Shoulder Pain
Rotator cuff injuries are very common. Over the age of 30, the rotator cuff is responsible for the shoulder pain that most of us experience.
Determining the cause of your shoulder pain and determining what the actual pain generator is in your shoulder is our job as a shoulder specialist. Until we know why your shoulder hurts, it’s hard to start a treatment plan.
The most common causes of shoulder pain will vary by age, your activities and whether or not you have suffered any trauma. Rotator cuff injuries are only one of the many sources of pain in the shoulder.
Shoulder Pain by Age
Children and teens tend to have overuse tendonitis … or shoulder dislocations and labral tears due to trauma or sports injuries.
“Young” Adults and “weekend warriors” tend to have shoulder pain due to rotator cuff injuries or rotator cuff changes (tendinosis). Tendinosis and other degenerative changes within the rotator cuff occur as a result of genetics, activities, and aging. In this age group rotator cuff injuries may also occur as a result of trauma or injuries, but rotator cuff degeneration is the most common reason we see you in our office.
Seniors tend to have shoulder pain due to arthritis, loss of cartilage, and small, medium or even very large chronic (old) rotator cuff tears from a lifetime of wear and tear. Sometimes the torn rotator cuff tendon will upset the tissues around the tendon and cause a bursitis. This secondary bursitis is a common cause of pain and discomfort.
The Most Common Cause of Shoulder Pain In Adults
In adults, the most common source of shoulder pain are injuries of the rotator cuff … a series of 4 small muscles that coordinate the motion of the shoulder. This post on what is the rotator cuff will clear many questions about its structure and function. Again … The most common cause of shoulder pain is actually rotator cuff tendinosis, or partial tears of the rotator cuff.
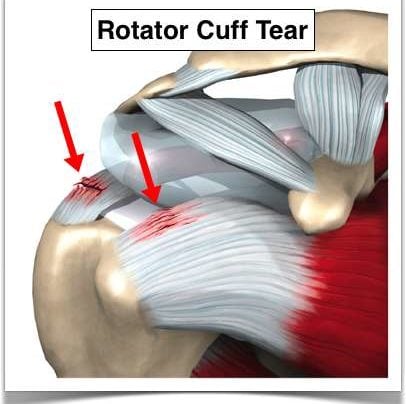
Rotator Cuff Tears
Let’s talk about rotator cuff tears (injuries). A lot of people say rotator cup tears— but it’s actually rotator cuff (C-U-F-F) tears.
What is the rotator cuff?

The rotator cuff are four small muscles located around your shoulder and they link together to form a cuff that literally sits on top of the top of your humerus. It’s beneath your deltoid so you can’t actually see or feel the rotator cuff. The purpose of the rotator cuff is to take all the energy or strength derived from the larger muscles such as the deltoid or latissimus or your pec major or your chest muscles and turn it into meaningful motion or rotational motion so you can move the arm out, move the arm up, any way you want to place it in space.
[hr]
What causes rotator cuff tears?
