Hip pain is becoming more common with each passing week. Similar to other injuries we see, people are more active and stay active longer. It has only been 5-10 years since we have started to identify a common cause of hip pain — Tears of the labrum in the hip. In addition, we have identified anatomical reasons why you might have developed a labrum tear in your hip. Unless though issues are dealt with, an isolated labral repair may not work.
This is a guest blog post by Derek Ochiai, MD. He is a Sports Medicine trained Orthopedic Surgeon with a particular interest focus on the hip.
Nowadays, it is rather commonplace to read about an athlete undergoing hip arthroscopy for a labral tear of the hip.
This hip pain post will review:
- what is a hip labrum?
- why is the hip labrum important,
- how the hip labrum tears
- what kind of treatment is available for hip pain due to labrum tears
What is a labrum?
The labrum is a rim of cartilage that surrounds the hip joint. It attaches to the socket of the acetabulum. If you have friends who had a knee arthroscopy for “torn cartilage”, they had a meniscal tear of the knee. The meniscus of the knee and the hip labrum are made up of the exact same type of cartilage.
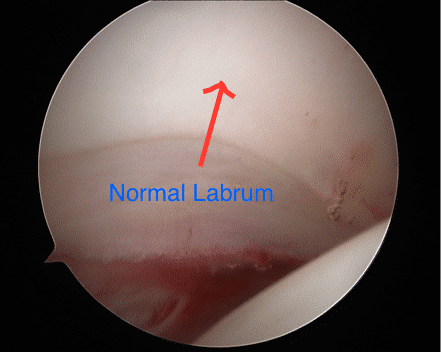
Figure 1: Arthroscopic picture of a normal posterior labrum. The labrum attaches smoothly to the acetabular articular cartilage. The femoral head is on the bottom right of the picture.
Why is the hip labrum important?
The labrum increases the relative depth of the socket, which can confer additional stability to the hip. This can be especially important in ballet dancers, figure skaters, gymnasts, and other athletes who put their hips through extreme ranges of motion. In developmental dysplasia of the hip (DDH), the socket is much shallower than normal, and the labrum deepens the socket to keep the femoral head of the hip in that shallow socket. Also, there are medical conditions where a person has increased joint laxity (such as Ehlers-Danlos), where the hip is more unstable and relies on the labrum for stability.
The labrum acts a seal around the femoral head, to maintain fluid pressure of the hip joint.
What are the symptoms of a labral tear in the hip?
The severity of symptoms can vary. The “hip pain” 90% of the time is perceived as deep in the groin. Sometimes, the pain can radiate to the side or the back of the hip as well. Many times, patients with a labral tear have pain and/or a feeling of catching in their hip, especially when going from sitting to standing. They may notice that they have to compensate to get in and out of cars. They may have pain with squatting and exercise, especially with sports that involve cutting and changing direction. Many times, patients also complain of pain with sex.
I didn’t injure my hip. Why do I have a labral tear?
The vast majority of labral tears are from FemoroAcetabular Impingement (FAI). FAI is a condition that develops in a person’s early teen years, where the hip is “out of round”. Since the hip joint and labrum are meant to function with round on round mechanics, this out of round conflict puts increased stress on the labrum. Over time, this increased stress can cause the labrum to tear. Symptoms of FAI greatly overlap with labral tears. In addition, symptomatic FAI can cause pain with prolonged sitting.
How is a labral tear of the hip diagnosed?
A medical professional can suspect a labral tear based on a patient’s symptoms and history. Clinically, the doctor can do provocative tests, such as the anterior and posterior impingement test, the McCarthy test, and the FABER exam, to further investigate. Many times, X-rays are very useful. FAI is a radiographic diagnosis, and usually can be easily seen on plain X-rays. With severe FAI, a labral tear can be inferred.
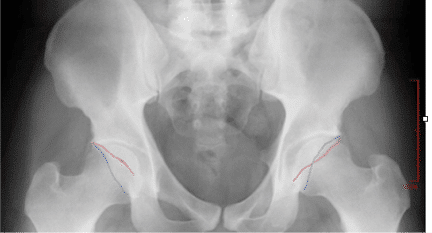
Figure 2: On left side of screen, normal acetabulum. The anterior wall (red line) and posterior wall (blue line) do not cross. On right, there is pincer type FAI, where the red and blue lines cross.
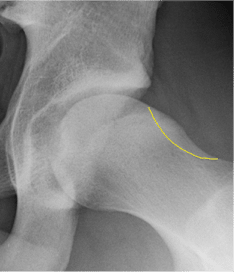
Figure 3: Typical cam type FAI X-ray finding. The yellow outline shows what the contour of a normal hip would look like.
MRI (magnetic resonance imaging) directly shows the cartilage of the hip. While a labral tear can be diagnosed with a plain MRI, an MRI arthrogram is more sensitive to labral tears. An MRI arthrogram does involve an injection directly into the joint, but then the dye can easily be seen leaking into a labral tear, making the diagnosis clearer.
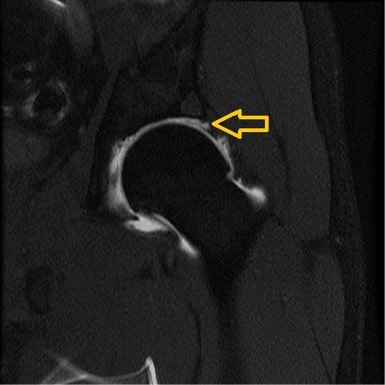
Figure 4: MRI arthrogram of a left hip labral tear. Arrow points to the dye leaking between the labrum and the articular cartilage.
I’ve been diagnosed with a labral tear. What do I do?
The mainstay of initial treatment for hip labral tears is physical therapy and activity modification. Physical therapy can help improve core/gluteal strength, which can shift the femoral head back in the socket a bit. This can decrease stress on the labral tear, which is normally near the front of the socket. While this doesn’t “cure” a labral tear, it can make some patients feel significantly better. Often times anti-inflammatories help our patients minimize their pain Sometimes, your doctor may suggest an intra-articular cortisone injection to the affected hip. While this also does not “cure” a labral tear, it can sometimes act as a physical therapy aid, allowing patients to “get over the hump” with initial therapy and start building core/gluteal strength.
When Should I Consider Having a Hip Arthroscopy?
Labral tears and hip FAI can now be addressed by hip arthroscopy, using cameras and small instruments inside the hip. “Scoping the hip” means looking inside the joint; there are multiple possible procedures that could potentially be performed during hip arthroscopy. In the past, the most common procedure was labral debridement, or trimming out the torn labrum.
While this has the advantage of not relying on the body to heal a labral repair, several studies have shown that labral repair has better long term outcomes than debridement. At least in my practice, labral repair is much more common. The labrum is repaired by drilling anchors into the bone of the socket, and using its sutures (thread) to wrap around and through the labrum to tie the labrum back into place. When doing a labral repair, any FAI should be addressed at the same time. Otherwise, there is a good chance of the repair failing (because the forces that tore the labrum would be the same forces causing it not to heal). Sometimes, a surgeon may tell a patient that the best procedure is an open surgical dislocation (through a large incision). There are some special cases where this approach may be preferable, but it is not common.
Do you have questions regarding an Orthopedic injury or longevity?
Do you want to talk to an expert who can listen to you for 45-60 minutes and explain the options in detail?
Dr. Howard Luks offers remote guidance sessions to review your X-ray or MRI images and explain your options.
Dr. Luks has also received hundreds of requests for educational sessions on the topics discussed in his book, Longevity Simplified.

Figure 5: Large anterior labral tear. Note the separation between the labrum and the acetabulum. Compare this to Figure 1.

Figure 6: Picture of a labral repair. In the picture, there are three sutures that are anchored to the bone, sewing the labrum back to the acetabulum.
A newer procedure to address labral tears is labral reconstruction. This uses a tendon graft to take the place of the torn labrum. Typically, this is only used for hip labral tears that are so degenerative, that repairing the labrum will not work to restore normal labral function.
Hip arthroscopy is a passion of mine. I hope this has been helpful to you. If you have been diagnosed with a labral tear, please ask your surgeon specific questions. Over the years, I have seen many second opinions from patients who had less than successful outcomes from hip arthroscopy that thought they had a labral repair, but the surgeon actually did a labral debridement. To me, “fixing a tear” means sewing it back and anchoring the labrum; however, “fixing a tear” to some could also mean “fixing the problem caused by the tear”, which could mean debridement.
Derek Ochiai, MD






Brittany
Hello,
I had surgery last year. I had a fai and labrum tear. Which both were fixed. I’ve been having the same type of pain in my groin and side of my hip again and my MRI shows that the tear is unchanged from the previous MRI which was prior to surgery. Is it possible to retear the tear?
Susanne
Hi. I am a 40-year old female (surgeon) and have just been diagnosed with a labral tear as well. No FAI and normal CAM. I do have an extra small bone at the tip of the Acetabulum on both sides. At the side of the tear, a small cyst might be visible on MRI. No trauma. Very uncommon you say? Living in the Netherlands, there is not much expertise here. I rather go for fysiotherapy before surgery. What would you recommend?
Hi …
physio would be the way to go before considering surgery.
Good Luck !
Jill
Hi! I was just recently diagnosed with a large left labral tear..no evidence of CAM or Pincer. I do have bilateral ischialfemoral impinges…saw a surgeon today who recommenda surgery. I have concerns that right may be torn too..actually the mri indicated impingement was worse on the right. He did not seem interested in addressing the right.:would it be a good idea to have an arthrogram on the right side as well to r/o tear before gojng for arthroscopic surgery for the left tear?? For the record , I am starting PT as I couldn’t do surgery for a few months. I am 41..and moderately athletic and work full time as a nurse..i love working out but havent been able to really run in a year without ” achy ” pain in my hips/ buttocks. I just would like to remain active!
Hi jill …
The most important thing you are going to do is to be sure that you are being cared for by a surgeon who specializes in hip arthroscopy. It is a very challenging surgery, and without a high enough volume the surgeon may be challenged trying to fix the labrum. In instances where a labrum is not repairable, then a new one should be reconstructed. Second and perhaps third opinions, when possible are a good idea when considering hip surgery. and volume matters. An experienced hip arthroscopy surgeon should be performing at least 40-50 or more of these / year.
Good luck
Derek Ochiai
Ms. Messenbrink,
Your son has a typical labral tear from cam FAI (see Figure 3 from my above article). In my practice, as a sports medicine hip arthroscopy surgeon, if a patient can play with the hip condition, I would allow play. He shouldn’t need to restrict his activities, except if those activities cause too much pain. Surgical correction is usually timed in a way that is the best for the athlete long term.
Desiree L Messenbrink
My 17yr old son has tearing that involves mid to anterior aspect of the superior Labrum that continues 2.1 cm into the anterosuperior aspect of labrum, also abnormal prominence of fermoral head/neck, alpha angle 70 degrees that may be cam type impingment.
The specialist is booked out 3 more weeks. He is a senior and plays football and basketball. Can you explain this in worried mom terms, should i restrict all activity? Will he be able to play college basketball?
Please help me.
Gordon Andrews
Hi Dr Luks,
I previously had a labral debridement surgery in 2009, and i have been complaining of pain since a few months after the surgery. I’ve had another MRI arthrogram which shows possible tears. One of the surgeons I met with is talking about the possibility of having to repair the labrum by stitching in cadaver tissue to the area where the previous debridement took place. Have you or are you aware of being able to use an autograft to reconstruct the cartilage at this time?
Thanks for your time.
There are many good hip arthroscopists who will reconstruct a degenerative labral tear. THe author of this article is one of them. I do not personally perform them… but I imagine that there are autograft alternatives.
Derek Ochiai
Mr. Andrews,
Labral reconstruction can be used doing both allograft or autograft. If a longer graft is required, sometimes allograft is preferable to get proper length. I have done labral reconstructions using both.
Linda
I’m a 57 year old women. I’ve been diagnosed with Hip impingement , bone spurs, labrum tears , and my pelvis has to be saved down. I’ve been getting cortisone shots, and working PT. But my doctor suggested after having a 3T MRI scan that I should have surgery. I’m afraid, and the cortisone seems to be helping. How long can I go before I need surgery?
