
Many Orthopedic Surgeons believe that partial rotator cuff tears are a common cause of shoulder pain. The issue is that partial rotator cuff tears are also prevalent in people without shoulder pain. Therefore it can be challenging to determine if your shoulder pain is due to your partial tear or something else in your shoulder like the biceps tendon. It is not uncommon for a shoulder MRI to show a partial-thickness undersurface tear of the supraspinatus. That sounds bad… but is it?
Could these rotator cuff abnormalities be an age-appropriate change? Most of you are here because you may have been told that you have a partial cuff tear and you are curious if they need surgery, or if the pain can be managed with non-surgical treatment. So, let’s review what partial-thickness supraspinatus tears are and whether or not you need surgery to treat them.
The most common questions about partial rotator cuff tears that I receive are:
- Why did I develop a partial rotator cuff tear?
- How do you treat a partial tear?
- Do I need surgery for a partial tear?
- Can I live an active life with a partial tear?
- Can a partial rotator cuff tear become larger over time?
In the video below, I talk about these types of tears and the treatments available. Below the video, this article continues.
Partial Rotator Cuff Tears Video
Why Do I Have A Partial Rotator Cuff Tear?
 A small number of you had an injury such as a fall or a car accident, your shoulder hurts, and your MRI shows a partial undersurface or partial bursal surface supraspinatus tear. The supraspinatus is one of four rotator cuff muscles in our shoulder. The supraspinatus is the tendon that tends to suffer from partial tears most commonly. Injuries are a less common cause of partial tears than aging.
A small number of you had an injury such as a fall or a car accident, your shoulder hurts, and your MRI shows a partial undersurface or partial bursal surface supraspinatus tear. The supraspinatus is one of four rotator cuff muscles in our shoulder. The supraspinatus is the tendon that tends to suffer from partial tears most commonly. Injuries are a less common cause of partial tears than aging.
Should you immobilize or not move a shoulder with a suspected partial rotator cuff tear? No. Developing a frozen or stiff shoulder can make your recovery much longer.
Yes, many partial rotator cuff tears are considered to be an “age-appropriate” finding. But my shoulder hurts… surely that’s the cause?? Not necessarily. There are many causes of shoulder pain. Just because a radiologist mentions a partial tear, does not mean that is the cause of your pain. This is where our physical examination is critically important.
Don’t misunderstand me… some partial tears are caused by trauma. They can be caused by a single traumatic event, or by chronic repetitive stress, like pitching or serving in tennis. If your partial tear is traumatic, your MRI will show signs of inflammation or “edema” in the rotator cuff tendon, or in the bone the tendon attaches to. Most shoulder MRI scans will not show this edema or inflammation… thus, most tears are not acute, traumatic tears.
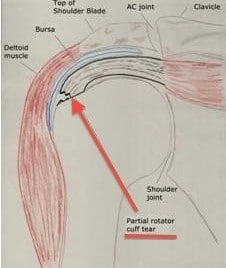
If you see “bursal surface” or “undersurface” mentioned on your MRI, that is merely referring to whether or not the top or bottom of the attachment of the tendon is involved. In the picture below, that is representative of a bursal surface partial tear.