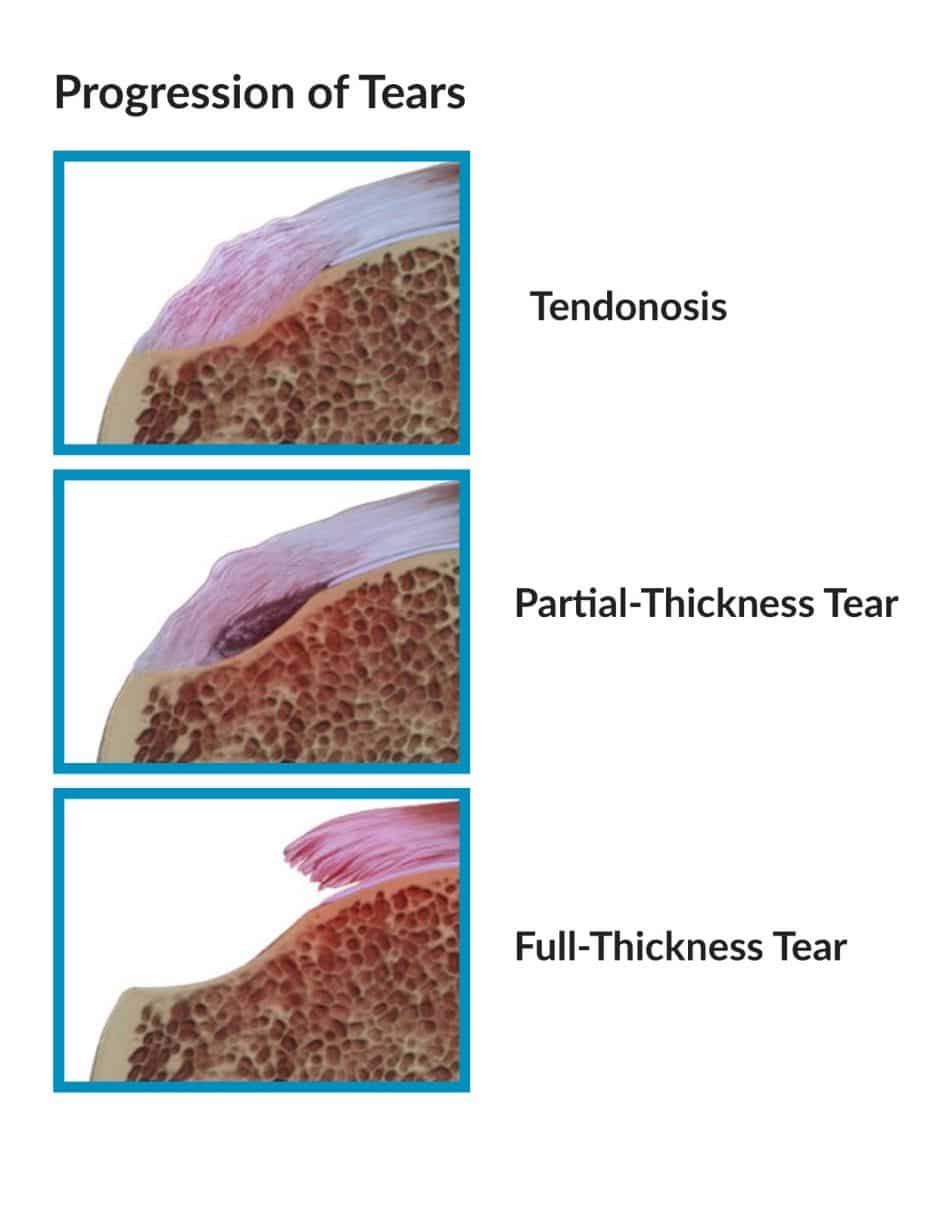 With time, sometimes with usual activities, sometimes with trauma, our tissues wear out, degenerate or tear. The vast majority of rotator cuff tears that we see in the office are attributed to attrition. Your tissues just wore out. Think of your favorite pair of blue jeans that you’ve had since high school if you could still fit in them that — think about the knees on the front of your jeans that that denim just wore out one day. You felt a breeze and looked down and there was a hole there. A portion of your rotator cuff tissue is not very different than that. It goes through a process of degeneration or something we call tendinosis which you can look up on my website. Tendinosis can progress from degeneration to fraying of the surface to a partial tear to a full-thickness tear where a portion of the tendon has detached from the bone.
With time, sometimes with usual activities, sometimes with trauma, our tissues wear out, degenerate or tear. The vast majority of rotator cuff tears that we see in the office are attributed to attrition. Your tissues just wore out. Think of your favorite pair of blue jeans that you’ve had since high school if you could still fit in them that — think about the knees on the front of your jeans that that denim just wore out one day. You felt a breeze and looked down and there was a hole there. A portion of your rotator cuff tissue is not very different than that. It goes through a process of degeneration or something we call tendinosis which you can look up on my website. Tendinosis can progress from degeneration to fraying of the surface to a partial tear to a full-thickness tear where a portion of the tendon has detached from the bone.
