Hip pain is becoming more common with each passing week. Similar to other injuries we see, people are more active and stay active longer. It has only been 5-10 years since we have started to identify a common cause of hip pain — Tears of the labrum in the hip. In addition, we have identified anatomical reasons why you might have developed a labrum tear in your hip. Unless though issues are dealt with, an isolated labral repair may not work.
This is a guest blog post by Derek Ochiai, MD. He is a Sports Medicine trained Orthopedic Surgeon with a particular interest focus on the hip.
Nowadays, it is rather commonplace to read about an athlete undergoing hip arthroscopy for a labral tear of the hip.
This hip pain post will review:
- what is a hip labrum?
- why is the hip labrum important,
- how the hip labrum tears
- what kind of treatment is available for hip pain due to labrum tears
What is a labrum?
The labrum is a rim of cartilage that surrounds the hip joint. It attaches to the socket of the acetabulum. If you have friends who had a knee arthroscopy for “torn cartilage”, they had a meniscal tear of the knee. The meniscus of the knee and the hip labrum are made up of the exact same type of cartilage.
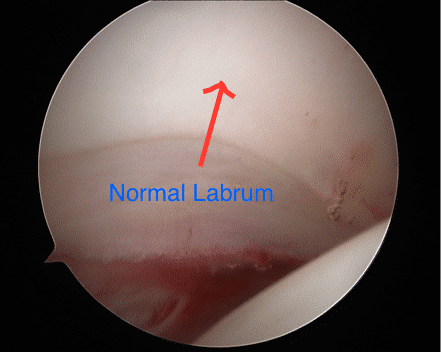
Figure 1: Arthroscopic picture of a normal posterior labrum. The labrum attaches smoothly to the acetabular articular cartilage. The femoral head is on the bottom right of the picture.
Why is the hip labrum important?
The labrum increases the relative depth of the socket, which can confer additional stability to the hip. This can be especially important in ballet dancers, figure skaters, gymnasts, and other athletes who put their hips through extreme ranges of motion. In developmental dysplasia of the hip (DDH), the socket is much shallower than normal, and the labrum deepens the socket to keep the femoral head of the hip in that shallow socket. Also, there are medical conditions where a person has increased joint laxity (such as Ehlers-Danlos), where the hip is more unstable and relies on the labrum for stability.
The labrum acts a seal around the femoral head, to maintain fluid pressure of the hip joint.
What are the symptoms of a labral tear in the hip?
The severity of symptoms can vary. The “hip pain” 90% of the time is perceived as deep in the groin. Sometimes, the pain can radiate to the side or the back of the hip as well. Many times, patients with a labral tear have pain and/or a feeling of catching in their hip, especially when going from sitting to standing. They may notice that they have to compensate to get in and out of cars. They may have pain with squatting and exercise, especially with sports that involve cutting and changing direction. Many times, patients also complain of pain with sex.
I didn’t injure my hip. Why do I have a labral tear?
The vast majority of labral tears are from FemoroAcetabular Impingement (FAI). FAI is a condition that develops in a person’s early teen years, where the hip is “out of round”. Since the hip joint and labrum are meant to function with round on round mechanics, this out of round conflict puts increased stress on the labrum. Over time, this increased stress can cause the labrum to tear. Symptoms of FAI greatly overlap with labral tears. In addition, symptomatic FAI can cause pain with prolonged sitting.
How is a labral tear of the hip diagnosed?
A medical professional can suspect a labral tear based on a patient’s symptoms and history. Clinically, the doctor can do provocative tests, such as the anterior and posterior impingement test, the McCarthy test, and the FABER exam, to further investigate. Many times, X-rays are very useful. FAI is a radiographic diagnosis, and usually can be easily seen on plain X-rays. With severe FAI, a labral tear can be inferred.
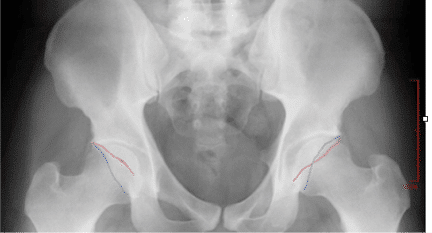
Figure 2: On left side of screen, normal acetabulum. The anterior wall (red line) and posterior wall (blue line) do not cross. On right, there is pincer type FAI, where the red and blue lines cross.
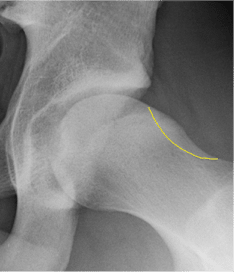
Figure 3: Typical cam type FAI X-ray finding. The yellow outline shows what the contour of a normal hip would look like.
MRI (magnetic resonance imaging) directly shows the cartilage of the hip. While a labral tear can be diagnosed with a plain MRI, an MRI arthrogram is more sensitive to labral tears. An MRI arthrogram does involve an injection directly into the joint, but then the dye can easily be seen leaking into a labral tear, making the diagnosis clearer.