In general, experienced hip surgeons avoid labral surgery in hips showing signs of degenerative osteoarthritis (bone spurs, etc). Perhaps seek a second opinion if you have any lingering doubts about the best course of action.
Derek Ochiai
Hip Arthroscopy hip preservation surgery can be a good option, IF there is little to no hip arthritis. I would recommend a second opinion, so that you are clear on what the options are for your hip. Certainly, if non-operative treatment is working well for you, then this is an option to continue.
Linda Straton
Hi to everyone, I’m a 57 year old women. I work for the PO for 20 years. I’m a letter carrier. I’ve been diagnosed , with labrum tears. hip impingement , bone spurs. And tilted pelvis bone . Very healthy otherwise. I’ve had 3 cortisone shots to my hip. And wonder how long can I put off surgery that has been recommended . And why can’t I just keep getting shots?
Derek Ochiai
Cortisone injections are not curative for your hip condition, but if they are used judiciously and sparingly, this is OK.
Linda straton
I’m a 57 year old women , with a physical job, I’m a city letter carrier. I’ve just been diagnosed with a hip impingement, bone spurs, labrum tear in my right hip. I had a 3t MRI that shows I need surgery. I’ve had 3 cortisone hip injections, that seem to help. My question is how little g can I keep getting injections until I have to have surgery?
Cath Roff
I am a fit and active 55 year old just diagnosed with a superior Labral tear but no FAI or arthritis. It feels like my hip joint drops out of the socket then grinds on the edge of the bone. It does this intermittently but is extremely painful and I have been using crutches for four weeks to manage the pain by keeping the weight off my joint. I am going to see a hip specialist this week. I am just wondering if physical therapy would be of any use to avoid surgery or if the mechanics of my tear would make surgery a better option?
Certainly no harm in trying PT for a few weeks to see if your symptoms improve.
Derek Ochiai
First of all, labral tears without some bony abnormality (dysplasia or FAI) is very uncommon. Also, hyperlaxity conditions can also play a role. If physical therapy is not helping, then repairing the labrum (or reconstructing the labrum) could help.
David
My Dad is 73. He has had an L4-5 fusion 2 years ago, has moderate lumbar scoliosis and has developed severe hip pain as well. An MRI revealed a “possible small anterior superior labrum tear as well as a small posterior labrum tear” He gets some relief by sitting with his right knee over the left leg. He says it takes some pressure off. The pain is lateral near the greater trochanter and is even sore to the touch. Everyone keeps saying it’s his back. Has no groin pain. Could small labrum tears with no groin pain be causing terrible pain?
I imagine his hip xrays showed evidence of osteoarthritis too. At 73 it is unlikely that a labral tear would be the #1 pain generator. If there is osteoarthritis on the Xray talk to your doctor about having the radiologist perform an injection of the hip. If they agree that has the advantage of confirming the hip as the source of pain… and potentially diminishing the pain for a few months.
Mike Fenwick
I have been diagnosed with osteoarthritis in my based on an xray of my hip, Is it possible that I have a labral tear rather than arthritis as my symptoms seem to match those of a labral tear. Is xray imaging definitive for osteoarthritis or is it possible that I have a labral tear and it was over looked
unlikely… Many arthritic hips will have degenerative labral tears too. But the research shows that treating just the labral tear is often met with failure. The arthritis will dramatically diminish your chance at improving after labral surgery.
Derek Ochiai
Definitely agree with Dr. Luks. In patients with hip arthritis, it is unusual NOT to have associated labral tears. There needs to be about 30% arthritis damage of a hip joint before the X-ray will show any changes, so if arthritis is seen on X-ray, it is definitely present.
Steve
I am a 68 year male who was actively walking about an hour a day until January of this year. I started having a severe burning in my left thigh that was so bag I could not walk.The pain goes away when I sit down.I self diagnosed with meralgia paresthetica that sounded like it was extremely reasonable..
I went to the VA and they first did an xray that showed nothing wrong followed by a MRI that showed a tear in my labrum of my left hip,
I am seeing the ortho doctor in three weeks BUT I currently still experience the burning thigh with no pain in my hip.
Does a tear in the labrum effect the thigh like I describe?
Thanks
.
typically not… keep in mind –our parts wear out as we age. An MRI of a 68 year old hip is never going to say “normal”. Just because something is “torn” or worn out doesn’t mean that it needs attention. I hope your doctor can shed some further light on this for you.
Christy
I am 2 week post op right hip labral tear repair. I am currently experiencing pain around distal femur and knee. I noticed I have residual fluid, slight swelling, and numbness around that area. My surgeon explained to me it’s probably from them hitting a nerve during the procedure. They did not do a nerve block on me. I’ve been icing it down 2 to 3 times a day. I’m feeling pressure and burning pain around that area also. Is this normal?
I can’t really comment on your condition… In general, a nerve stretch injury is possible from the surgery. You need to talk with your surgeon again if you are concerned. Many of these nerve stretch injuries heal — but another exam might be in order.
Karen Lilley
Dr. Luks I am a very healthy active 62 year old female. I have just been diagnosed with a labral tear (out patient arthroscopic/MRI). I have had it for 3.5 years and PT was not successful. A preliminary opinion (over the phone from a orthopedic surgeon) is because of my age I need a full hip replacement. I do not understand why they will not recommend a labral tear repair by arthroscopy. Should I be looking for a very experienced doc (Worcester MA area) in hip arthroscopy before rushing into full hip replacement? BTW they did not mention any FAI but did mention the presence of minor arthritis. Thanks for your advice
Once there is arthritis, a labral repair is not usually indicated. Osteoarthritis can dramatically affect the results of labral surgery.
Virginia
Thank you so much for all you have given us in terms of your knowledge on this forum. Sept 2016 I fell down 2 stairs landed on my left knee then ended up on my left hip. I have had a lot of pain on the outside of my hip. It hurts a lot when I’m sleeping at night also. I just had an MRI done and it shows a partially detached left Superior labrum. The bones are well aligned with normal marrow signal. There is no evidence of hip fracture or joint effusions. There is no evidence of avascular necrosis. Both hip joints are mildly to moderately narrowed but symmetrical in appearance. However, the left labrum appears partially detached superiorly and is best seen on coronal thin section image 10 of Series 7. It potentially could be caught between the femoral head and the acetabulum at times. IMPRESSION: no evidence of acute bone bruise fracture a fusion or avascular necrosis. Mild to moderate symmetric osteoarthritis of the hip period partially detached left Superior labrum. I will be 65 in May have been physically active at work unloading boxes standing on my feet and also sitting. I question, as you stated in the above Forum, that surgery may not help the tear because of my age and osteoarthritis?. Would Physical Therapy be an option or will it just aggravate the situation? I have not gone to see a surgeon yet just researching the internet and thankfully I came across your awesome site. Any feedback would be gratefully appreciated. Also, would a pemf mat be useful in this case? (Ex: Bemer mat or IMRS mat) I do plan on finding a capable doctor here in Florida but I wanted your expert opinion also. Thank you so so much for this forum!
It is unlikely given the arthritis that the labral tear is the source of your pain. If the pain is on the outside of the hip you should talk to your docs about evaluation for bursitis or gluteus medius strain. Depending on what they feel is the underlying cause, then PT is often very useful.
Ramona Prow
Dr. Luks, Thank you so much for your detailed response, so generous with your time and expertise. I’m finding that it may he necessary to go outside of Louisville to seek a second opinion but am unsure how to go about finding a doctor who specializes in hip/sports injury /adolescents.
Thank you again for your time!
Ramona
Jeannine M Hanson
My daughter was just diagnosed with Hip Dysplasia and bilateral labral tears. Our specialist skipped over the tears and went straight to recommending a PAO. My daughter is a sophomore in high school and a very active dancer. She is not ready to give it up. In your opinion would labral tear repair help extend her ability to dance for another year? We would like to hold off on the PAO for a year or 2.
Sorry Jeannine … It’s impossible for me to tell you what the next steps should be.
Ramona Prow
Good Morning Dr. Luks,
I’m reaching out to you regarding my 15 year old son. In July of 2015 he sustained a right hip injury playing soccer. He and another player went in to strike the ball at the exact same time, thus coming to an abrupt halt, and Tyler being the smaller one was on the losing end and felt a “pop”. He muddled through for the next few weeks with only mild pain, worked on stretching, icing etc. Ultimately he had a 3T MRI in late September. The orthopedic surgeon at that time ordered a “3T MRI to get the best possible images of the labrum without contrast” because he “didn’t want to inject the hip of an adolescent with an open growth plate”. The 3T MRI was read as normal but MD stated he could see that Tyler was growing rapidly and that was the likely cause of his pain and released him for soccer, told to work through the pain, which he did and was fine. Fast forward to October 29th, 2016, identical scenario however this time after a grueling high school season where he definitely had some overuse issues and more rapid growth. This time the physician thought Tyler had a “sports hernia” , went to PT , also had acupuncture & dry needling which helped with tightness but his anterior groin pain persists. His growth plates are still open but this time the MD ordered arthrogram with steroids. I am being told steroids could affect his growth and he himself eluded to that 16 months ago. I am very confused and concerned so requested we proceed with the least invasive option first. 3T MRI was done last week and is normal. Am trying to decide how to proceed as well as look for a second opinion. Considering asking for ultrasound to evaluate for hernia. Please give me your thoughts. As a pediatric surgical services nurse, I understand there are no guarantees and each medical professional can have different viewpoints etc., however I feel as though I must proceed cautiously and gather as much information as possible to make a more informed decision for my son. Thank you for your time, it is so very appreciated
HI Ramona …
There are so many causes of hip pain in a 15 year old. Labral tears are actually very rare in this age group. Sports hernia are 1. very very rare in this age group and 2. have been coming under fire recently as a diagnosis of exclusion and the possibility that it isn’t even a true diagnostic entity. An US will not show a “sports hernia”.
The injury you describe in a child your son’s age will usually cause an AIIS (rectus femoris) pelvic injury. It is a fairly benign injury in most. Hip pointers and chronic growth plate (pelvis) injuries are more common than labral tears.
The only way to arrive at a good diagnosis is a great physical exam. I would start with a second and perhaps third opinion. Steroid injections into the joint will not affect his growth but should be avoided if possible.
Good luck… there are plenty of sports docs who specialize in hip injuries — hopefully you have one near you.
Jaclyn
Help needed! I’ve been to two orthopedic surgeons for opinions. Last June while running, I experienced excruciating pain in left groin area. I was out of commission for 3 months icing, resting, etc. I had X-ray and regular MRI. Neither showed hip labral tear (one doctor said due to scar tissue?), but both doctors believe there is a tear. I’ve tried physical therapy for 6 weeks when pain flared/got worse in groin area and outer hip. Just got first cortisone shot 3 days ago. Any other suggestions? I’m a runner; last orthopedic surgeon said I may need to give that up entirely. Help!
There are many other reasons why a runner might have groin pain besides a labral tear — many large cities have Ortho surgeons who specialize in sports related hip injuries. Very few Orthos are good at hip arthroscopy. I would seek out an expert opinion near you.
Jaclyn
Are MRI arthrograms painful? I’m also wondering if a second regular MRI (it’s been 6 months since last one) might be warranted since I’m experiencing new pains near outer hip now. Thoughts? Thank you so very much!
Karen
Two years ago I had arthroscopic hip surgery for FAI,cam impingement with a labrum tear. I recovered well and was pain free. Now I’m having groin pain. I had a repeat arthrogram which shows a full thickness labrum tear. I just had steroid injection with no relief, taking gabepentin and NSAIDs. I have see an orthopedic surgeon who is hesitant to re scope my hip. My question is if the previous tear will show on the Mri scan? Or is this a new tear?
Did the sutures or the anchors from the first surgery show up? there should be some sign that the labrum was fixed previously. There are surgeons who can re-repair, or reconstruct the labrum if they feel it will help you.
