Hip pain is becoming more common with each passing week. Similar to other injuries we see, people are more active and stay active longer. It has only been 5-10 years since we have started to identify a common cause of hip pain — Tears of the labrum in the hip. In addition, we have identified anatomical reasons why you might have developed a labrum tear in your hip. Unless though issues are dealt with, an isolated labral repair may not work.
This is a guest blog post by Derek Ochiai, MD. He is a Sports Medicine trained Orthopedic Surgeon with a particular interest focus on the hip.
Nowadays, it is rather commonplace to read about an athlete undergoing hip arthroscopy for a labral tear of the hip.
This hip pain post will review:
- what is a hip labrum?
- why is the hip labrum important,
- how the hip labrum tears
- what kind of treatment is available for hip pain due to labrum tears
What is a labrum?
The labrum is a rim of cartilage that surrounds the hip joint. It attaches to the socket of the acetabulum. If you have friends who had a knee arthroscopy for “torn cartilage”, they had a meniscal tear of the knee. The meniscus of the knee and the hip labrum are made up of the exact same type of cartilage.
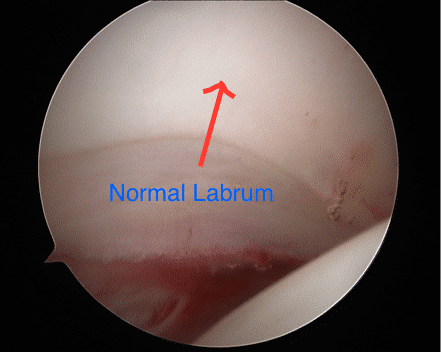
Figure 1: Arthroscopic picture of a normal posterior labrum. The labrum attaches smoothly to the acetabular articular cartilage. The femoral head is on the bottom right of the picture.
Why is the hip labrum important?
The labrum increases the relative depth of the socket, which can confer additional stability to the hip. This can be especially important in ballet dancers, figure skaters, gymnasts, and other athletes who put their hips through extreme ranges of motion. In developmental dysplasia of the hip (DDH), the socket is much shallower than normal, and the labrum deepens the socket to keep the femoral head of the hip in that shallow socket. Also, there are medical conditions where a person has increased joint laxity (such as Ehlers-Danlos), where the hip is more unstable and relies on the labrum for stability.
The labrum acts a seal around the femoral head, to maintain fluid pressure of the hip joint.
What are the symptoms of a labral tear in the hip?
The severity of symptoms can vary. The “hip pain” 90% of the time is perceived as deep in the groin. Sometimes, the pain can radiate to the side or the back of the hip as well. Many times, patients with a labral tear have pain and/or a feeling of catching in their hip, especially when going from sitting to standing. They may notice that they have to compensate to get in and out of cars. They may have pain with squatting and exercise, especially with sports that involve cutting and changing direction. Many times, patients also complain of pain with sex.
I didn’t injure my hip. Why do I have a labral tear?
The vast majority of labral tears are from FemoroAcetabular Impingement (FAI). FAI is a condition that develops in a person’s early teen years, where the hip is “out of round”. Since the hip joint and labrum are meant to function with round on round mechanics, this out of round conflict puts increased stress on the labrum. Over time, this increased stress can cause the labrum to tear. Symptoms of FAI greatly overlap with labral tears. In addition, symptomatic FAI can cause pain with prolonged sitting.
How is a labral tear of the hip diagnosed?
A medical professional can suspect a labral tear based on a patient’s symptoms and history. Clinically, the doctor can do provocative tests, such as the anterior and posterior impingement test, the McCarthy test, and the FABER exam, to further investigate. Many times, X-rays are very useful. FAI is a radiographic diagnosis, and usually can be easily seen on plain X-rays. With severe FAI, a labral tear can be inferred.
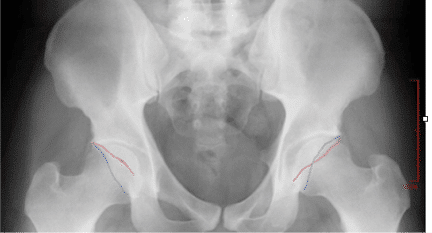
Figure 2: On left side of screen, normal acetabulum. The anterior wall (red line) and posterior wall (blue line) do not cross. On right, there is pincer type FAI, where the red and blue lines cross.
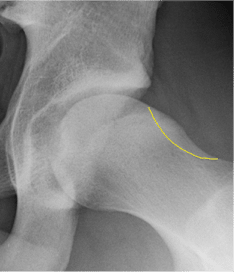
Figure 3: Typical cam type FAI X-ray finding. The yellow outline shows what the contour of a normal hip would look like.
MRI (magnetic resonance imaging) directly shows the cartilage of the hip. While a labral tear can be diagnosed with a plain MRI, an MRI arthrogram is more sensitive to labral tears. An MRI arthrogram does involve an injection directly into the joint, but then the dye can easily be seen leaking into a labral tear, making the diagnosis clearer.
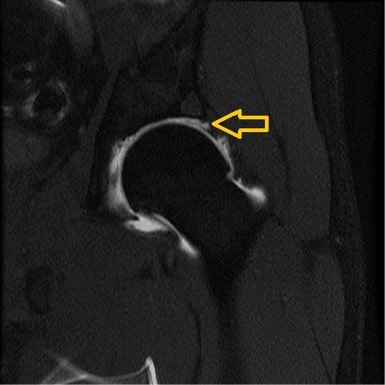
Figure 4: MRI arthrogram of a left hip labral tear. Arrow points to the dye leaking between the labrum and the articular cartilage.
I’ve been diagnosed with a labral tear. What do I do?
The mainstay of initial treatment for hip labral tears is physical therapy and activity modification. Physical therapy can help improve core/gluteal strength, which can shift the femoral head back in the socket a bit. This can decrease stress on the labral tear, which is normally near the front of the socket. While this doesn’t “cure” a labral tear, it can make some patients feel significantly better. Often times anti-inflammatories help our patients minimize their pain Sometimes, your doctor may suggest an intra-articular cortisone injection to the affected hip. While this also does not “cure” a labral tear, it can sometimes act as a physical therapy aid, allowing patients to “get over the hump” with initial therapy and start building core/gluteal strength.
When Should I Consider Having a Hip Arthroscopy?
Labral tears and hip FAI can now be addressed by hip arthroscopy, using cameras and small instruments inside the hip. “Scoping the hip” means looking inside the joint; there are multiple possible procedures that could potentially be performed during hip arthroscopy. In the past, the most common procedure was labral debridement, or trimming out the torn labrum.
While this has the advantage of not relying on the body to heal a labral repair, several studies have shown that labral repair has better long term outcomes than debridement. At least in my practice, labral repair is much more common. The labrum is repaired by drilling anchors into the bone of the socket, and using its sutures (thread) to wrap around and through the labrum to tie the labrum back into place. When doing a labral repair, any FAI should be addressed at the same time. Otherwise, there is a good chance of the repair failing (because the forces that tore the labrum would be the same forces causing it not to heal). Sometimes, a surgeon may tell a patient that the best procedure is an open surgical dislocation (through a large incision). There are some special cases where this approach may be preferable, but it is not common.