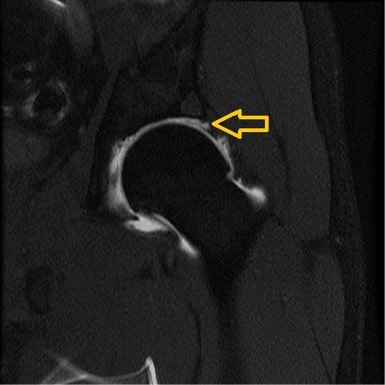
Figure 4: MRI arthrogram of a left hip labral tear. Arrow points to the dye leaking between the labrum and the articular cartilage.
I’ve been diagnosed with a labral tear. What do I do?
The mainstay of initial treatment for hip labral tears is physical therapy and activity modification. Physical therapy can help improve core/gluteal strength, which can shift the femoral head back in the socket a bit. This can decrease stress on the labral tear, which is normally near the front of the socket. While this doesn’t “cure” a labral tear, it can make some patients feel significantly better. Often times anti-inflammatories help our patients minimize their pain Sometimes, your doctor may suggest an intra-articular cortisone injection to the affected hip. While this also does not “cure” a labral tear, it can sometimes act as a physical therapy aid, allowing patients to “get over the hump” with initial therapy and start building core/gluteal strength.
When Should I Consider Having a Hip Arthroscopy?
Labral tears and hip FAI can now be addressed by hip arthroscopy, using cameras and small instruments inside the hip. “Scoping the hip” means looking inside the joint; there are multiple possible procedures that could potentially be performed during hip arthroscopy. In the past, the most common procedure was labral debridement, or trimming out the torn labrum.
While this has the advantage of not relying on the body to heal a labral repair, several studies have shown that labral repair has better long term outcomes than debridement. At least in my practice, labral repair is much more common. The labrum is repaired by drilling anchors into the bone of the socket, and using its sutures (thread) to wrap around and through the labrum to tie the labrum back into place. When doing a labral repair, any FAI should be addressed at the same time. Otherwise, there is a good chance of the repair failing (because the forces that tore the labrum would be the same forces causing it not to heal). Sometimes, a surgeon may tell a patient that the best procedure is an open surgical dislocation (through a large incision). There are some special cases where this approach may be preferable, but it is not common.

Figure 5: Large anterior labral tear. Note the separation between the labrum and the acetabulum. Compare this to Figure 1.

Figure 6: Picture of a labral repair. In the picture, there are three sutures that are anchored to the bone, sewing the labrum back to the acetabulum.
A newer procedure to address labral tears is labral reconstruction. This uses a tendon graft to take the place of the torn labrum. Typically, this is only used for hip labral tears that are so degenerative, that repairing the labrum will not work to restore normal labral function.
Hip arthroscopy is a passion of mine. I hope this has been helpful to you. If you have been diagnosed with a labral tear, please ask your surgeon specific questions. Over the years, I have seen many second opinions from patients who had less than successful outcomes from hip arthroscopy that thought they had a labral repair, but the surgeon actually did a labral debridement. To me, “fixing a tear” means sewing it back and anchoring the labrum; however, “fixing a tear” to some could also mean “fixing the problem caused by the tear”, which could mean debridement.
Derek Ochiai, MD








Help needed! I’ve been to two orthopedic surgeons for opinions. Last June while running, I experienced excruciating pain in left groin area. I was out of commission for 3 months icing, resting, etc. I had X-ray and regular MRI. Neither showed hip labral tear (one doctor said due to scar tissue?), but both doctors believe there is a tear. I’ve tried physical therapy for 6 weeks when pain flared/got worse in groin area and outer hip. Just got first cortisone shot 3 days ago. Any other suggestions? I’m a runner; last orthopedic surgeon said I may need to give that up entirely. Help!
There are many other reasons why a runner might have groin pain besides a labral tear — many large cities have Ortho surgeons who specialize in sports related hip injuries. Very few Orthos are good at hip arthroscopy. I would seek out an expert opinion near you.
Are MRI arthrograms painful? I’m also wondering if a second regular MRI (it’s been 6 months since last one) might be warranted since I’m experiencing new pains near outer hip now. Thoughts? Thank you so very much!