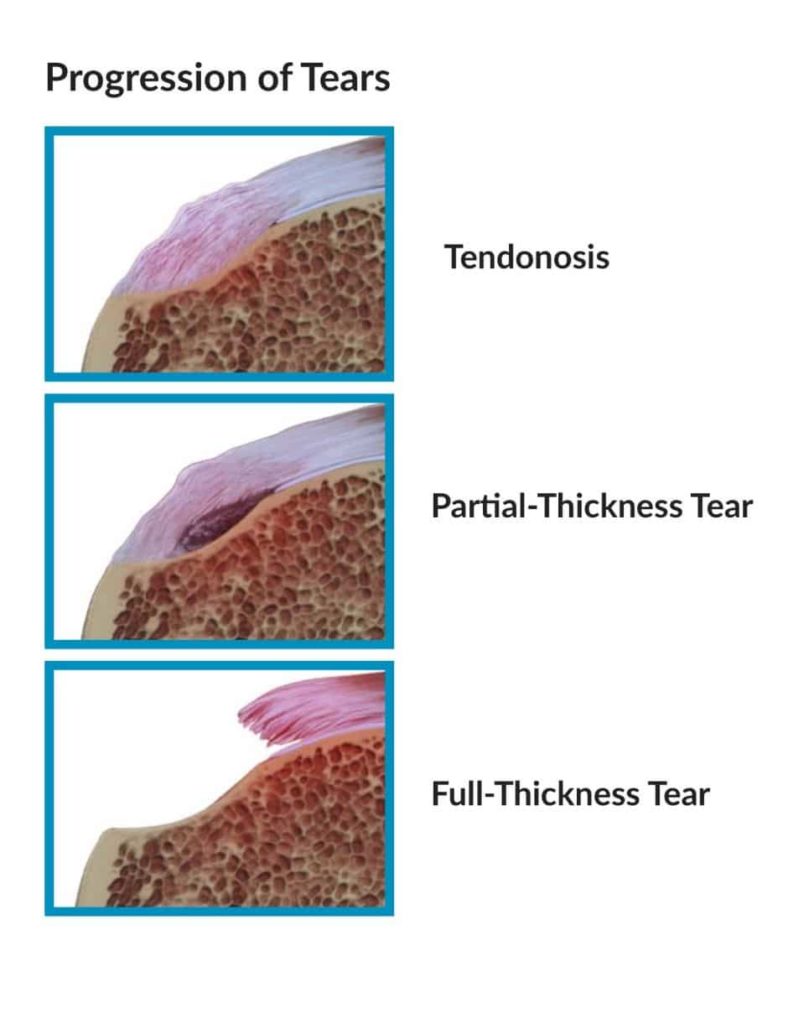
The primary cause of rotator cuff tears is a process we refer to as degenerative rotator cuff tendinosis. Tendinosis occurs as we age. Our tendons are changing at a microscopic level. That can lead to thickening of the rotator cuff, and eventually to partial “tears.” But it’s not actually a tear; it’s more like the tendon tissue became thinner and frayed, and on an MRI, our Radiology colleagues will read that as a “tear.”
Again, With rotator cuff tendinosis, our rotator cuff tendons are starting to wear out. Think about an old pair of socks or your favorite pair of blue jeans. You didn’t tear the “heel” of your socks, and you didn’t “tear” the front of your jeans, they simply wore out. Tendinosis is not caused by trauma or injury.
How Do You Treat A Partial Rotator Cuff Tear?
Our first goal as a shoulder surgeon is to determine if your partial tear is the cause of your pain. As I mentioned above, there are many causes of shoulder pain. Partial tears may or may not be the cause of your pain, regardless of your MRI. Our exam and your complaints often help us determine what the cause of your pain is. Hopefully, your X-rays are normal. Yes, X-rays are important because they can tell us if you have calcific tendonitis, fractures, or osteoarthritis of the shoulder.
Once we determine that the partial tear could be a cause of your pain, we can start the proper treatment. For those of you with minimal discomfort with specific movements, physical therapy will be offered. The majority of people with pain due to partial supraspinatus tears will respond very well to physical therapy.
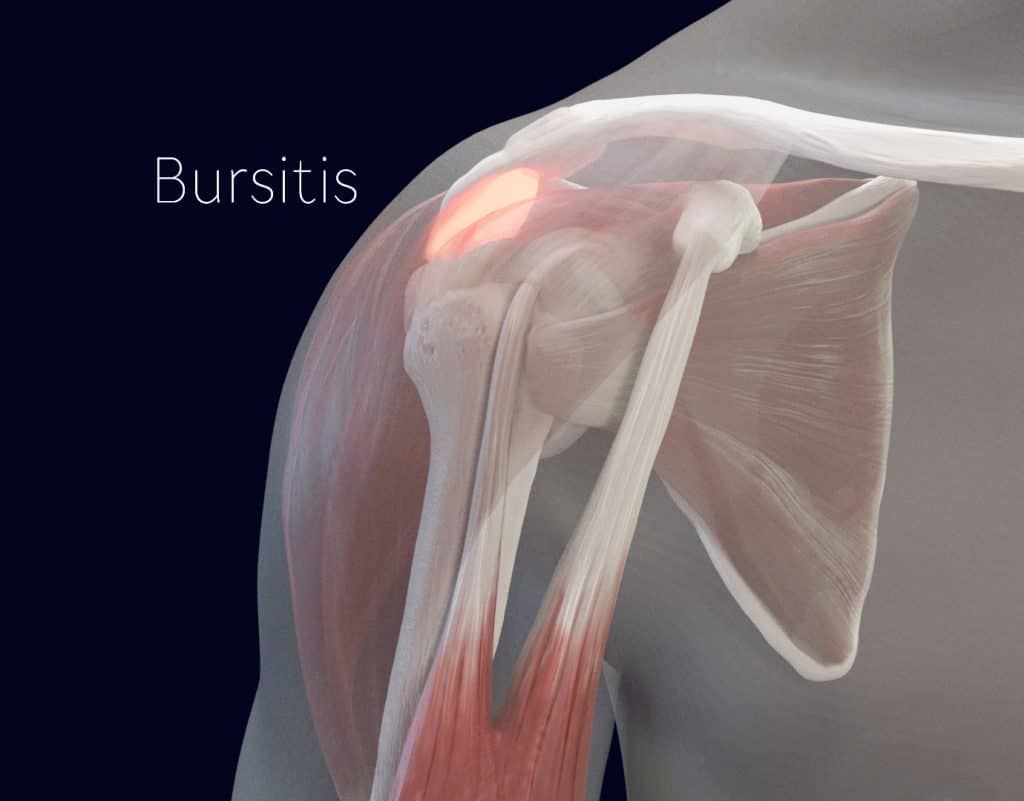 Some people with partial tears also have significant bursitis. Bursitis is usually the reason why you have pain at rest and severe shoulder pain at night. If we believe that the severe pain that is keeping you up at night is due to bursitis and your partial tear, then an injection may be useful. Injections into the “subacromial” space above your rotator cuff can minimize the pain and make the physical therapy easier to initiate.
Some people with partial tears also have significant bursitis. Bursitis is usually the reason why you have pain at rest and severe shoulder pain at night. If we believe that the severe pain that is keeping you up at night is due to bursitis and your partial tear, then an injection may be useful. Injections into the “subacromial” space above your rotator cuff can minimize the pain and make the physical therapy easier to initiate.
The majority of people with partial rotator cuff tears will respond well to physical therapy. To be effective, the physical therapy will focus on making sure you have a full range of motion of your shoulder. As shoulder motion is improved, the therapist will focus on exercises for your rotator cuff and the muscles surrounding your scapula or shoulder blade. You can do many exercises on your own, and here is an excellent resource for shoulder and rotator cuff exercises.