Katie green
Hi, everyone very interesting in reading all of your comments. I am a 36 year old female who has has also been experiancing lots of all the above. All my troubles however started firstly when I was 17 years old but with my left knee, this was corrected with a lactural release at the time. Now at the age of 30 I have endured further surgery on my right knee, this time a miniscus tear and cart lodge shave. However during the last 9 months I have bee sufffering with extensive pain to my left hip, a pain I have problems with on a daily basis, forcing me to give up work as a full time nurse. Up until now I am not getting any answers from my doctor apart from the suggestion of bursitis and been given regular oral morph and morpinhine capsules for the pain, along with naproxen and codidramol none of which touch the pain. I am unable to put any weight through the leg itself and the pain does not ease with either lying down, standing or sitting. I currently find it very hard to sleep as any movement awakes me. It a constant dull ache which starts from the grion and Carey’s itself right around the whole pelvis on my right side. The only way to describe the pain is chronic tooth ache. I have now paid to go private for an MRI as an normal X-ray is showing no problems… the pain is making me feel so low could this possible be a tear. Has anyone else experienced anything like this before, it’s really beginning to scare me now. As I don’t understand how anyone can be in this much pain with it not being something very serious .. x any suggestions welcomed as I am at a loose end
Dave
Hi Dr Luks, I am a 42yo male in fairly good shape however due to some hip dysplasia I have developed a medium case of OA in both hips and torn my anterosuperior acetabular labrum in my right hip(kicking a soccer ball). It has been fairly painful especially when sitting or doing walking movements/stairs. The doctors are sort of at a loss because I am too young to have a hip replacement but it is a waste to fix the labrum and still have the bone deformity ruin it again. I have been doing physio such as isometric strengthening exercises like leg lifts, etc but this seems to irritate the problem more and I am finding it hard to sit, move, any sports, etc. My MRI showed the tear clearly as well as a ‘large bony bump at the anterior aspect of the femoral head neck junction’ which I have on both hips.
Do you have any recommendations to help cut back on the pain. I have been using a heating pad and I have been trying to stay away from pain medications. Should I be working my legs? Should I get the bone fixed or has the damage already been done? My last doctor shook his head and said ‘ I don’t know, maybe the horse has left the barn’
Thanks very much!
Hi Dave …
In cases like this, it is usually not worth having surgery because of the OA. Once the arthritis reaches a certain severity the chance that surgery will help you goes way down.
Typical treatments include physio, injections (under ultrasound or X-ray) and activity modification (which understandably no one likes).
Dave
Thanks Dr Luks. I guess I just have to put up with it as best I can until I need a hip replacement. I am a little worried that I would need at least one or two THRs more in my lifetime though and successes are very low for the second time around….
Mark McWilliams
Hello Dr. Luks. Thank you for all your comments above as well as the very informative article. I am 38, and have been dealing with an annoyance of pain for 6+ months. I cannot cross my right leg over my left without pain, nor perform seated spinal twists (stretching) without pain. I can still run, cycle, etc.. I have been diagnosed with a labral tear in my right hip. The doctor is a well known hip specialist in the area I live and has had good reviews/feedback. He is recommending repair and reshaping of the femoral head. I have scheduled myself for surgery, but it was a difficult decision as I do not experience significant pain and I am still very active with minimal impact. I will say that it has worsened a bit over the 6+ months, but marginally. I am deciding to have the surgery because I feel I will need it at some point down the road and just want to get it done sooner than later in order to fix the issue as well as prevent future damage. Do you think my strategy is reasonable?
Very tough decision you have Mark. It is also a very controversial topic. We can not say with 100% confidence that doing something now will avoid arthritis in the future. Unfortunately, not enough quality studies in this area yet.
Mark McWilliams
Thank you for your prompt feedback Dr. Luks. I feel like I am rushing the decision a bit. I have decided to keep my sx date, but I am going to see my PT again and have her assess my mobility and see what she recommends for strengthening and exercise to unload the hip and protect it a bit. If I am not in much pain (1.5 out of 10 only when placed in to certain positions) I just feel like I shouldn’t undergo surgery. I want to listen to my body telling me that I am still very active and able. Is my understanding correct that the repair surgery is to perform repairs specifically to alleviate pain and that if the tear can be managed (with minimal discomfort/pain) then surgery may not be the only option? Merry Christmas. Thanks again for your help and advice.
Joseph Hesslink
What would you do if you are diagnosed MRI with a acebular labral tear at 65 on lupron with stage 4 advanced metitatic prostate cancer m1 n1
probably seek a second opinion…. or have them inject the hip under US or image guidance to prove where your pain is coming from.
Andrew Finnerty
Thank You so much for this forum Dr. Luks. I had a work related fall/injury over 5 years ago that resulted in L4/L5 (maybe S1) ridiculopathy on my right side. Unfortunately I’m just getting PT now which has helped some with my core and lower back, but having a possible piriformis syndrome for so many years left me being unable to walk properly. It doesn’t hurt terribly to walk once I get moving, but sitting and laying on my right side is painful. Nothing catches per say, but I have had “the real” bad pain if I move my hip a certain way w weight on it (out/back and to the side) I have only had a lower back MRI. I’ve had pain down both sides of my leg and in my SI joint and behind my navel on the right side. I’m possibly getting a cortisone injection next Fri 17th in my lumbar to help treat the ridiculopthy, but after reading the forum I feel as though I may be mis diagnosed, partly bc of the initial report. I lifeguard in Southern NJ and some of the bosses who would write up the initial report are difficult to deal with. I’m 35 and try to stay active but have been progressive especially with not sleeping and dealing w chronic pain that Severely increases w weather change. It’s a workmans comp claim w AmeriHealth as the Ins. If the insurance would cover it, I have family outside NYC or if you know of surgeons in the Southern NJ/Philly area. I really appreciate your dedication to medicine.
Hey Andrew…
I’m sure there are a few good hip docs in Phili or at the larger academic hospitals in NJ.
Good luck
Shaun
Could you please help me with some advice? I have a very close friend in south Australia that for the last 2 years, has been told that she has pelvic pains (Pudendal neuralgia)
causing her to stop work, Day to day life is very hard for her! And going to bed is a challenge every night! She has tried so many different thing, and been told so many different things! She has now been told that she should have a dye enhanced Magnetic Resonance MRI as it’s now thought she may have a torn hip labarl! On her left hip! Even though most of the pain is on her right side?? ( could this be true??)
she will need to fly to Sydney to have this done! and is unable to do this til next year!!
I am flying out to see her from the uk very soon, and have seen many hip support bracers on the internet that could hep her in the mean time just like this
https://www.mediuk.co.uk/shop/hip-supports/
Do you think that I should buy one and take it with me? As I would like to be able to get her something to ease the pain! Only if it’s a small amount!
If someone could please help me with this I would be most grateful,
And if I do buy a hip brace, Then do I buy one for the left or right leg??
Thanks shaun
I labral tear on the left hip would not be considered to be a cause of pain in the right hip. Pelvic pain can be a challenge to diagnose. It often requires a multi-specialty approach — OB/GYN, Ortho, Physio- specializing in pelvic pain, etc.
Good luck to you and your friend.
Michelle
Hello, I found this article extremely helpful. I’ve been suffering from intermittent deep aching and slight limping pain in my rt groin for about 20 years. Last 8 months this progressed to burning pain and lower back pain as well as groin swelling and pain is now rt and left side. It’s always worse when sitting, squatting and end of day, I also have pelvis misalignment and loud snapping noise in my hips. I had an MRI (no contrast) of my pelvis, this showed a cystic area, possible bursitis or labral tear. My sports medicine dr is focussing on bursitis, injections and pain meds haven’t helped and he now believes its spinal pain. I think it still could be labral tear. My pain is sometimes unmanageable and I’ve given up dancing and cycling which is my passion! Should I seek arthroscopic investigative surgery? At this point I’m so frustrated and really want a surgeon to examine me, any support or advice would be more than gratefully received. Thank you
Milly
I’ve recently been diagnosed with a small labral hip tear, that I’ve dealt with for years. Had my first appointment with a surgeon last week, and he is arranging a CT to look more in depth. He asked me whether my problem ‘stopped me from doing anything’ which the answer right now is no. However it does cause pain on a daily basis depending on how I’m sitting or moving, and sometimes it aches throughout the day.
I’m wondering as he seems reluctant for surgery, can a tear get bigger over time if not repaired? If so should I avoid certain excises, such as running? I only 24, and concened about my hips as I age, if not repaired am I likely to get arthritis? (it already runs in my family.)
I obviously do not want surgery, however if I know that surgery will prevent future problems I would rather have it now whilst I’m young.
Any advice would be great, thanks.
MRIs are becoming very powerful. Many will find small “abnormalities” — many of those abnormal findings are not necessarily the cause of our pain. That is a hard concept to grasp for both patients and physicians — but it is true. The key is find out what the cause of the pain is. It is unlikely that a small tear will cause pain — but no impossible. The research and science does not show that these tears will worsen and even if they do, we do not know if that matters. So, talk to your doc about tests (sometimes involving injections) can help determine if the small tear i the source of your pain. There are many patients out there who had hip surgery for a tear, but still have pain. We are not sure why though…
Odette
Good afternoon,
I would like another opinion about my current situation, recent MRI shows (right hip) cranial acetabular retroversion, pincer type FAI and labrum tears in two places, also recently had cortizone injection for bursitis and another cortizone injection into hip joint 2 days ago, the pain is better but not completely gone. I had no traumatic event or sudden injury that caused it to become symptomatic. I would like your opinion as to how best get a permanent solution for this problem.
Nat Haskell
I was wondering what how you both would approach a prominent Fibrocyst or Synovial pit thats bordering 30% of the width of the femoral neck at the head neck junction. Is this something that you would leave alone and continue with decompressing the area of bony impingement? Would you remove the cyst and graft it?
I ask the question because I went forward with a arthroscopy to address a labral tear and to address FAI that included a large (1.1 cm) cyst at the head neck junction at the anterior lateral aspect. The osteoplasty was performed around the cyst and my ROM was seemingly great. My recovery was near perfect and was rapid. 2 weeks after weight bearing restrictions were lifted, I suffered a acute anterior femoral neck stress fracture along the mid section of the femoral neck. There was no trauma involved…..simply just walking from my car to the house. My doc was stumped about why it happened cause the fracture was anteriorly opposed to superior (tension side) of inferior (compression side)……but at the mid aspect of the anterior neck at the head neck junction. We ended up pinning the femor to insure we wouldnt have a complete fracture.
Im just curious if either of you have encountered similar pathology and how you addressed it.
Sugar Graham
My daughter broke her hip playing soccer. However, when she went to the ER they said if it was broken she wouldn’t be able to walk so they did not take x-rays. Instead, they referred her to physical therapy. After weeks of therapy, she was still in pain and uncomfortable. I took her to the doctors and they took a front view of her hip and said it looked normal and to continue with therapy but referred us to the Ortho. By the time our appointment came around it had been 8 weeks since the initial injury. That was when we were told that she had indeed broken her hip. I wanted a second opinion and an MRI done to make sure there was no other damage done from the PT or injury. They have ordered it but without contrast. Will tears in the labrum or other muscle/joint issues show up with the MRI without contrast??
Thank you in advance for any help or advice
Many radiologists do not require contrast to determine if a labral tear is present. Some radiologists do. In my region most radiologists do not ask for contrast MRIs. Fractures do not require contrast.
Megan
Hi Dr. Luks,
I have a labral tear on both my hips, I am a top athlete and am meant to be competing in the world champs next July. I am booked in for a cortisone injection to get me through an upcoming competition and am meant to be getting surgery later this year but just found out about the tear in my other hip. Can you please offer any advice? Why do I have it in both hips?!
HI Megan … Bad luck, bad genetics and repetitive stress. Some of us simply aren’t meant to be elite athletes… our bodies start to break down. Definitely not the answer you wanted to hear — but it is a common problem in highly competitive athletes.
