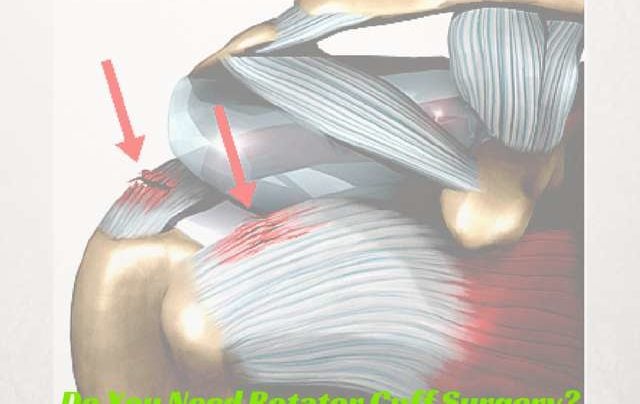
Rotator cuff surgery involves stitching or reattaching your torn rotator cuff tendon back to the humerus. The surgery to repair your rotator cuff is performed arthroscopically or with a small camera and other small incisions. With modern techniques rotator cuff surgery has become relatively easy to perform for Orthopedic Surgeons who specialize in shoulder injuries. But, this begs this question… do all rotator cuff tears require rotator cuff surgery? The answer might surprise you.
Whether or not you should consider rotator cuff surgery depends on a number of factors:
- your age
- the cause of your rotator cuff tear
- traumatic
- no injury
- the size of your tear
- if you have failed a trial of non-surgical management.
- physical therapy
- injections
- anti-inflammatory medications
This post and the answers below by our five Orthopedic Surgery experts deals with the topic of degenerative rotator cuff tears. That means that your rotator cuff wore out. If you had a severe injury which caused your rotator cuff tear, then I suggest you read this post. Rotator cuff surgery is usually recommended for nearly all traumatic tears.
Degenerative rotator cuff tears are very common. Many of you will not recall having an injury. You simply noticed your shoulder hurt one day. Some of you may have felt a snap while lifting up something like a suitcase. These are all common presentations for patients with degenerative rotator cuff tears. Many small degenerative rotator cuff tears will not require rotator cuff surgery. After 40, many people will have a rotator cuff tear and not even know it. You may wish to review our first Expert Series post where we discussed the cause of rotator cuff tears.
Remember:
- The rotator cuff is the most likely source of pain after 30
- Most rotator cuff issues, including tears are due to degeneration or attrition
- Most patients with small degenerative rotator cuff tears can be treated without surgery.
- Surgery for degenerative rotator cuff tears is generally considered after failure of a non-surgical regimen of physical therapy, possible injections and oral medications.
As accomplished shoulder surgeons, when do we consider rotator cuff surgery for a small degenerative rotator cuff tear?
Our Expert Series continues today with an answer to your question:
Do I Need Rotator Cuff Surgery?
Derek Ochiai, MD: Website, Twitter
Surgery is an option for degenerative rotator cuff tears that fail to respond adequately to non-surgical treatment, such as physical therapy and cortisone injections. Also, if the rotator cuff tear is inhibiting the patient’s quality of life.
Scott Slattery, MD: Website, Twitter
There are many options for the treatment of a small degenerative rotator cuff tear. I give all patients with small degenerative tears the option to treat them non-surgically with anti-inflammatory medications as well as physical therapy to improve flexibility, strength, muscle balance and coordination. This can work quite well. If the patient has good function and minimal pain, surgery is not absolutely required. If the tear is degenerative, chronic and large with associated muscle atrophy, initial non-surgical treatment with oral medications, injections and physical therapy is almost always the best option.
Marty Leland, MD: Twitter, Facebook
When I first see a patient over 40 with shoulder pain, my first treatment is anti-inflammatories, physical therapy, and frequently a subacromial steroid injection. I will then see the patients back 6-8 weeks later. If they are much better, there is no need for any further treatment. If they aren’t much better, I get an MRI to evaluate their rotator cuff. I usually do not order an MRI the first time I see them because, even if they do have a small rotator cuff tear, I would like to see if non-operative treatment would help them. If it does, GREAT! They may have avoided a surgery. I only order MRIs if they aren’t getting better. However, if I have a patient with a long history of shoulder pain and weakness and they are very weak on examination, I sometimes do order an MRI after the first office visit.
Jeffery Berg, MD: Website, Twitter
Degenerative rotator cuff tears are extremely common. Often these tears can be asymptomatic and incidentally diagnosed. So the first component of my “treatment” for these tears is to determine if they are symptomatic or not. If not felt to be symptomatic, I direct my treatment towards the suspected source of the patient’s symptoms and I advise observation of the tear. The observation primarily consists of clinical evaluations (history and exam) yearly if they remain asymptomatic or sooner if symptoms worsen, since these tears can progress and that progression usually is associated with an increase in symptoms. Depending on the office evaluation, I might also suggest serial ultrasounds or MRIs to evaluate for progression.
If these tears are felt to be symptomatic, I typically will start with nonoperative treatment. I find this to be the most reasonable treatment as degenerative tears often respond favorably to “conservative care” and although the symptoms can often respond well to surgery, they often don’t fully heal following the surgery. My nonoperative treatment consists of oral anti-inflammatories to treat the frequently associated bursitis as well as the pain that often brings the patient to the office. I will almost always include physical therapy as there usually is associated shoulder dysfunction and finally I suggest avoiding aggravating activities. Typically, I try this for 4-6 weeks, looking for any improvement. If improvement is seen, I will suggest continued nonoperative treatment until symptoms resolve or stabilize at an unacceptable level. If the latter, I will recommend an arthroscopic repair. If there is some retraction (lateral to mid humeral head) seen on the MRI, and depending on some specific patient characteristics (ie. young health, high activity level, etc.), I may suggest surgery on initial diagnosis, as I am concerned that if there is any further retraction, the tear may become unrepairable.