[hr]
Traumatic rotator cuff tears versus degenerative rotator cuff tears
There are also situations where you have a normal rotator cuff or a cuff with slight degeneration. You go outside. You play sports. You get tackled and knocked down or you slipped on the ice and fall on that shoulder or as you’re falling you reach for something to hold onto it and you yank your shoulder. Those situations can cause acute traumatic ruptures of the rotator cuff. Is there a difference between attritional and traumatic rotator cuff tears? Absolutely.
Most of us, and I mean academic physicians, believe that attritional rotator cuff tears can be managed in the majority of situations – non-operatively (without surgery). That means with physical therapy or doing nothing if doesn’t bother you too much, occasional injections, etc. If those non-operative modalities are unsuccessful in alleviating your pain AND you have significant pain with use or severe pain at night when you’re trying to sleep, then surgery is an option. But it is YOUR decision. Some tears will grow in size with time. So even if your tear feels better after therapy, you should see your surgeon every 4-6 months for a follow-up to see if the tear has become larger.
Acute or traumatic rotator cuff tears are a different story. Those should generally be repaired. (Again, not all acute tears need surgery and once again, my disclaimer applies and this is not medical advice. You should talk to your orthopedist.) But if you slip and fall and tear your rotator cuff, the likelihood of it being a large tear is fairly high. Those rotator cuff tears have a very good chance of healing after surgery. Should acute rotator cuff tears be fixed sooner rather than later? Yes.
[hr]
Can I delay my rotator cuff surgery?
Yes, assuming you understand the implications of that decision. A few issues to consider.
(1) Retraction. The rotator cuff is like a loaded rubber band, all right? Imagine a rubber band between my two fingers. I release it on one end. What’s gonna happen? It’s gonna shoot over towards the other finger. The muscle is no different. If the rotator cuff retracts or pulls far enough away from the bone, it will make the repair difficult and the likelihood of a successful repair when all is said and done much lower.
The other issue with waiting: Fatty atrophy. Atrophy is simply put — picture a leg that goes into a cast. You take the cast off in four weeks and that leg has shrunk. What has happened? The muscles have atrophied or become smaller. What happens with rotator cuff muscles that are no longer attached to the bone? The body changes the muscle to fat. It’s very cruel because if you re-establish continuity of the tendon, it doesn’t turn the fat back into muscle. So if you wait on a large, retracted, acute rotator cuff tear and that tissue turns to fat, then it doesn’t matter if you get it fixed later, because you’re fixing a piece of fat and it no longer functions as a muscle.
[hr]
Night Pain and Rotator Cuff Tears
Most patients with rotator cuff tears simply have pain. A few may have weakness and loss of motion as well. Rotator cuff pain can be activity related — such as trying to reach overhead: trying to wash your hair; for women, trying to put on a bra; for men, trying to put on a belt, or even trying to reach back and pull something out of the backseat of your car.
What brings the majority of patients into an office for small rotator cuff tears? Night pain. You can’t get comfortable at night or you’re waking up at night. Larger rotator cuff tears that encompass at least one or two complete tendons — will complain of weakness. They simply can’t lift the arm up or if they do, they can’t lift it far.
It will take an examination by an orthopedist and perhaps an ultrasound or an MRI to determine the actual size of the tear. X-rays may be useful to reveal changes that we can see in the bone that are secondary to rotator cuff disease as well.
So, bottom line take-home message:
Do all rotator cuff tears need to be “fixed”?
The answer is no. You can go much slower on the small attritional rotator cuff tears where the tissue simply wore out and try a course of therapy, injections, etc., However, we need to consider being much more aggressive with large acute traumatic tears after a significant incident or traumatic event.
We would love to see you if you have any lingering questions about your rotator cuff or shoulder injury:

Any questions? Please feel free to post them in the comments.
Remember, this for informational purposes and is not medical advice. Evidence changes frequently which makes some of these comments out-dated in the future and since it is a transcription I will not change them.