Michael
About one year after hip labrum surgery where they attached by threading the labrum through 2 holes in my hip and shaved off some cyst. I am an avid baseball pitcher with a practice (mild work out) and game (all out work out) once a week along with yoga and swimming in off days. I am having groin pain, with the same feeling I had to where I need the original surgery. Right handed so I am pushing hard off the runner with my right foot. Of course my first reaction, mental thought was its my labrum again. Can I tear it again, with the cyst and bone spurs being removed 1 year ago. I went through all the P.T. and conditioned myself for 3 months after the medical clearance. I have a 99% feeling that it’s either lower back or hamstring related but can’t shake the feeling that it’s my labrum. Aside from the MRI with dye and X-ray, is there anything I can do at home to differentiate between which muscle groups may be causing my issue. It cost me around $14k for the surgery and and office visits and would like to avoid it if possible. 38 years old, excellent health otherwise.
Sometimes a good exam by a well trained hip doc can tell you without the need for further imaging.
Carole
How good of you to post this kind of information. I have a labral tear on what I thought was my good hip – recently had an anterior hip replacement on the other one!!! I’ve not had a great experience with some doctors, and it is good to have this detailed information available so that I can both make a reasonable evaluation of what I’m being told, and also be more comfortable with making a decision on any suggested procedures. Fortunately, I do have a lot of confidence in my surgeon, and he explains things very well, but I will remember so much more having read your thorough treatment of the subject. I rarely post on something like this, but I wanted you to know that you are very likely helping lots of people who, like me, don’t typically post the information.
Thank you for taking the time to let me know :-)
Donna Myers
Thank you for this column–
I am a 61 yr old female.. Until recently, have been in excellent health. 6 ft/134 #. 4 months ago I began having pain in my left hip(lateral trochanteric area) , initially intermittent following moderate workouts. my exercising was 5-6 times at local gym-doing Zumba, 360 Cardio. Pilates, Yoga–a variety each week. Over the past few months, pain has worsened to the effect that mere standing /wt-bearing and stairs are riveting.The pain wakes me up several times during the night. Aleve has not provided any relief. I already get acupuncture treatments q 6 weeks for my rt epicondylitis (did not want surgery and this treatments are wonderful-but are an Out-of-Pocket expense/not covered by insurance) In March I saw my Primary md, was referred to Ortho who initially diagnosed me with ileo-tibial band syndrome. was referred to PT-only had 3 treatment sessions–Therapist assessed that treatments not effective-referred me back to Ortho. Then had arthrogram MRI of left hip and LS spine series on 9 May 2016. Current dx is now left labrum tear with loose body/ and multi level arthritis with severe left foraminal & recess stenosis L2-3 w/ disc protrusion & arthritis On 31 May 2016 I have appt with a Sports medicine orthopedic surgeon who has a specialty in arthrospopic repairs. From the information you have provided, it seems I’m on the right treatment track finally. I am concerned about my gym routine-I surely don’t want to lose what I’ve worked on for the past 20 months since my retirement! I am so frustrated…. Your thoughts, advice please…..
Kathy Kangiser
I really enjoyed reading your article and all the questions and answers. I have had hip pain for 4 years. I have groin and glute pain as well. I have mild arthritis in hip. I have GT Bursitis. I do not show a lot of pain upon examination. According to a few doctors I am not a candidate for surgery. I was told my pain is not from tear. My problem now is along with the hip issues I have gluteal tendon degeneration and hamstring tendon degeneration. Is this caused by the tear and minor cam? Whenever I do PT I end up with severe pain. If I could work past this do you agree that extensive PT and/or exercise could help my pain which is pretty bad.? Thank you for all of the insight and information!
Javier Barraza
Thank you for the response. I do plan on seeing somebody who’s very experience.
As it pertains to cycling and FAI. Is cycling intrinsically bad for FAI? I definitely do not have pain doing it and pain only occurs on internal rotation and pinching my left leg and left hip (basically any motion that mimics the adduction of flexed, internally rotated hip). I’d like to be able to continue to exercise as I work towards an evaluation.
Javier Barraza
HI Dr. Luks!
Thank you for providing your expertise and knowledge to a growing but still not yet fully understand subject.
I’m a 46 yr old male who is very active. I’ve been diagnosed with FAI and a labral tear in my left hip with some hip dysplasia but have “managed” this condition for the last 7 years; mostly through stretching, physical therapy, and avoidance of impact sports such as running, jumping etc. I have been able to live pain free and have been able to ski, mountain bike, road bike, and even able to do some moderate hiking. Until this year that is. This past ski season I started having pain during skiing and sometimes when I tie my shoes. Definitely not pain all time but certainly if my left leg is isolated and my hip pinches to the inside. I’m going to have it re-evaluated soon as I’ve never had pain doing these activities before so I’m concerned that my condition has progressed. The last time I had it checked was 2 years ago and the MRIs and X-rays showed no significant change in my condition since the original diagnoses 7 years ago.
If it has progressed, am I candidate for arthoscropy? Or is the hip dysplasia and the fact that I did not correct this when I was younger rule me out for a possible successful outcome?
Thanks for any information you can provide.
It’s a complicated subject … dysplasia and osteoarthritis can significantly affect the outcome of treatment — both surgical and non-surgical. Just be sure that the person you see is very experienced in this area.
Nancy
I am a 54 year old female scheduled for surgery due to labrum tear and cam/pincer impingement. I am active (kickboxing and strength training 5 days/week), but do have rheumatoid arthritis. Would you be nervous about a positive outcome given my age. My surgeon, who specializes in this procedure, didn’t seem concerned but everything I’ve read seems to suggest that I may be too old to have a good outcome.
Age is a factor… as is the RA. If there are mild-moderate arthritic as well as a degenerative change in the labrum then the chance of success is significantly lower.
Kristi
I have a question Dr. Luks im a 17 year old female and i was diagnosed with hip flexor from soccer last year and was treated and healed but recently after my two games i feel a stabbing pain in my left hip and when it pops its painful and when i do the butterfly stretch and raise my leg it feels like my bones are grinding and that is painful as well i went back to the orthopedic and he diagnosed me with snapping hip syndrome and he said he is worried about me having a possible tear on my tendon he wants an MRI done but i dont want it if there is no tear and the pain in my hip has died down 5 days after i played my last game do u think its a tear if the pain eases up ?
Plenty of people …including athletes have tears of the labrum which are managed (and return to sports) without surgery.
Megan
I was diagnosed with FAI almost 6 years ago and recently found out I have a labral tear. My orthopaedic surgeon suggested a Synvisc-One injection but I have been in more pain than before the injection. My hip locks and my entire right leg goes completely numb, where I have to use my arms to lift my leg to get it unlocked. After the injection, I had my hip lock the next day and was in such excruciating pain I was screaming. What is being missed? My orthopaedic surgeon has no idea why my hip is locking and I am really regretting the decision to get the injection. I would love some advice on where to go from here.
second opinion.
Heather Collins
I am post 4 years surgey and it has definitely made my quality of life better. I was 38 when the surgery took place. I was originally diagnosed with arthritis because that is all they could come up with for my hip pain. After relentless complaints of pain, not being able to walk well, and at times not being able to climb the stairs to go to bed, I was finally diagnosed. It took almost 2 years. The frustrating part of the whole thing was not being taken seriously about my pain and the doctors/co-workers not believing me. With every exam they would push and poke. Since I didn’t say it hurt when they did this they didn’t believe my pain. I always told them the pain is deep inside. Trying to find a surgeon was something else, the labral repair surgery was not common in the area I am from and finding a doctor was hard. I called 50 surgeons and only 5 could perform the surgery. Since the surgery, I still have some pain and discomfort but usually when I am sitting. The one area that my movement remains limited is when I am having sex or I am in a position needing to hold my hips open, such as when I am getting a pap exam. After all this time I still have decreased strength in my hip/leg despite all the PT and strengthening I have done. After surgery I was not able to go back to work full time for 1 year because doing my job (I am a nurse) would cause the bursa to become inflamed. Now the more active I am, the less it hurts. I still get bursitis every now and then, but the best thing I have found to help with pain/discomfort is lying flat on my stomach to stretch the hip and thigh. Good luck to all of you going through the process of a labral tear pre and post surgery.
Susan Whitney
Hi Dr.,
I am 8 weeks post arthroscopic surgery for FAI. My MD was unable to repair the labram and had to scrape it clean, he also fixed my cam impingment. I have been doing ok post op but now having increase episodes of my hip catching causing pain that stops in my path. Is catching normal after surgery?
Anna
Hi Dr Luks,
I was recently diagnosed with an anterior superior labral tear to my left hip with pincer type FAI. I actually have bilateral labral tears but I’m really only symptomatic in my left hip. It has been fairly painful and I work as an RN in an extremely busy ER so I’ve been having difficulty tolerating 12 hour shifts on my feet. My orthopedic surgeon recommends arthroscopic hip surgery to fix the FAI and either repair or debride the labral tear. Can you give me your opinion on anchoring the labrum vs doing debridement and why one might be better than the other? Thanks! ~ Anna
IF surgery is contemplated then you need to address both. the FAI causes friction and tearing of the labrum. I’m not saying you need surgery… many do not… I’m simply saying that you need to see someone who does these ALL THE TIME.. Hip scopes are very hard to perform. Then, after you’ve met the proper physician you can determine the best way to proceed forward
Heather
Anna, I too am an ER Nurse and am fearful about my prognosis. Did you end up having surgery and how are you doing a year later??
Betsy
Good afternoon Doctor! My 20 year old daughter was just diagnosed with FAI and a labral tear in her hip. She had FAI surgery on the same hip in 2013. I didn’t think FAI was a reoccurring ailment. Do you have any input or suggestions? She is worried to go through the surgery again and end up in pain again every 3 years. I’d appreciate your input.
it’s not a recurring issue. There are many reasons why her hip might still be bothering her. FAI surgery is a very technically challenging procedure. Perhaps see a second opinion — someone who performs a lot of these procedures.
Janette
Hi, I am a 42 yr old female. I fell on a wet floor at a gas station a few months ago. I wqa told I have sprain my ham string. However. I have other things going on too according to my doctors. I keep getting a very sharp pain in my groin that shoots down my leg and makes my hip hurt. It beings me to tears if I move the wrong way. My range of motion is limited and it feels like I can not move my leg past a certain point. They think it is possible I have a labial tear. Heres my issue: they say it is degenerative. I just ran a half marathon 2 weeks prior and has No symptoms prior to the fall. They say it had nothing to do with this fall, which is when all this pain started. PT did not help. I feel like this is being ignored. How is it possible to have no pain, run a half marathon, trained for months, be active in yoga with full range of motion and no pain and have this tear without knowing? My leg twisted in when in a way it should not have in the fall. Help.
Kelly
My PT has recommended an MRI arthrogram for a suspected labral tear. My doctor ordered a plain MRI. Will the plain MRI show the tear adequately, or should I ask for an arthrogram to be ordered instead?
Brenda
Hi,
This is Brenda again from previous comment on Nov 18.
I’m wondering if you ever think that reconstruction is appropriate as a primary surgery? I have FAI with degenerated labrum as described on MRarthrogram (no discrete tear seen). I did try PT and a shot and am same or worse than before (and now beginning to develop symptoms in my other hip). I have now been told by one surgeon that reconstruction is most likely necessary to ensure proper function of labrum. Two other (very experienced) surgeons have said they only do reconstruction as a second procedure because they feel that repair even for “degeneration” works. It looks like having tried PT and a shot, that I am headed to surgery, but don’t know if I should go with the one who sounds like will most aggressively reconstruct if he feels it necessary as primary procedure, vs one who will only repair. I don’t want more surgery than I need. On the other hand, given the long rehab and recovery, I certainly don’t want two surgeries if the problem can be fully addressed with just one. Thanks for any opinion!