On a rare occasion, your pain will not improve with physical therapy, stretches, medications, and injections. If you feel that your pain is severe and you are willing to assume the risks of surgery, then a partial rotator cuff repair may be necessary. There are many ways to address partial supraspinatus tears at the time of surgery. Sometimes we only need to clean up the torn area and remove the inflammatory tissue. Sometimes, especially in people with deep partial-thickness supraspinatus tears, we may want to repair that tendon back to the bone.
Partial rotator cuff tear treatment:
- Anti-inflammatory medications, such as Ibuprofen or Naprosyn. Be sure to discuss the risks with your doctor.
- Tylenol: Do not take too much! It can be taken in addition to anti-inflammatory medications.
- Heating pads or ice. Heat is usually more effective, but if ice works well for you, then continue using it.
- Sleeping in a more upright seated position: Either in a recliner or with several pillows behind you.
- Injections: Useful if you have severe pain, especially at rest, and when trying to sleep.
- Physical therapy: By far, the most effective non-surgical treatment for partial cuff tears.
- Surgery: Often unnecessary, but if the above treatments fail to provide relief and your pain is severe, this will be an option to explore.
Can A Partial Tear Heal Itself Without Surgery?
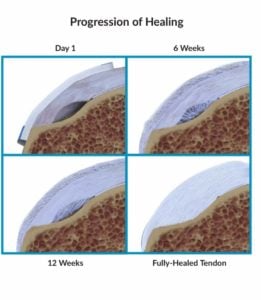
The research has recently shown that some partial rotator cuff tears will heal and reattach themselves without surgery. How long does it take a partial rotator cuff tear to heal? That’s not an easy question to answer! Depending on how severe the inflammation is, it can take a few weeks to a few months for your shoulder pain to improve significantly.
After surgery, healing for a partial tear will take many months. If a biological patch is used to try and repair a partial tear then it can take 6-12 months for the patch to integrate and result in healing.
We have learned a lot about these partial tears over the last few years. Some tears stay the same size over time, some of them will heal, and a few will become larger. Unfortunately, we cannot predict which partial tears will heal or which will progress to larger tears. What this means is that the presence of a partial tear in a typical adult shoulder is not in and of itself a reason to consider surgery. Like many shoulder issues, we try physical therapy, and in some instances, wait for many months to see if the condition will settle down on its own. If you do not respond to non-surgical treatments, then surgery may be considered.
