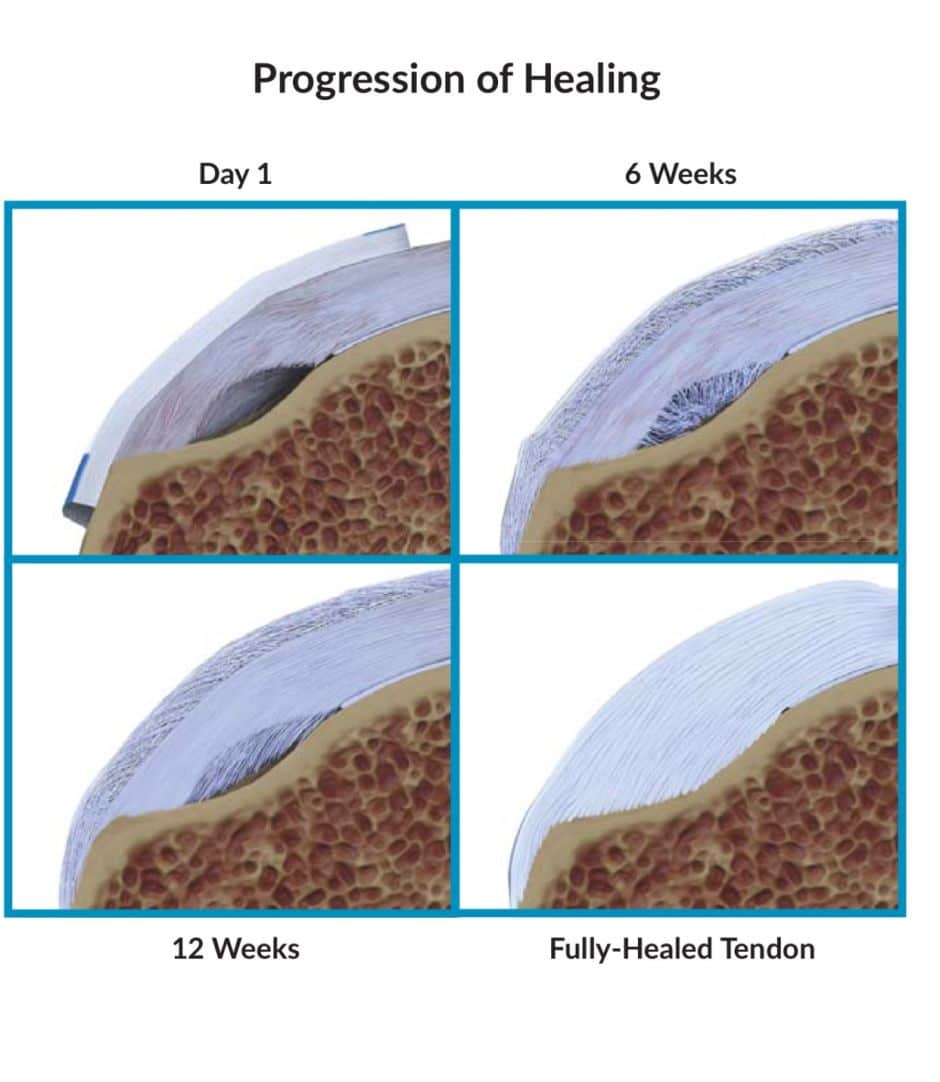
For patients with severe night pain due to tendinosis or a partial rotator cuff tear, a promising procedure is where we place a small patch into the shoulder during a shoulder arthroscopy (minimally invasive). Using a camera and other instruments, we place the patch over the area of degeneration or tearing. Then biology should take over and slowly regenerate your rotator cuff over time.
The patch usually becomes absorbed into your tendon and “induces” the tendon to heal. Before we place the patch, we will also clear away any inflamed bursa. Removing the inflamed bursa will ease your discomfort. Reversing or improving the tendinosis and partial tear could give you a good chance of not having to deal with this again in the future.
A fair number of shoulder surgeons are currently utilizing this technology.










Your article was very helpful as I finally found a description of what I think might be going on with my shoulder. For the past several months I have been waking up several times at night with severe shoulder pain-impossible to get back to sleep. I have been using Naproxen and Tylenol plus heat and usually end up propped on pillows on my couch-then I might get an hour of not very restorative sleep. I am desperate for relief as I know my lack of sleep is affecting my ability to function during the day, and I am now falling asleep in the middle of the day because I am able to sleep then-the pain is still there but not so extreme. I have a history of falls on my shoulder that have been successfully treated with heat, massage, followed by exercises to mobilize and strengthen my shoulder. This episode is not directly related to any specific fall and is not responding well to my usual treatment. I am exhausted and really need some help. Cortisone injections have been very helpful for other injuries (knee and thumb). Maybe this is the way to go? Your thoughts? Thanks-Beth
HI Beth .. Night pain can truly be exhausting. An injection might help. A thorough history and exam by a shoulder doc should be able to pinpoint the issue .. eg. Bursitis, vs Calcific tendonitis, etc. Then they can determine if an injection can help and where the injection should be placed.
I looked at a half dozen other websites before I found this one. The information provided was vastly superior to anything else. I appreciate the detail and expertise without the excessive medical terminology.
:-) Thank you! I’m super happy that you found it useful!
Hi, just read this article because I’m worried about the pain in my right shoulder. I do know I have to see a doctor and stop playing doctor on Google but something that worried me when reading your article is that this tear will not heal and will continue progressing? At least this is what I understood.
I’ve been with this pain around three weeks now. It seemed to go but it returned back, not as painful as the beginning. The only thing different from the rest is that I had real sleep problems maybe the first day only. Now I do wake up but only if I sleep over my right arm or if I turn to sleep on a side on right shoulder. I’m still working out. Where some days I forget I have a shoulder injury and some it is a little painful. Thank you for your article and greetings from Uruguay, South America!
Hi Enrique!
Actually, only some tears become larger over time. Some tears might not become larger over time. Many people with severe shoulder pain do not even have a rotator cuff tear :-) Most just have some fraying (age-appropriate changes). Many radiologists read that as a “partial tear”- that’s not entirely accurate. Surgery for most partial tears is rarely necessary.
Good luck to you!
7 months after surgery, acromium impingement (type 3) Chondroplasty to both the humeral head and glenoid. MRI suggested small cuff tears of the supaspinatus, and infraspinatus. The surgeon didn’t remark on the infra.. the supra, <25% linear tear at the footplate. Doc didn't repair the supraspinatus tendon. I seemed to have aggravated it, appointments to come… My question(s) is/are: Not only sleep time hurts, but driving is torture. The pain goes down my upper forearm and finishes at the tip of my forefinger, actually, the finger is kind of numb. What, exactly causes these particular pains? Why is laying down for sleep so painful? Also pain behind the same shoulder around the scapula. Great writing, and explanations, by the way.
Thank you Nathan, I’m glad you found this useful.
We are not sure why the shoulder acts up so much at night.
A decompression- removal of the acromion – is not always met with success. Cuff disease.. or rotator cuff tendinopathy/tendinosis is a common cause of pain in some people. PT remains the best way to approach rotator cuff related pain if your surgeon feels that is the source of your pain.
In patients with chest wall pain, scapula pain and radiating pain or numbness in the forearm/fingers we often look to the neck as a potential source. Just something for you and your surgeon to potentially explore further.