Jayne
Dr Luks,
I am a 20 year old cross country/track runner. I was a soccer player from 2000-2014. In 2014 I decided to switch from playing soccer at the collegiate level to cross country/track at the collegiate level (worked better with my schedule). I have always been able to ‘crack’ my hips. I can crack both sides without pain. Sometimes they will crack on their own when I turn my body a certain way. This has never caused any issues for me. 6 months ago, during cross country pre-season, I started having pain deep in my right hip. I felt my right hip clicking, and could physically feel it ‘pop’ with each step I took when I walked. I had an MRI done and my university’s sport’s medicine doctor diagnosed me with a femoral neck ‘stress reaction’. I was immobilized for 4 weeks on crutches, then underwent physical therapy along with cross training for rehab. With cross training, I noticed the pain starting to come back. After another 4 weeks of rehab and cross training, the pain was still present deep in my hip. I noticed prolonged standing or sitting not only caused increased hip, but also lower back pain. Since my pain was not going away, the doctor had me get another MRI. This MRI showed full recovery of the femoral neck ‘stress reaction’, thus showing my injury had healed. The doctor suggested the pain I was feeling was due to my body adjusting back to working out, and that this was to be expected. As an athlete, I know the difference between pain caused from fatigue and pain caused from injury. Frustrated that my pain was not being taken seriously by the school’s doctor, I brought the MRI results to my chiropractor/physical therapist at home who treated me (with unrelated injuries) during high school. The MRI results included a summary report that suggested if pain persists, to get an MRI arthrogram. Using this, my chiropractor/pt was able to write a script and get my insurance to approve of this MRI. The results showed slight right hip labral tear.
After this diagnosis, I followed up with my school’s doctor. He referred me to a hip specialist, but cautioned the only reason I should see the specialist was to take steps towards getting surgery (anesthesia shot), and that even after surgery my hip pain could persist. I’m 20 years old…the thought of needing hip surgery so young was enough for me to hold off on seeing a hip specialist. The thought of never being able to run again after the surgery is ever scarier.
During winter break, I cross trained and ran ‘as tolerated’ (low mileage) with limited pain. I returned for practice 1/10/16, and began running with the team again. After a long run (8 miles), I began to experience deep hip pain and lower back pain again, but also with a sharp shooting pain on the outside of my right knee. This pain started on 1/14 and has not improved. I have cross trained and completely taken two days off. I tried running very slowly today, but found the pain to be as sharp as before. It hurts to walk around and even persists when I lay in bed at night.
I am really frustrated and concerned for my health. My biggest concern is that in few years from now, I won’t be able to go on a leisurely 4 mile run without experiencing pain. Running was a great stress reliever for me, but has turned into a nightmare. I would love to be able to competitively run, pain free, my last year of college (next year), but don’t know how likely this would be seeing as I am having difficulties with walking. I am looking for any insight you have for competitive runners with limited time. But at this point, I am willing to give up my competitive running dreams if it is necessary for me to be able to run recreationally in the future. Even if I undergo extensive therapy, I still have to physically get my body back in shape to run at top speed. Any of your insight is incredibly appreciated.
Thank you,
Jayne
Amanda
I am 43 years old. have a right hip labrum tear and moderate FAI. I have had cortisone injection without success.
The pain is chronic at the site of the groin and right buttock (around site of SIJ). I have had physical therapy for 1 year now. I cannot walk more than 10 mins without causing extreme stress. I also have a bilateral avulsion of levator ani which means that my pelvis in unstable creating more instability for the hip. Surely if the orthopaedic surgeon recommended surgery to repair labrum/alleviate the FAI then the pelvic instability (which cannot be easily fixed) will still be problematic?
Andrew E
Hi Doctor, long story short, if a person has had a torn labrum for about 4-5 years now without it being fixed, is it still possible to get it fixed surgically? Or is it bad if a person has waited that long?
A good hip surgeon could still fix it, or reconstruct the labrum … if it is necessary to do so. Find someone who performs many many hip procedures for a solid consultation.
Kim Riedlinger
As diagnosed by an Arthrogram MRI, I have a large Labrum tear in my left hip. Radiology report reads: large tear from 12 o’clock to 5 o’clock.
I am a veteran. Today I saw the VA ortho surgeon again. He says I have to live with it and Labrum tears don’t cause pain. I argued with him and he agreed to write an order to see a civilian doctor that might know more about these tears. My problem is I only have one shot with this so I need to find a good dr. Is there a list any where ? As a doctor what do you recommend, if you needed to find a Dr what steps would you take for yourself?
KathyS
Hi Dr Luks
I had a labral tear derbrident one year ago and continue to have deep, aching anterior pain. I have worked hard on core and gluteal pain and try to avoid hip flexor strain. I also have L4-5 disc bulge with foot numbness. I am scheduled see a local orhopod to see if there is something else that can be done. Do you think tendonitis/bursitis could be the culprit? Thanks for your great website. BTW I’m a physical therapist so you can imagine how frustrated I am!
Christopher
Thank you for such a wonderful education on this malady. I am a 55 yr old male. I was in great physical condition before lifting injury. MRI indicated posterior labrum tears on both sides. Pain is manageable, not acute. Initial injury was three months ago.
I used RICE, somewhat successfully, and believe that it was healing quite well with a short period that I did not use crutches, however, going to PT on crutches was unbearable, further irritated condition and I’m afraid I’m back at square one.
I am on my own for a while now and was unable to refresh frozen gel pads for posterior glut relief. I noticed that Chinese methods do not believe in cold therapy to diminish inflammation. After inflammation subsided briefly I am self administering gentle massage to promote blood flow. I am worried that injury will never fully recover, on its own or via surgery?
Thank you again for sharing such valuable information.
Christina
Hi, I am a 27 year old female. I used to run long distance but gave that up about 6 months ago ( not for pain reasons but to preemptively protect my joints). Now I swim and walk. I am 5’9 and weigh 124 lbs. For the last 2 months I have been experiencing a pain near my tailbone that is aggravated when I sit for long periods of time or drive long distances. Flights are a nightmare.
More recently, in the last month, I have been experiencing a low back pain literally where my back meets the top of my buttocks. The pain is about a 4 (on a scale of 1-10) and sometimes is worse at night. The pain also seems to happen near my groin and outside hips. I noticed that one week the pain subsided and then when I began squatting and doing lower body exercises the pain at night was uncomfortable. It feels as though I want someone to deep tissue massage my hip/buttocks area.
Firstly, I think I have a deviated sacrum which I am interested in knowing what options I have for relief. My physical therapist said he noticed a slight deviation to the left, but just ever so slight.
Secondly, my hip/buttocks pain has not affected my flexibility or range of motion. When I saw my physical therapist he was surprised that I was able to perform so many stretches with ease. It just feels like sometimes after I do squats or intense leg work my hip and buttocks/lower back will hurt later. I have never felt a sharp or radiating pain while working out.
I have eliminated running and swim 3 times a week. I have no pain while exercising, just later.
I take a Rx NSAID but I would like to find other forms of relief.
Marc
Hi Dr.
I am wondering if you can tell me what exactly causes muscle pain in the inner thigh when one is diagnosed with labrum tears and FAI? Are there exercises or stretches that can get rid of the muscle pain? Can massage help? Thank you.
There are many causes of groin pain… and FAI or labral tears is only one cause. My site has a post on groin pain in athletes. PT can help many… if performed properly.
Susan Gordon
Where I live I do not believe the surgeons will perform hip arthroscopy for labral tears for individuals my age (55 – 60 years old). Is this common? Is it common for surgeons to operate on this age patient if they are in pain but not needing total hip replacement?
Usually by our age there is enough arthritis that the surgery will not work … although – this is certainly not the case in all patients — but tread lightly before considering an arthroscopy for labral tears.
Zaneta T
I’m 41 years old and have been suffering with Labral tears in with hips along with osteoarthritis in both hips, I also have a history will lower back injuries. On Dr for my hips didn’t work to do surgery until a spine Dr looked at my x-ray and MRI for lower back. After viewing reports, I was sent to physical therapy, which did nothing because of extreme pain. Does surgery look like possibly. Have gone to pain management, had injections in both hips and back and nothing seems to work anymore. Need you help to decide my next medical move. Z.T
Dee Lytle
I am looking for a hip surgeon that can do a hip labral tear repair in Oklahoma for someone with Ehlers-Danlos Syndrome. I have labral tears in both hips and currently unable to sit, stand, or walk more than 15-20 minutes. I have to use crutches for even that limited amount of time. I’m pretty much completely bedridden at this point. I look forward to your timely response, thank you.
Lara Provencher
My 15 year old girl has been dancing for 12 years and was recently diagnosed, after two years of hip pain, with hip flexor tendonitis and torn labrum. I am not finding a lot of information about surgically correcting both during the same surgery, possibly. What are the general pros and cons of this. I am researching so I can go into pre-op with some understanding of what I am approving my child to go through.
Adam M. Lazzarini, MD
The torn labrum is often associated with iliopsoas tendonitis. That’s the flexor tendon’s medical name. The labrum can be repaired using a truly minimally invasive technique with a scope. Sometimes the tendonitis will improve without intervention once the labrum has been treated. Alternatively, a release can be performed. I only recommend this if absolutely necessary because of the potential for slightly decreased flexor strength in an athlete. Before surgery, I would have the tendon bursa injected to determine how much of her pain is coming from that vs. the labral tear. If the tendon is to be released, it is easily done at the same time as the labrum.
You can see arthroscopy of the hip on You tube.
Hip scopes have become a commonly performed procedure with very good results. Make sure you are seeing an arthroscopist with experience who does this procedure often. Best of luck.
Derek Ochiai, MD
Normally, the hip flexor tendinitis is secondary and because of the labral tear, and should improve with therapy after potential surgery.
janeth
My 14 year old just got diagnosed with right hip labral tear. She started with pain when she was around4-5 years old but never had a big injury that we remember we were told it was growing pain. My question is being that young how is it possible for labral to tear?? She didnt do any sport growing up do to pain. Thank you
Derek Ochiai, MD
Since most labral tears are from either FAI or hip instability, it can sometimes affect people in their early teen years, and have treated patients as young as 12. I would have her see a sports medicine physician for work up.
Gelsey
Hi. I am a 32 year old female. I have been active my whole life, dancing ballet and modern since I was a kid. I stopped dance in my early 20s, but I have taken up running since then, usually 4-5 miles on a treadmill, 4-5 times per week. In June I developed ITB syndrome in my right knee, so I picked up the elliptical to stay in shape, at fairly high resistance. The ITB issue resolved and I started alternating running with elliptical a couple months later. Starting in September I noticed reduced ROM in my left hip. I have significant pain with external rotation, particularly if the hip is flexed and abducting. I can’t sit Indian style or in butterfly (feet together, knees to the floor) without horrible pain. I also have some pain with walking when my leg is extended back. No pain with general weight bearing though. I used to be so flexible, and now I feel like my left hip is so restricted. Pain is usually in the medial thigh and groin, but sometimes radiates to the knee. I’ve stopped running for several weeks and ramped down the elliptical resistance significantly, without improvemen. I got an MRI arthrogram that showed mild stress reaction/bone marrow edema in the superior pubic ramus without fracture, small joint effusion, and a superior anterior labral tear. My Ortho wants to take a conservative approach and seems to think the bone marrow edema is the source of most of this. I am a physician myself and I know labral tears don’t heal. I’m an active woman and I feel like my quality of life has been compromised, so I was actually eager for him to operate. He’s a specialist in arthroscopic surgery, so I was shocked that he didn’t even mention surgery. In fact, he said he wanted to hold off on injecting me to see if this gets better. He sounded pretty confident that the labral tear was not the main cause of pain. Could some mild bone marrow edema in the ramus really cause months of pain and stiffness like this? He said it’s evidence of stress and the acuity of my pain fits more with this than the tear. Thoughts?
Derek Ochiai, MD
A conservative approach to start is usually a good idea. Once marrow edema resolves, and if symptoms persist, then hip arthroscopy may be a reasonable option.
Derek Ochiai, MD
Depending on how severe the dysplasia is, PAO may be the best option. Would probably be worth it to get a second opinion from someone skilled in hip arthroscopy, as arthroscopy in the setting of dysplasia is technically difficult.
Dana
Hello. I am in need of some advice concerning my 15 year old daughter. She has had hip pain for 4 months and has been using crutches due to the pain. Xrays, MRI, and hip arthrogram show very mild hip dysplasia and a slight labral tear. Because her foot is getting cold/numb, she had an EMG and pelvic/spine MRI that were normal. A steroid injection in her back and hip did not relieve the pain. Her ortho was discussing doing a PAO but not sure that would help bc her presentation is not clear. Do you have any opinions or comments on PAO or other suggestions for the root cause of her pain?