Do you have questions regarding an Orthopedic injury or longevity?
Do you want to talk to an expert who can listen to you for 45-60 minutes and explain the options in detail?
Dr. Howard Luks offers remote guidance sessions to review your X-ray or MRI images and explain your options.
Dr. Luks has also received hundreds of requests for educational sessions on the topics discussed in his book, Longevity Simplified.
Very few people will go on to require rotator cuff surgery. And recovery from surgery for a partial tear can take many months too. So it is worth the investment into physical therapy and a home exercise program before considering diving into surgery as an option.
Do I Need Surgery For A Partial Rotator Cuff Tear?
Many who are suffering from shoulder pain due to rotator cuff tendinosis and partial tears will respond to physical therapy. Therefore, most of you will not need to consider having shoulder surgery. In addition to the physical therapy, your doctor will occasionally consider injections or over the counter medications. If your pain does not respond to physical therapy AND you feel that your quality of life is poor, then you can consider surgery as an option. The surgical options for partial tears of the rotator cuff and tendinosis are changing as we gain a better understanding of the biology involved.
Can A Partial Tear Become Larger Over Time?
The short answer is yes. Over many years a partial tear might become larger and form a full-thickness rotator cuff tear. AGAIN..this is a degenerative process, so as the degeneration progresses, your tear can become larger. Rotator cuff tears do not become larger overnight. It can take many many years for the process to evolve. In general, you should not consider surgery now to prevent the tear from becoming larger.
If you are considering surgery now, it is because you have tried physical therapy for a few months, and you have tried injections or medications, AND your pain persists. Only a few of you will need to consider surgery if you adhere to a proper non-surgical regimen.
There is no hard evidence that shows that we can affect the natural history of tendinosis. That means that you should only consider surgery now if you have significant pain that is not responding to non-surgical measures.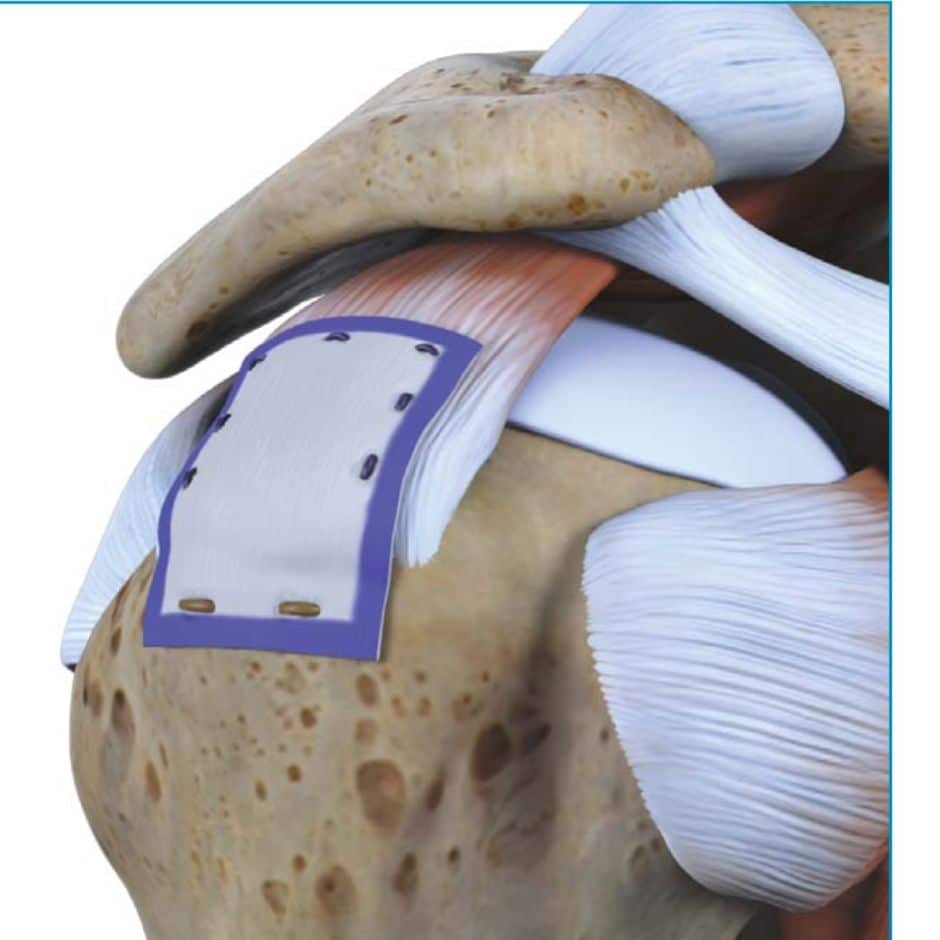
The vast majority of you will return to an active lifestyle after the treatment for a partial rotator cuff tear due to rotator cuff tendinosis.