How we as physicians manage certain injuries may not always seem logical to patients. Many will not understand why we do not MRI every painful joint and many do not understand why we do not need to operate on everything that is “torn”. It is our obligation to educate you.
Our last post … When Should We MRI Your Shoulder will help you understand that we can make a reasonably good diagnosis and establish a treatment plan that should work without expensive, time-consuming imaging. In addition, many of our parts wear out. Like your favorite pair of jeans … Not all rotator cuff tears require rotator cuff surgery. The American Academy of Orthopedic Surgeons produced a document to assist surgeons in evidence-based management of rotator cuff tears. In this document, they find limited evidence to support surgery for degenerative rotator cuff tears without a trial of non-surgical management first. That said, some rotator cuff tears might continue to hurt after nonsurgical treatments … and you might be offered surgery as an option to improve your pain and thus your quality of life.










Dr., first, thank you for taking questions.
I’m a 47 yr old female railroad conductor, have been a conductor for 17 years.
My job includes pulling/pushing on doors that can contain up to 200 lbs of pressure, dozens of times a day, climbing up and down on/off trains, throwing switches via switch handles, etc.
All this I’m sure has helped bring about the shoulder pain I’ve had for the last four months. I’m still fully functional, but experience acute pain in the shoulder when reaching up or out (especially when done quickly), cannot lay on that shoulder, have pain when trying to tuck in my shirt in back, and lots of pain in the first few minutes upon waking.
Ibuprofen helps, and while the pain was initially between the shoulder and clavicle, it’s now mostly in the outer upper arm, or below the surface of that area. Occasionally it feels like something’s “shifting” there (the strands of muscle or tendon, for instance).
My question is, considering the shift in the focus of pain, does this sound like something that’s getting better? Considering that this has been going on for months, I’m getting used to it and learning to live with it. Should I be?
Sure sounds like your rotator cuff is bothering you. We each have a different threshold of pain which will lead us to seeing a doctor. Usually if the pain persists for a while I ask people to be examined by a shoulder doc to get a good handle on what’s going on.
Hi Dr. Luks:
I’m a healthy 68 yr old female, working full time, exercising, and very active.
I have a full tear of my superspinatus ( tossed a trash bag ) and 2 ortho doc opinions both say I need the surgery, or it could be non reparable, later on.
I’ve talked to so many others , including PT experts, who say I should have opted for PT and injections first, prior to scheduling the surgery.
What say ye?
thanks!
Most shoulder docs agree that the management of degenerative small supraspinatus tears usually starts in the non-operative realm and progresses to a surgical approach if the patient does not respond to non-surgical measures.
Dr. Lucas. I am a 69 year old male with a near full thickness tear involving >50% of the supraspinatus. My Primary care doc started me off with x-rays and a round of PT, limited to 6 visits by my wonderful insurance. The results of the PT initially were not good, which led to an MRI. My PCD said the 50%+ tear was not repairable without surgery. I prepared myself mentally for the long recovery period, and went to see the surgeon. I was blown away when he said he didn’t want to do surgery, and instead, gave me cortisone and a script for 18 PT visits. I’m torn, no pun intended. I stopped performing because I couldn’t carry my equipment up the stairs without significant pain. I was looking forward to getting back to that after recovery. Additionally, my father is 94, and very healthy. I plan to follow him and his success. Just not sure how much fun it would be with a broken wing. Is there reason to believe that the PT visits can restore full function to my shoulder?
It quite possibly could.
I am 62 years old. My right should rotator cuff is completely detached. It happened two Years ago. I go to the gym and lift weights 5x a week. It’s sore but not really painful. I have full range of motion. Should I have surgery? No injury, just wear and tear!
HI Sammy…
Without examining you and looking at you and your studies it is impossible to offer you a treatment plan. Sorry, and I wish you success with your shoulder !
Hi Dr Luks,
I’ve been lucky enough to dislocate my shoulder 5 times over the years and have developed a large Hill-Sachs lesion and torn Labrum. I am scheduled for a Remplissage procedure in a few weeks and have cold feet. I was told rehab is long and may take 6-8 months before I can return to surfing or go back to work as an RN. My last dislocation was 6 weeks ago and I am already back surfing, working, and in the gym. I know without surgery I will surely dislocate it again, but I am currently pain free and able live normally. I am 31 years old and am very active in outdoor sports. Should I get surgery now or keep risking future dislocations? Mahalo.
That’s a tough choice…. each time your shoulder dislocates you decrease the chances that surgery will be a success in the future.
A labral repair and remplissage works well as long as there is no bone loss on the glenoid (socket). If there is bone loss of a certain severity then a bone block procedure such as a Latarjet (Bristow) might needed.
As Orthopedists we prefer strong stable joints– if that is achievable. What happens if your shoulder dislocates in a strong surf and you can’t get back to shore easily? There are many situations where if your shoulder dislocates it can put you in harms way.
While surgery is not absolutely indicated— there is a strong argument to be made for considering the proper procedure performed by the proper surgeon.
Good Luck