Thanks
Patrick
I am almost two years post hip arthroscopy for a cam/pincer impingement and labral tear and I am once again experiencing pain in the affected hip area. I cannot stand on my feet for more than 20 minutes before pain (7 out of 10 scale) sets in or if I go out for a run, the hip will become tight after 2 miles or so with varying sharp pain occurring sporadically during the run.
After running the hip will be sore (6 out of 10 scale) for a few hours before the pain finally subsides (as long as I stay off my feet). I had significant arthritis in my hips prior to the surgery and I am fearful that I have re-damaged the hip due to running and may now need total hip replacement. Is this pain normal or is there a possibility I have further damaged my hip?.
Thanks
Derek Ochiai, MD
I would absolutely follow-up with your surgeon and get repeat X-rays. FAI surgery may slow down the progression of arthritis, but it cannot reverse an already arthritic hip.
Daisy
Hi Dr., 3 years ago I was treated for an external snapping hip… after that open surgery, I developed an internal snapping hip which has been ongoing. I’ve had several x-rays and one CT scan.. all showing nothing abnormal, and no signs of arthritis to speak of… I guess that has always been good news, however, I have been in pain… almost daily. The groin is not always that painful, it feels more like a pinch.. but deep pain in the gluts and the lateral hip (and KNEE!!) with weakness. Finally, last week after a MRI with contrast I’ve been diagnosed with a torn labral.
The MRI reports call it a “horizontal cleavage tear in the anterosuperior Labral” 1:00 and ending at 3:00 with a complete transverse tear, and slight separation from the acetabular bone. I’m not sure what all this means…
I was referred to a surgeon by my ortho-surgeon who said no one in the area really does this surgery. I traveled and met with the new surgeon, who said I was a candidate, but not “ideal” because I am over 50 (I’m 54). Can you shed some light on how bad a tear I have and your experience with patients over 50.
Thank you!
Derek Ochiai, MD
Daisy, while most of my patients are more in the 16-30 age range, I have several patients I have treated successfully over the age of 50. The oldest one was actually 73 years old.
Kita
Hi Dr. Wow! It’s amazing to see how many ppl are suffering from the same issue. I’m 38 yrs old Like others I’ve had pain in my rip hip, I saw a ortho Dr last year he gave me an X-ray then suggested therapy I did that to no avail… This year pain still was persistent my Internal medicine Dr sent me for a MRI which revealed I had a partial thickness tear in my labral and I had moderate cam type FAI along with tendinitis and bursitis in both hips. Bac to the Ortho Dr Now I’m waiting to get an ultrasound guided steroid injection in my groin on Dec 21 but the pain is starting to affect my daily activities and now my knee is in constant pain and starting to give me problems …. What is the likeness that my knee problem is related to my hip and what do u think ( just a guess based of what I told u) would or should be my next course of action??
Derek Ochiai, MD
Hip and knee issues can play off each other. Also, hip pain can refer to the knee, so it is likely that the knee pain is in some way related to the hip (unless you have a separate knee issue). See how you feel after the hip injection; if knee pain goes away, then it is definitely from the hip.
Kate
I was diagnosed with labral tear few years ago, prob at least 3 Haven’t gotten surgery. Most Physical activity makes it hurt, along with long sitting. Pops and clicks. Worried about surgery, read stories of it not helping pain. Also seems like will be out of work for while. How long is recovery?
Derek Ochiai, MD
For my patients, normally crutches for a couple of days up to two weeks. Physical therapy for 8-10 weeks. Normally, it is THREE MONTHS before the patient feels significantly better than before surgery.
sharon
Thank you for your information… it was very helpful and answered more of my questions that I had. I just received a hip injection for the bursa and acetabular labrum tear.. I’m excited for tomorrow I will be more ease from the pain …once again thank you
you’re welcome!
Alan
Dr Luks
I have a labral tear and paralabral cyst. I had a cortisone injection and had the cyst aspirated. The surgeon won’t do a labral repair because of arthritis. He said I may have a few more years before I need a hip replacement. In the meantime, I’m really having a hard time with the pain from the the cyst. Can this be excised? Thanks for being so generous with your time.
Alan
Derek Ochiai, MD
The paralabral cyst is because of joint fluid leaking out the labral tear. the cyst itself does not cause pain; it is only a marker that there is a labral tear.
Christina
I have suffered hip pain for 10 plus years, this last year being the worst and continuous unless I have a cortisone shot. I recently had an MRI and it has shown I a full tissue Labral detachment, how is this different than a tear. I have been told to restrict physical activities until I see surgeon
Derek Ochiai, MD
Detachment and tear are exactly the same thing.
Helaine Pfaff
Doc, I’ve had debilitating left side sacral/buttocks pain for several years. It started localized at my SI joint and progressed to hamstring and back of leg. After multiple X-Rays, MRIs and injections of lumbar and SI joint, I could never get a definitive diagnosis of any spine or SI related cause. Saw many ortho and neurosurgeons.
X-rays of hips were normal and never had classic hip/groin pain but after exhausting all other causes, I insisted on an MRI of hip and a Labral tear was seen. Then a CT scan showed FAI. I had hip arthroscopy for Labral tear and bone shaving to correct FAI 6 months ago. I have had slight improvement of buttocks/hamstring pain since surgery (except upon waking when it’s excruciationg). Unfortunately I have developed more pronounced hip pain, quad and knee weakness since surgery. 6 months out from surgery this seems worse than at 4-5 months.
Questions are: 1/ do you see patients presenting almost exclusively with posterior pain as a result of FAI? Does surgery often resolve this, or rarely? 2/ why would hip and frontal issues surface after surgery?
Thank you
Derek Ochiai, MD
Posterior hip pain as a presenting complaint is about less than 10% of cases, so it does happen. If pain (wherever it is referred to) resolves with a cortisone injection temporarily inside the hip joint, then surgery is usually successful. Not sure why your pain is worse at this point, as normally you should be on the mend by now.
Elizabeth
Doc, I am preparing to undergo a hip labral surgery for tearing and fraying and have had X-rays and MRI/mri arthrogram. I am concerned about possible impingement that isn’t present in the X-ray or MRI….will they still check for it when doing the surgery or should I have a CT prior to to be sure? I failed to ask the doctor about this at my last appointment and I really am concerned we will repair/debride the labrum only to have it happen again not realizing there is an impingement that caused it in the first place. Thank You
Derek Ochiai, MD
Normally, I can pick up impingement based on specific X-ray parameters, so it is possible that your surgeon has already checked for that?
wendy
Hi just to say i found this very interesting, i have had x 2 xrays 1 standing 1 laying down, a ct scan, an mri scan i have being going to the GP to state i have pain whilst having sex for the last 12 months, after all this i finally have a diagnosis a anterosuperior labral tear, after reading this its exactly me, i have also back pain but as i have had a spinal fusion i thought it was that but the fusion was 18 months ago, so this eased my worries.
Thank You
Derek Ochiai, MD
Glad you liked the article!
Sam
Hello, 46 year old male that was diagnosed with FAI with labral tear under MRI. Pain can be an 8 and is definitely worse in the morning, and told that I have mild arthritis in the hip joint. I haven’t had a cortisone injection yet. Can the arthritis get worse if I don’t get the arthroscopic surgery due to the deformity of my bone? My goal is to avoid a hip replacement down the road. Thanks!
Derek Ochiai, MD
8/10 pain is definitely severe. Hip arthritis can progress with or without hip arthroscopic preservation surgery. There is some basic science studies to suggest that hip arthroscopic FAI surgery may slow down progression of arthritis, but my main reason to do surgery is to improve function and decrease pain. A cortisone injection is definitely “worth a shot” (pun intended).
Nikki
This article was very helpful! Thanks so much! I am 30 years old , and my younger child is 9 months old. I am (was) very active, including doing Zumba several times a week (even throughout my entire pregnancy.) About three weeks ago, I noticed my left hip starting to get sore. It got progressively worse over the course of a week, to the point where I literally could not sit down or move it at all without excruciating pain all around and within the hip socket. The muscles felt like they were spasm-ing and caused most of the pain, but the joint itself also throbbed. There was about a week where I could not do anything without causing pain so bad it made me cry. After an MRI and visit with a specialist, I found out I have a torn labrum as a result of FAI, and that surgery is my best option. I now have slightly better range of motion and less pain, (I’m assuming the muscles are healing) but am curious as to why I have never had any hip pain previously if I have had FAI? (The xray showed calcium deposits by the tear as well, so I don’t think the tear is new). Since I’m approving on my own, should I reconsider the surgery?
Derek Ochiai, MD
Nikki,
Any time a patient feels like they are getting better without surgery, then I advise them to wait to see where their hip pain settles out at.
FAI can cause labral tears, but it is possible that you FLARED a pre-existing labral tear, and that it is calming back down to baseline on its own.
Jill
A few months ago i was injured at work I was knocked backwards and took quite a fall. Since then i have had tailbone and right hip pain. The tailbone area has stayed about the same but the hip area has been constantly increasing in pain to the point where i am limping and can barely walk. The doctor sent me to physical therapy but she would not start until I had an arthogram mri to check for a labral tear. It came back “normal”. I have a sharp stabbing pain in the crease of my pelvic area (exactly where the dye was injected) random shooting pain the extends a few inches down my thigh, pain and pinching sensation on the side of my hip and about two inches above my knee plus a dull ache below my buttucks that at times has a tingling sensation. I’ve also havent had a normal bowel movement since the injury occured but none of the doctors find that last part to be of any concern. Any insight would be greatly appreciated! Also, the orthopedic never even opened the mri cd and didnt even take it-is this common?
Derek Ochiai, MD
I would probably see a spinal surgeon, to make sure that the pain is not from your back (as back pain can radiate to your hip). Personally, I read ALL MRI’s myself, but I can’t speak for everyone.
Brenda
Thanks for this explanation. I’m wondering if there is a role for physical therapy +/- steroid injection for my situation:
I’m 44 years old, active. Left hip pain with exercise (running, brisk walking, now even with spinning) also with sitting for prolonged periods – getting worse. NSAIDS and activity modification have not helped so far, but haven’t done PT yet.
MRI arthrogram shows degenerated labrum with many internal tears, no discrete external tears, some synovitis, very mild CAM. Xrays hip, pelvis, lumbar spine are all normal – no arthritis
I’ve seen two hip trained orthopods. One is suggesting straight to surgery (repair v reconstruction depending on what he finds in there) and the other suggesting trial of PT with steroid shot. I’d like to avoid surgery if possible, but also don’t want to delay the inevitable. I do want to be aggressive about doing whatever I can to prevent arthritis in the joint and need for THA down the line.
Derek Ochiai, MD
I nearly ALWAYS try physical therapy first. There are many people with asymptomatic labral tears, and if therapy can make you one of those people, then try that. I use cortisone injections as physical therapy aids often. if this fails, then surgery may be the best course of action.
Vince
Great video! I am interested in the relationship of Labral tears and FAI to Runner’s dystonia which have been diagnosed with. 3 primary injuries 10 years ago as an Ironman triathlete all affecting the left side.(!) speared in the left mid-back while on stride at the start of a marathon by a falling runner (2) freak occurrence of a broken spoke on a five spoke rear wheel causing it to go out of round and wearing down the brake pad over 52 miles of racing and (3) ankle sprain.
I never had a full recovery. Could not bike due to left toes digging into cleats and ankle not flexing during the pedal stroke, yet could pedal backwards with no problem. Inside hip felt “off” and left leg slightly unstable. was able to return to running with underfoot stretching 3-4 times at beginning mile or two and consciously keeping my leg/foot from turning in.
Ran a marathon 2 years ago. 9 months ago training for a marathon fine, took a break, returned to training and foot stretching did not allow running, rather suddenly felt left leg/hip lose control and feel like the “strings broke”. Walked home, walking fine for miles after. Sough PT which was very aggressive and within weeks I could not take a step without all toes curling under and at time foot curling. Can walk on toes, backwards, just as the cycling was for the past 10 years.
Hip MRI result:
Small osteophytes are seen at the sacroiliac joints. There is no evidence
for edema, sclerosis or fusion. The symphysis pubis appears normal.
The alpha angle of the left femoral head is increased at 67 degrees
(series 7, image number 10). There is a tear of the left acetabular
labrum (series 8, image 17). There is no evidence for hip effusion.