The surgical treatment of partial rotator cuff tears and rotator cuff tendinosis is evolving. We now have a biological patch that we can implant in your shoulder, which shows promise in reversing tendinosis and healing partial-thickness tears. But as with any procedure, there are risks, and there are failures. So consider your options carefully.








Dan Gonet
I was scheduled to have surgery the week when the corona virus came to light. My surgery was cancelled and I have decided not to have it done once elective surgeries are resumed. The findings of my MRI stated” There is moderate acromioclavicular joint arthrosis with inferior spurring, narrowing of the subacromial space, and mass effect on the sujacent supraspinatus myotendinours region. Minimal fluid is seen in the subacromial/subdeltoid bursa. Coracoacromial and coracoclaviclar ligaments are intact. There is some thickening of the coracoacromil ligament. Signal alteration is seen in the supraspinatus tendon consistent with tendinosis. There is mild tendinosis near the infraspinatus insertion as well. The teres minor tendonis intact. There are findings of subscapularis tendinosis. There is some thinning of the proximal vertical segment of the biceps tenndon. Signal in the intrcapsular component indicates tendinosis. The supraspinatus, infraspinatus, teres minor, and subscapularis muscles are preserved. The deltoid muscle is unremarkable. Glenohumeral articulation is maintained. There is a small glenohumeral joint effusion. There is degenerative tearing of the superio labrum extending anteriorly. There is thickening and signal alteration alond the axillary recess which may be reflectionn of adhesive capsulitis. A small area of fibrocystic change is seen in the humeral head at the superior aspect of the bicipital groove. Acromioclavicular joint arthrosis with narrowing of subacromial space and mass effect on subjacent supraspinatus. Tendinosis and partical thinning of biceps tendon. Degenerative labral tearing. Findings suesstiion adhesive capsulitis. My question is, did I make the right decision not to have the surgery. What I’ve read is my condition is really frozen shoulder and may respond to PT.
Those are all very common findings… even in shoulders that do not hurt. There is nothing on that MRI report that says you need an operation. PT is the way to go.
Good luck
Dawn
I’m a 59 year old female and play golf about once per week. Recently lost about 20 lbs in the last 6 months due to changing food choices and exercise. The exercise includes military style push-ups and planks most days of the week. Over the last few weeks I’ve started to experience popping and a limited range of motion in my right shoulder. Could I have inadvertently injured myself?
At 59 your rotator cuff is starting to show its age… it’s a process we refer to as tendinosis. It’s not unusual for our shoulders to ache or hurt after starting a workout program. Often times that discomfort will subside. If the pain continues on for a few weeks / months and starts to interfere with your quality of life then you can consider having a shoulder doc examine you.
Jim Gallaher
Dr., I fell on my shoulder skiing on March 3 of this year and a few days later saw an orthopedist who diagnosed it as a strain. I immediately started PT but was still in considerable pain. Went back to the ortho and got an MRI that showed a partial tear of the infraspinatus. He diagnostically suspected a labral tear as well but didn’t want to do an arthogram as he felt there was no need for the invasive test if we weren’t doing surgery. I’ve been doing PT almost daily now since March 14th and range of motion is very good with minimal pain except for external rotation where I’ve just finally surpassed 90 degrees. Pain is minimal at night now after a rough second month and my daily activities for the most part aren’t affected. I still however seem to take 2 steps forward and 1 back with therapy as I occasionally do something that tweaks the infraspinatus and brings pain back to that area and the side of my arm. I also have a lot of shoulder clicking and a catching sensation on the side of the shoulder, presumably where the infraspinatus tendon attaches to the humerus. My question is how long will the recovery take? It’s been almost 3 months and while I know I’ve progressed greatly, I’m concerned it’s not fast enough or it won’t get any better. I still need to be careful when lifting things and have yet to be able to return to golf which I thought I’d be able to do by now with just a partial tear. I am a 46 year old male and the injury is to my non dominant shoulder. Any help would be much appreciated!
Actually a very common story…. As long as you are improving, regardless of how slowly, continuing with your stretches and exercises are worthwhile.