Good Morning Dr. Luks,
I’m reaching out to you regarding my 15 year old son. In July of 2015 he sustained a right hip injury playing soccer. He and another player went in to strike the ball at the exact same time, thus coming to an abrupt halt, and Tyler being the smaller one was on the losing end and felt a “pop”. He muddled through for the next few weeks with only mild pain, worked on stretching, icing etc. Ultimately he had a 3T MRI in late September. The orthopedic surgeon at that time ordered a “3T MRI to get the best possible images of the labrum without contrast” because he “didn’t want to inject the hip of an adolescent with an open growth plate”. The 3T MRI was read as normal but MD stated he could see that Tyler was growing rapidly and that was the likely cause of his pain and released him for soccer, told to work through the pain, which he did and was fine. Fast forward to October 29th, 2016, identical scenario however this time after a grueling high school season where he definitely had some overuse issues and more rapid growth. This time the physician thought Tyler had a “sports hernia” , went to PT , also had acupuncture & dry needling which helped with tightness but his anterior groin pain persists. His growth plates are still open but this time the MD ordered arthrogram with steroids. I am being told steroids could affect his growth and he himself eluded to that 16 months ago. I am very confused and concerned so requested we proceed with the least invasive option first. 3T MRI was done last week and is normal. Am trying to decide how to proceed as well as look for a second opinion. Considering asking for ultrasound to evaluate for hernia. Please give me your thoughts. As a pediatric surgical services nurse, I understand there are no guarantees and each medical professional can have different viewpoints etc., however I feel as though I must proceed cautiously and gather as much information as possible to make a more informed decision for my son. Thank you for your time, it is so very appreciated
HI Ramona …
There are so many causes of hip pain in a 15 year old. Labral tears are actually very rare in this age group. Sports hernia are 1. very very rare in this age group and 2. have been coming under fire recently as a diagnosis of exclusion and the possibility that it isn’t even a true diagnostic entity. An US will not show a “sports hernia”.
The injury you describe in a child your son’s age will usually cause an AIIS (rectus femoris) pelvic injury. It is a fairly benign injury in most. Hip pointers and chronic growth plate (pelvis) injuries are more common than labral tears.
The only way to arrive at a good diagnosis is a great physical exam. I would start with a second and perhaps third opinion. Steroid injections into the joint will not affect his growth but should be avoided if possible.
Good luck… there are plenty of sports docs who specialize in hip injuries — hopefully you have one near you.
My daughter was just diagnosed with Hip Dysplasia and bilateral labral tears. Our specialist skipped over the tears and went straight to recommending a PAO. My daughter is a sophomore in high school and a very active dancer. She is not ready to give it up. In your opinion would labral tear repair help extend her ability to dance for another year? We would like to hold off on the PAO for a year or 2.
Sorry Jeannine … It’s impossible for me to tell you what the next steps should be.
Dr. Luks, Thank you so much for your detailed response, so generous with your time and expertise. I’m finding that it may he necessary to go outside of Louisville to seek a second opinion but am unsure how to go about finding a doctor who specializes in hip/sports injury /adolescents.
Thank you again for your time!
Ramona
Dr. Luks I am a very healthy active 62 year old female. I have just been diagnosed with a labral tear (out patient arthroscopic/MRI). I have had it for 3.5 years and PT was not successful. A preliminary opinion (over the phone from a orthopedic surgeon) is because of my age I need a full hip replacement. I do not understand why they will not recommend a labral tear repair by arthroscopy. Should I be looking for a very experienced doc (Worcester MA area) in hip arthroscopy before rushing into full hip replacement? BTW they did not mention any FAI but did mention the presence of minor arthritis. Thanks for your advice
Once there is arthritis, a labral repair is not usually indicated. Osteoarthritis can dramatically affect the results of labral surgery.
Thank you so much for all you have given us in terms of your knowledge on this forum. Sept 2016 I fell down 2 stairs landed on my left knee then ended up on my left hip. I have had a lot of pain on the outside of my hip. It hurts a lot when I’m sleeping at night also. I just had an MRI done and it shows a partially detached left Superior labrum. The bones are well aligned with normal marrow signal. There is no evidence of hip fracture or joint effusions. There is no evidence of avascular necrosis. Both hip joints are mildly to moderately narrowed but symmetrical in appearance. However, the left labrum appears partially detached superiorly and is best seen on coronal thin section image 10 of Series 7. It potentially could be caught between the femoral head and the acetabulum at times. IMPRESSION: no evidence of acute bone bruise fracture a fusion or avascular necrosis. Mild to moderate symmetric osteoarthritis of the hip period partially detached left Superior labrum. I will be 65 in May have been physically active at work unloading boxes standing on my feet and also sitting. I question, as you stated in the above Forum, that surgery may not help the tear because of my age and osteoarthritis?. Would Physical Therapy be an option or will it just aggravate the situation? I have not gone to see a surgeon yet just researching the internet and thankfully I came across your awesome site. Any feedback would be gratefully appreciated. Also, would a pemf mat be useful in this case? (Ex: Bemer mat or IMRS mat) I do plan on finding a capable doctor here in Florida but I wanted your expert opinion also. Thank you so so much for this forum!
It is unlikely given the arthritis that the labral tear is the source of your pain. If the pain is on the outside of the hip you should talk to your docs about evaluation for bursitis or gluteus medius strain. Depending on what they feel is the underlying cause, then PT is often very useful.