Increased signal is seen at the insertion site of the gluteus medius
tendon on the greater trochanters bilaterally (series 5, image 15).
Otherwise, the pelvic and hip musculature appears normal. Except there is
mild prostate enlargement. There is no evidence for lymph node
enlargement in the pelvis.
several orthos state Labrum tear and FAI cannot account for sx and runners dystonia Dx. Yet, outer hip flexor pain by day and inner hip pain upon awakening during the night. Referred to movement disorder clinic.
I am concerned the hip issues are being dismissed prematurely. I have trouble walking and moving my hop forward close to my torso which interferes with my foot plant. Runner’s dystonia and task specific dystonia seems poorly defined dx with at best an hypothesized cause. Any reason to explore hip function further as cause of foot symptom or contributing to it. If so , what do you suggest?
Derek Ochiai, MD
Have you tried a cortisone injection to your hip, to see if that helps your symptoms at all?
Nicole
Hello, I am a 20 year old female US Marine who was diagnosed with: partial labral tears in both hips, sciatic inflammation, piriformis syndrome, and gluteal strain. My sports medicine doctor said that she didn’t want to have me do the surgery and would rather have me do physical therapy for 6 weeks because the surgery has a low success rate. Shots are not an option for me, as I am suspected to have low bone density and have a history of stress fractures in the last 2 years (7 to be exact). So, basically, I was given ibuprofen and physical therapy to treat my injuries. I’m constantly in excruciating pain, and have bouts of muscle weakness that usually leaves me unable to walk. Sometimes it’s both hips at once, and I’m quite literally brought to my knees. I don’t know if I should seek out a second opinion, or if I should listen to my doctor without question. I’ve had this injury since early 2014, have had it misdiagnosed as lumbar lower back pain and a hip flexor strain, and I don’t think I can take it much longer. I’m at my wits end, what should I do?
Derek Ochiai, MD
Nicole,
Hard to get a complete picture without examining you, but typically physical therapy is a good start. If this doesn’t help, then sometimes surgery is necessary. For the labral tear, the surgery is usually very helpful, but if symptoms are sciatica, then sometimes hip surgery does not help. Sometimes, an inside of the hip cortisone injection, to assess pain relief, can be helpful.
Karen
Hi, My daughter is a highly competitive lacrosse player and had a mri showing a small labrum tear on right hip. will stem cell help repair this or are we wasting time and money?
Derek Ochiai, MD
Karen,
In the vast majority of labral tears, there is underlying FAI. If so, this would fight against any increase in healing response with either stem cells or PRP, so the likelihood that it would help is small.
Kim
Hi Dr Luks. I am 46 tore the labrum in my right hip slipping over last Dec. I was in tremendous pain until I had athroscopic labral tear repair surgery 11 weeks ago. However I am still on both crutches. Every time I try to just use one crutch I end up in severe pain in my groin a while after. This pain will extend down my inner thigh & sometimes around the knee also providing discomfort to several areas of my foot & ankle. I am cycling every day water walking in the pool as well as doing physio exercises from my surgeon. I am told my hip is perfect after re xray from surgery I have good strength in the hip & buttock (prior to surgery I couldn’t squeeze my right buttock) & legs.
Why am I taking so long to recover & get off at least one crutch if not both? I was told maximum 4 weeks both crutches. Why would I be in so much pain still? If you could post suggestions I would be very grateful.
Derek Ochiai, MD
Kim,
Recovery is definitely longer than expected. Perhaps you should talk to your surgeon about possibly repeating your MRI.
Anne
Ok I’ve got a weird one. Hip pain for many years, clicky, stiff, variable range of motion, etc. I always instinctively knew I had a problem but didn’t see a doc because it was never bad. Well in the last couple of years it got bad but the weird part is what triggers it: sleeping on my side (opposite side of affected hip). First time was while out camping. Had to cancel and go home due to waking up unable to walk normally. Second was so bad it was 911-esque and all I did was go to bed, but admittedly my hip had been bothering me a lot the previous day (stiff and achy but that often happens after sitting so I ignored it). Got xrayed and FAI turned up. Waiting for MRI to get booked and to start physio. But I have questions.
1. I live an active lifestyle but my worst symptoms start when I sleep. Has anyone ever heard of that?? (If I’m lucky it will wake me up before it gets super bad, but I’m not always lucky)
2. I went from a 10 (uncontrollable crying, unable to walk at all) to a 1 on pain in a matter of only a couple of weeks. How is that possible? Granted there were some strong NSAIDs involved but still, that strikes me as pretty fast. First time this happened wasn’t nearly as severe but it lingered for months. So what gives?
3. I feel like I’ll fall if I stand properly. The joint feels unstable. But I can’t figure out if that’s just a mental protective reaction to spare the sore side or if it really is unstable. The cognitive dissonance is resulting from a suspicious lack of injury that would obviously cause one’s hip to be weakened, such as a fall. How can I tell what’s going on? I know the therapist will be able to tell but I’m terribly afraid of letting them try. The pain is very positional dependent. If they try to get it into position to check for tears, there’s a 50/50 chance I’ll scream (or feel nothing – it’s weird that way).
I’m starting to wonder what shape my labrum is in. I hope the MRI will help with that. I initially assumed this was bursitis and just self-treated but I minimize my own symptoms because I dislike having to deal with them unless they can’t be ignored. But sometimes I wonder if I just got unlucky enough to get a bunch of things at once. Can tears hurt this much and suddenly flip the pain switch off?
I’m curious to know if either of the doctors here has seen patients get tears due to sleeping position. This is really maddening because my favorite sleeping position is what does me in. It’s both hilarious and depressing at the same time. I’m not sure how to deal with it.
I presume I’ll get talked to eventually about correcting the FAI. Right now it’s a bit difficult because there are no specialists involved and the diagnosis is basically being radiologist driven. I just showed up on a random doctor’s doorstep with cane begging for crutches and painkillers. I kind of feel badly for having dumped myself on them like that. They were kind enough to take me in but I’m probably a bit of an overwhelming case for them.
Derek Ochiai, MD
Anne,
The MRI will be helpful. Pain from labral tears can wax and wane, depending on whether the labral tear is irritated at the time. NIGHT PAIN can be from FAI, but it is more commonly from early arthritis, which can be caused by FAI.
Renee N.
I have had hip pain since giving birth 15 years ago to a 10 lb baby – I am having the MRI with dye soon. Have you had injuries like this with child birth?
Thanks
Derek Ochiai, MD
Renee,
Yes. I have definitely seen pregnancy associated labral tears. It is a combination of increased ligament laxity and sometimes during delivery, the hip over extends and over rotates. Good luck with your MRI.
Tammy Kraushaar
I work in health care and have spoken to various physicians- they believe that Ortho waits until THR is necessary at an older age. Labrum tear repairs are not usually done- not sure why? low success rates? (cost?) I’m in Canada- so I mean cost to the system.
None the less I haven’t seen the Docs yet, so will listen to their opinions and treatment recommendations. I’ve heard that one uses stem cell tx.
Any feedback would be helpful. There are no pieces missing. I have no OA, just a tear that causes me pain and limited mobility. it’s been going on for more than 6 months- did not kayak or cycle all summer- now winter is coming and I love to skate ;(
Tammy
Tammy kraushaar
hello Dr Luks,
I have a labral tear that extends from the superior lateral to the anterior superior labrum with no femoral acetabular impingement.
Where I live the Ortho Surgeons don’t like surgical repair for women in my age group. I’m active, fit and in my 40’s. Do you know much about intra articulate injections or stem cell tx?
The sports med Doc is at a bit of a loss. She referred me to 3 different Ortho Surgeons for treatment advice.
Would appreciate your feedback.
Tammy
I do not understand why.. there might be something else to the story??
Derek Ochiai, MD
Tammy,
I’d get another opinion. Hip arthroscopy is a procedure that people do travel for.
Tammy kraushaar
I’m waiting to see 3 Ortho specialists here, just doing my research before seeing them. Surgical option (repair) doesn’t seem like a promising recommendation. Will keep you posted.
Tammy
Shelby Waldron
Dr. Luks,
I am a student in Oklahoma attending Radiology school, I am doing a pathology report on acatabular labral hip tears. I was diagnosed with this condition back in 2010 & had it surgically repaired twice. I am commenting to ask for your permission to use your photos on this website.
Thank you for your time.
Andy Friestam
Thanks for this article and the detailed responses. What is the medical opinion on PRP and Stem Cell therapy on and around the Labrum as a way to regenerate the tear to avoid surgery? Also with time is it possible that the tear if not severe can heal on its own if you have mild FAI??
Derek Ochiai, MD
Andy,
My thoughts on PRP/stem cells is that it is unlikely to stimulate a healing response when there is concomitant FAI, as the tension force of the FAI is opposite the way the labral heals to bone. While labral tears do not heal on their own, they can become asymptomatic, especially with physical therapy focused on gluteal strengthening.
Mary-Jo
Hi Dr. Luks, WHY is it so hard to find a surgeon that does arthoscopic labral tear surgery? I had a terrible experience with a surgeon, and I can’t seem to find another surgeon that does the surgery. I am so upset and in pain. :(
Derek Ochiai, MD
Mary-Jo,
Hip Arthroscopy is a highly subspecialized field. You really want to have a surgeon who does this type of operation all the time.
Tanya
I was diagnosed in 2013 with a labium tear in right hip, meniscus tear in right knee and a Baker’s cyst in same right knee. I was in process of gyno surgeries when diagnosed with the tears. It was decided that I get the gyno surgeries and heal from them and return. I have had the dye, shots and May 2014, I had the FAI and the arthroscopic to repair my labrum. Once inside my hip, it was discovered that my rips eight months prior were not repairable any longer. I was supposed to complete physical therapy but my personal life was experiencing severe crisis. My half of my home burnt down while I was in the hospital. I was living separated he in the front and me in the back. I was planning on leaving as soon as I healed from the hip repair surgery. Long story short, I had so much pain, internally, emotionally and mentally and could not work, could not afford physical therapy at $60 per week for eight weeks. Had no support system from X, I began walking as far as I could, I bought a bike and ride twice a week for short periods. This week after walking and/or biking, I have had very bad stabbing pains in hips, lower lumbar and deep inside buttocks. My left side as well from withstanding the extra weight the right side cannot handle any longer.
My surgeon said without the physical therapy or a hip replacement, I would have an 85% chance of being in a wheelchair. I take Mobic once a day and occasionally when its real bad, Tylenol 3 or Vicodin. I am progressively getting worse. Now my left hip is stabbing me and I have been having buttock stabs, right shoulder pain, at times so severe pain medications don’t help. My left knee locks up now. I am literally falling apart. I am scared to have a hip replacement because of all the lawsuits I have read about.
I am 51, had three ten lb girls, I was extremely active physically growing up. What do you think about my situation. I was thinking about going to Shands in Gainesville, Fl for a second opinion. I don’t qualify for pain management because I admitted medical marijuana use. It helps me get my mind off the pain and move. I fear the pain and the meds are not working as well now. Without pain management I imagine wanting to die from being so tired and the living with pain. Where are you located? Can you tell me your opinion based on my short book. lol Thanks
I am ready to fix my battered bones. I have transitioned into my independence and divorce just became final. I am afraid both hips and both knees are going out at the same time. Help in Florida! Thank you!
Linsey
Thanks so much for this informative article. My 17 year old daughter is super active with swimming and running has been complaining of hip pain now X6 months and is getting worse. I have suspected she has a labral tear as she complains with deep groin pain sometimes radiating to the lateral thigh, as well as feeling like her hip is “coming out” at certain times. Your article has shed even more light on this. Thanks for sharing your insight and experience in a very clear, concise manner….
Derek Ochiai, MD
So glad you liked the article!
Jen
My daughter has a 1.5 cm tear in her labrum as well as fraying and tearing of the ligamentum teres. She is a competitive gymnast. Her chiro says that she needs to quit gymnastics immediately. Do you feel this is good advice?
Derek Ochiai, MD
I take care of high level gymnasts, figure skaters and ballet dancers all the time. If she is having significant pain in her hip, I would recommend temporarily stopping gymnastics while seeking the opinion of a highly trained hip arthroscopic preservation surgeon.