As always, well said. You have a gift for speaking to patients and not at them. Thanks.
Thanks Eric… hope all is well.
Dr. Howard J. Luks, MD,
How common is tendon tears with people with RA ?
Thanks for any info you can share.
Sandra Van Zandt
In general you run the same risk as the general population.
I like the demeanor of your responses. I am 64, fell on my shoulder (bowling) in March, had x-ray to determine any fx., told “if not better, in two weeks”, see an ortho. On exam, sent for MRI, after two weeks, had to call 6x for result.. (Crystal Run Health Care, Middletown, NY) nurse tells me “hi-grade-rotator cuff tear. It’s been approx. 50days from injury, too late for repair work?? (¬ there)
Hi doc, glad your’e there. I’m 64 yr. old fem. fell bowling end of Feb., on my right upper arm. I’ve had exam, x-ray, & MRI. Only know report read ‘hi-grade rotator cuff tear’, still have not heard from Dr.’s regarding course of treatment. Has too much time gone by for surgical intervention? Pain on certain movements. It took a 1 1/2 weeks to find out this much.
Mimi… I’m sorry you had to wait so long to hear of your results. There are many many variables we need to consider when contemplating a rotator cuff repair. As I always say, we treat patients, and not MRI findings. Before offering an opinion about the repairability of a tear, or even if a tear needs surgery I like to look at the report, possibly the films, talk to the patient and examine the patient. Then we have a complete picture and we can talk about the options available.
Hi doc I had a traumatic injury at work(firefighter) one ultrasound showed a 1.5 cm tear with bursal fluid and bicep tendosynovitis. Another ultrasound(different tech) saw no defect. I am experiencing a deep seated ache and lack of strength. There is Definetely something going on in there. Would an MRI be the test of choice? If a partial tear is found would surgery be recommended due to my occupation? any advice is much appreciated.
Eric,
The US is only as useful as the tech performing it and radiologist reading it. In general, an US can be just as useful as an MRI to visualize the rotator cuff. If discrepancies exist an MRI might be useful to better delineate what the status of your rotator cuff is.
In general, the first line of treatment of partial thickness tears is not surgical. Physical therapy, injections, etc can return most patients to full function.
Some partial tear can progress to full thickness tears, but *we* are not able to predict whose tear might progress and whose tear will not. The academic shoulder community does not talk about surgery on partial tears to prevent progression to full tears. *We* only consider surgery on patients with partial thickness tears once they have failed a thorough course of non-operative treatment. Unfortunately, both non-surgical and surgical management of rotator cuff disorders can require many weeks to many months to recover from.
Hope this helps.
Debbie Adams [email protected]
52 years old with severe night pain from left shoulder. Had right rotator cuff repaired Feb/2010
Mri ofr left shoulder shows severe totator cuff tendinosis small anterior thickness tear. The MRI also shows abnormal bone marrow at thelevel of the humeral shaft with relative decrease signal on t1 and increased signal on fat supppressed T2 images Appearence may be related to reconverted hemopoittic bone marrow secondary to anemia, hematological disorders of it’s marrow inflitration related to neoplastic process. Correlate clinically and further evaluation recommended. received one steroid shoit last week. Starting PT today. Ortho has nit spoken to me about the marrow changes. I am a smoker so there is a possiblility this is all related to my smoking. Can you further explain what theissue may be and do I need to worry about a cancer diagnosis.
Thx for the post. Suggest you talk with your primary care doctor before doing anything else re: the shoulder. Need to treat WHOLE patient… not just the rotator cuff. “Red marrow conversion” not very common in humerus. In general, atypical edema patterns shoulder be evaluated.
I have a complinet rotator cuff tear,this happen febuary10th. had MRI in March ,having surgery June 9. will my joint already be turn into fat, and can’t be fixed
Your surgeon should be able to tell you by looking at the MRI. The radiologist should have also made a comment about whether or not there was atrophy or “fatty infiltration”.