Figure 5: Large anterior labral tear. Note the separation between the labrum and the acetabulum. Compare this to Figure 1.

Figure 6: Picture of a labral repair. In the picture, there are three sutures that are anchored to the bone, sewing the labrum back to the acetabulum.
A newer procedure to address labral tears is labral reconstruction. This uses a tendon graft to take the place of the torn labrum. Typically, this is only used for hip labral tears that are so degenerative, that repairing the labrum will not work to restore normal labral function.
Hip arthroscopy is a passion of mine. I hope this has been helpful to you. If you have been diagnosed with a labral tear, please ask your surgeon specific questions. Over the years, I have seen many second opinions from patients who had less than successful outcomes from hip arthroscopy that thought they had a labral repair, but the surgeon actually did a labral debridement. To me, “fixing a tear” means sewing it back and anchoring the labrum; however, “fixing a tear” to some could also mean “fixing the problem caused by the tear”, which could mean debridement.
Derek Ochiai, MD











I’m a 57 year old women , with a physical job, I’m a city letter carrier. I’ve just been diagnosed with a hip impingement, bone spurs, labrum tear in my right hip. I had a 3t MRI that shows I need surgery. I’ve had 3 cortisone hip injections, that seem to help. My question is how little g can I keep getting injections until I have to have surgery?
Hi to everyone, I’m a 57 year old women. I work for the PO for 20 years. I’m a letter carrier. I’ve been diagnosed , with labrum tears. hip impingement , bone spurs. And tilted pelvis bone . Very healthy otherwise. I’ve had 3 cortisone shots to my hip. And wonder how long can I put off surgery that has been recommended . And why can’t I just keep getting shots?
Cortisone injections are not curative for your hip condition, but if they are used judiciously and sparingly, this is OK.
I’m a 57 year old women. I’ve been diagnosed with Hip impingement , bone spurs, labrum tears , and my pelvis has to be saved down. I’ve been getting cortisone shots, and working PT. But my doctor suggested after having a 3T MRI scan that I should have surgery. I’m afraid, and the cortisone seems to be helping. How long can I go before I need surgery?
In general, experienced hip surgeons avoid labral surgery in hips showing signs of degenerative osteoarthritis (bone spurs, etc). Perhaps seek a second opinion if you have any lingering doubts about the best course of action.
Hip Arthroscopy hip preservation surgery can be a good option, IF there is little to no hip arthritis. I would recommend a second opinion, so that you are clear on what the options are for your hip. Certainly, if non-operative treatment is working well for you, then this is an option to continue.
Hi Dr Luks,
I previously had a labral debridement surgery in 2009, and i have been complaining of pain since a few months after the surgery. I’ve had another MRI arthrogram which shows possible tears. One of the surgeons I met with is talking about the possibility of having to repair the labrum by stitching in cadaver tissue to the area where the previous debridement took place. Have you or are you aware of being able to use an autograft to reconstruct the cartilage at this time?
Thanks for your time.
There are many good hip arthroscopists who will reconstruct a degenerative labral tear. THe author of this article is one of them. I do not personally perform them… but I imagine that there are autograft alternatives.
Mr. Andrews,
Labral reconstruction can be used doing both allograft or autograft. If a longer graft is required, sometimes allograft is preferable to get proper length. I have done labral reconstructions using both.
My 17yr old son has tearing that involves mid to anterior aspect of the superior Labrum that continues 2.1 cm into the anterosuperior aspect of labrum, also abnormal prominence of fermoral head/neck, alpha angle 70 degrees that may be cam type impingment.
The specialist is booked out 3 more weeks. He is a senior and plays football and basketball. Can you explain this in worried mom terms, should i restrict all activity? Will he be able to play college basketball?
Please help me.