Lori B.
I have had 3 steriod shots. One in L-4, One in L-5 (no relief) My last one was on 9/2/15 not sure the name of this one. It was given to me if I may be frank, right at the top of my butt crack.. It will be one week tomorrow. I did get some relief but now I already feel like it is wearing off. My last MRI says my right hip has a small anterior superior acetabular labral tear. After reading this, do you have any suggestions on what I should do next, Am I a candidate for this surgery. I know you should only no more than 3 steriod shots in one year. So I have reached my limit. What do I do now?
Thank you.
Derek Ochiai, MD
The limit for cortisone injections is per body part. You MIGHT be able to get a cortisone injection inside the hip joint, to see if this alleviates your pain. If it does, that would argue that your labral tear is symptomatic. However, many times patients can have a labral tear on MRI and it is just a coincidental finding, and not the cause of the pain.
Anna
After having a synovectomy, labral repair, and FAI repair- I have had issues with my SI joint and sacrum/lumbar pain specifically when bending over. Is this common and what could be causing this pain?
Jeff
Recently diagnosed with a torn labrum, CAM impingement and moderate hip arthritis in left hip (29 years of age and triathlete) Doc told me I would really never run distances again as the cartilage in my hip has been damaged and will eventually need a THP. Will FAI surgery delay my need for a THP as my femoral head will not rub against the cartilage? Is there any benefit to doing FAI if I have moderate cartilage damage already? Thank you and great article!
Derek Ochiai, MD
Glad you liked the blog! Given your activity level and age, it would absolutely be reasonable to consider hip arthroscopic preservation surgery. In biomechanical models, FAI osteoplasty decreases pressure on the articular cartilage. You should see someone who subspecializes in Hip Arthroscopy, for their opinion on your specific case.
Jeff C
Just diagnosed with a torn labrum, a cam impingement, and moderate arthritis in the hip (29 years old triathlete). Doc told me I will eventually need a THR in my left hip and even if I have FAI surgery to fix impingement and labrum, running long distances will never again be an option due to cartilage wear (as it now hurts running even a mile) Will having the surgery at least delay the need for a THP? Will it keep my femoral head from rubbing against the joint, thus diminishing cartilage wear? If not, should I just wait to get a THP?
* Article was great! Thank you!
Penny
Dr Luks, may I commend you on a wonderful presentation of this problem. it is clear, concise and the pix are wonderful. And it seems like you covered all of the pertinent points. Even I could understand it.
I have been experiencing the exact symptoms you have listed. At this point my pain is so agonizing that I can not sleep at all. The pain has actually made my entire leg and sometimes feet sore. I am scheduled for the MRI with contrast. The information you have presented will allow me to make an informed consent when/if the diagnosis is confirmed.
I suspect an orthopedic surgeon would be expected to do this type of repair. Would a sports ortho be a better choice or would it matter. Having had numerous surgeries, I can attest to the importance of having just the right surgeon. Of all of the decisions one makes, this, to me is the most urgent. Also, what is the recovery time for this type of surgery and is it quite a painful recovery? I am a 67 yo caucasian female.
Thank you for your attention to this question~
Derek Ochiai, MD
Glad you liked my presentation! I would go to someone who is a hip arthroscopy specialist. These are NORMALLY sports medicine trained orthopaedic surgeons who then subspecialize in hip arthroscopy and hip preservation surgery.
Andrea G
I am 61 and before my pain started I was very active, aerobics, hiking, etc. After 4 years of undiagnosed pain, I was recently diagnosed with a labral tear confirmed by an MRI. I only have minimal pain/discomfort while walking but significant pain while sitting for any extended period which gets worse as the day goes on. I have had 2 consults and both surgeons recommended full hip replacement. One does the anterior approach and the other surgeon recommended direct superior. But neither surgeon mentioned Arthroscopy as a possible alternative. BTW – when the surgeons manipulated my leg, I only had minimal discomfort and both said I had excellent mobility for my age and condition.
Derek Ochiai, MD
If you have signs of arthritis on MRI, then hip replacement is the most reasonable approach. However, if the gliding cartilage of the socket is intact, hip arthroscopy may be reasonable. I would see a surgeon who specializes in Hip Arthroscopy, for their opinion.
Reginald
I am a 26 year old male, loves mountain biking and hiking. Had a hip arthroscopy 1 year ago, but it the pain hasn’t gone away yet. Also had two cortisone injections over the last four months hoping that it will clear up the remaining inflammation. No luck I guess. What’s the next step? MRI again or going in with a scope to see what’s going on?
Thanks in advance!
Doug D
Can arthroscopic surgery repair a completely detached labrum.
it can
Derek Ochiai, MD
Absolutely. I repair detached labral tears of the hip all the time.
Derek Ochiai, MD
I repair completely detached labrums all the time.
Jena Pendergrast
I’m a distance runner that has been experiencing pain in my left hip for over 2 years. I was recently with a labral tear and had a cortisone injection but did not see any relief. When I spoke with my doctors PA, she reminded me that if I didn’t see relief with the shot that I probably won’t feel better after the surgery, that my pain is coming from another source. I’m waiting to hear back from the Dr. I have not run in over 3 months and before that my last half was in February, when I took time off because of the pain and inflammation. What else is causing my pain? Is surgery out? I just want to get back to running, yoga and walking without pain. Thanks!
Derek Ochiai, MD
While a POSITIVE effect with a cortisone injection is encouraging, in up to 1/3 of patients, the cortisone injection does not help BUT the patient gets better with hip arthroscopy. Therefore, a negative response to a cortisone injection does not rule out surgery.
Starla
My son, an active duty Army Soldier, 31 yrs old just saw a military orthopedic surgeon who said his labrum tear was so extensive that he could not do the “fix.” He has referred him to another surgeon at another military installation. The first surgeon said the MRI indicated the tear was all the way around the joint/hip area. We have been told there is a Dr in Nashville who Is very successful with these types of repairs. The problem is we have been told the military insurance, Tricare, will not cover this. They claim this procedure is “experimental” and in most cases, doesn’t work. Any advice or suggestions you can offer will be greatly appreciated.
Desiree Bustos
Hi Dr Luks,
The result of my MRI right hip performed 23.10.14 demonstrated the following: an undisplaced labral tear involving the anterosuperior labrum and anterior labrum with mild paralabral cyst formation; mild trochanteric bursitis with tendinopathy of the gluteus minimus; and appearances consistent with underlying ischiofemoral impingement.
MRI lumbosacral spine performed 14.10.14 demonstrated L4-L5 disc desiccation with right asymmetric broad-based disc protrusion resulting in right subarticular recess narrowing with displacement and potential impingement of the traversing right L5 nerve root.
Right-sided gluteus minimus tendon injection performed in Dec2014, Jan-Feb2015,one injection each month.
The pain was only lessen after the injection but my pain is 24/7 even I’ve been having a physio therapy. I couldn’t sleep on my back and on my right side, I could only sleep on my left side. Prolonged sitting, standing, driving is killing me. Couldn’t drive more than 30 minutes as the pain is unbearable. Standing still for 5 minutes will give me pain so I couln’t stay still. I need to rest after standing/sitting after at least 20 minutes.The pain on my right lower back and right hip is terrible especially on my right lower back, it’s stabbing pain. And now the pain is going down on the right side of my leg. I have more pain now that even the endone pain reliever would only lessen the pain.
The winter even worsen the pain.From July 10-19 I was using crutches to help myself in moving around and I needed help in wearing pants, undies and socks. Now I am able to wear my socks without help but at times I needed help. The pain was only lessen but it only fluctuates from moderate to severe but it never goes to mild. Will it always be worse during winter. Please advise me on the best thing to do to recover totally.
Thank you very much.God bless you.
Desiree
Carly manuel
Desiree, I just read your history and problems about your hip. I have the exact same thing. Mine was diagnosed over a year ago. I have quit yoga because of pain and getting up and down is very difficult. My thigh, IT band and down into the shin is very very painful . If you get this, can you please reply ? I’m interested in what your outcome has been . How much was your surgery, if you did get surgery. And, rehabilitation? How long was it before you could work again ? And are you pain free today? I’m 61, and a massage therapist. I have to work as I’m single and I have no insurance! I appreciate any info you can give me or anyone reading this.
Thank you so much !
Carly
Mike Horowitz
i learned last week that I have a possible full thickness tear of the labrum in the left hip. I’m 51 and have been running and doing Triathlons for years. My question is what physical activities can I do or should not do in the next 3 weeks as I wait to see the Orthapedic specialist?
minimally symptomatic tears are very common at our age… especially with your lifestyle. Unless you have pain nothing will be necessary. Even with pain, it is still a quality of life procedure. That being said, most surgeons would allow their patients to remain active as long as you don’t have significant discomfort
Nikki Klinger
I was recently diagnosed with laberal tear in my right hip. Just relieved to know what’s been causing all this pain for so long. I’m also glad to know there is more than one option. Thanks for the help.
Ray Thaw
i have been told that having a laberal tear, untreated for 8 months has no bearing on AVN in any way. Can this be supported by fact or am I being hoodwinked?
There is no known link between a labral tear and osteonecrosis.
Sadie
I was recently diagnosed with bilateral acetebular retroversion and labral tears (the right is worse than the left). My orthopedic doctor says the cartilage and bones look very healthy. I’m 25 and have been living with the pain for 9 years (I have done physical therapy for a long time, and only recently had an MR arthrogram).
I’ve been working with a new physical therapist and riding my bike, which has greatly improved muscle strength and makes certain activities much easier, but I am still experiencing significant pain, especially at night and following long periods of sitting/standing/walking.
In your experience, would this be something I could have fixed surgically, or would the potential for complications and possible need for revisions make continuing with physical therapy and taking ibuprofen a better choice in the long run?
Hi Sadie .. You can find me on Curely where I can answer questions by text or email … Join me there. http://www.curely.co/
Derek Ochiai, MD
Sadie,
In my vast experience with treating your condition arthroscopically, the success rate is about 93%. Therefore, if your hip pain is significantly inhibiting your quality of life, I would go to a well qualified hip arthroscopic surgeon for their opinion.
Kirstie
Can a labral tear or pinch effect the ability to walk, lift the leg, and muscle weakness? For the past 8 months I have been struggling with extreme weakness and the inability to use one leg. MRIs, EMGs, and other nerve tests show no results.
Hi ! I would love to help you with your questions. You can find me on Curely where I can answer questions by text or email … Join me there. http://www.curely.co/
Howard Luks MD
Derek Ochiai, MD
Labral tears can cause irritation to the hip flexor (iliopsoas), because of the close proximity to the hip joint and the hip flexor. Therefore, some of these symptoms could be from a hip labral tear.
Lindsay
Hi Kirstie, I’m curious if you’ve made any progress with a diagnosis? I am dealing with something very similar to you, and have been unable to come up with any answers. Tx.
Cindy
I have Avascular necrosis, Ficat stage 2, as well as a tearing of the Labrum. I suspect my pain is from the tear, but am not positive. Would I still be a candidate for the repair, or does having AVN precluded me from this procedure?
Thank you!
Most would recommend to let treat the AVN (osteonecrosis) and watch (ignore) the labral tear for now. The pain is virtually always due to the osteonecrosis. But without examining you I obviously can not know for sure.
Chellie
I had an accident 5 years ago. I work with an airline, I twisted my left leg while stepping off a step. My left leg twisted to the left and my top of my body was twisting to the right looking for something to grab so I didn’t fall. In short, I ended up with an injury to my left hip. I had an x-ray done immediately and they thought I broke my hip but an Orthopedic surgeon said it was Trochanter Bursitis and tendonopithy (sp?) I had the surgery, but was left with inner pain in my left hip. In the last 2 years since the surgery I have failed to find relief for the pain. In addition my lower back is out and I have been trying to have injections to help this pain I cannot pin point. I was seeing a Chiropractor and he put me through a series of workouts and stabilizing exercises without help and that is when he ordered an MRI with Contrast with shows an Anterior Labral tear. Is it possible the Surgeon missed diagnosed it? And can you tell how long it has been torn?