
Meniscus tears are very common. Each knee has two menisci which serve as cushions. They can tear due to degeneration, or they can tear due to trauma or a sports injury. The treatment of a meniscus tear will depend on the type of tear you have, whether or not you also have osteoarthritis and the nature of your complaints.
Many people do not understand why many meniscus tears do not require surgery. Having a firm understanding of what the meniscus does and why some tears do not require surgery should go a long way in assisting you in your surgical decision-making.
Meniscus tears are a very common source of pain in the knee. They are also commonly seen on MRIs obtained for other reasons – and are not necessarily the cause of your pain. Many people come in on a daily basis and ask if surgery for their meniscus tear is always necessary. In this post, we will explore
- what a meniscus is,
- what are meniscus tears,
- why meniscus tears are so common
Meniscus Tears
What is a meniscus? It is a cartilage disk that’s found in the knee.

There are actually two of them. We have one on the inner side of the knee which we call the medial meniscus and one on the outer side of the knee which we call the lateral meniscus. These two disks function as shock absorbers or cushions to minimize the stress on another type of cartilage that we have in the knee which we call the articular cartilage. The articular cartilage is the cartilage that actually coats the ends of the bones. If the two menisci are not present or they’re torn, then the articular cartilage sees an increase in stress and can trigger the onset of osteoarthritis. Meniscus tears are by no means the only cause of osteoarthritis. However, they certainly are a significant contributor.
Why do meniscus tears occur?
Now I see many patients every week who present with knee pain and many of them are suffering from meniscus tears. Why/How do we get meniscus tears? Why do these little meniscal disks tear so easily once we reach our fourth, fifth decades and beyond? Our meniscal tissue is non-regenerative. It’s similar to our brain or our heart tissues. If we have a heart attack or a stroke, we do not regenerate those areas of our heart or our brain. It simply scars in. Yet if we cut our skin, our skin heals. Our skin tissue is regenerative, same with some muscle and a lot of other tissues in our body.
The meniscus tissue in our knee has very few mechanisms for repairing itself. Therefore, every step that you’ve taken, every twist that you’ve done, every time you’ve knelt down or squatted down, you’ve put a force across that meniscus and eventually it wears out and the meniscus tears. (This is why most tears are referred to as being “degenerative”. A lot of times people will note that they simply knelt down to pick up something up and when they went to stand up they felt something rip inside their knee and noted the onset of pain.
Why does a meniscus tear hurt?
The typical patient with a meniscus tear doesn’t have much in the way of pain with walking straight ahead. Sometimes they do. It depends on the size of the tear but usually, they’ll tolerate walking in a single direction very well. Patients with meniscus tears will occasionally complain of pain going downstairs. They’ll have pain getting up from a seated position. They’ll have pain with turning, pivoting and twisting and some patients, if the meniscus tear is large will complain that the knee is buckling or giving way or feels unstable. Many of you will also find you need to sleep with a pillow between your legs at night.
A meniscus tear hurts because they sometimes irritate the lining of the knee joint called the synovium. Tears can also hurt if there is a loose piece which is getting caught in the joint.
Types of meniscus tears?
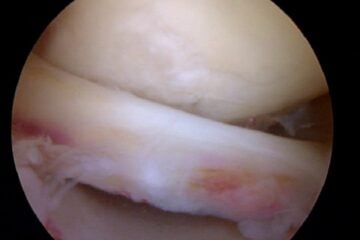
What are the different types of meniscal tears? The majority of tears are degenerative meniscal tears. When you look at the cartilage disc, the edges are simply frayed. The tissue has been destroyed from years and years of use. Nothing you did wrong. The tissue simply wore out. It’s like the front of a pair of blue jeans that you’ve worn for decades and the material just simply wore out.

Then there are those who have suffered more acute meniscus tears and these tears can have different shapes and different patterns. The shape and pattern will determine how symptomatic or how bothersome the meniscus tear will be. If a loose flap of tissue is created and that flap is moving around within the knee – that’s when you’re going to have given way and you’re going to have pain with many activities. You’re not going to tolerate flap tears well and those patients with flap tears (or unstable tears) will usually (not always) go on to require an arthroscopy or a scope to try to either repair or remove that torn piece.
We Treat Patients, NOT MRI findings…
Many patients with meniscus tear pain will improve within a few weeks of onset… in many cases, there is no need to rush into surgery.
- If your pain is starting to improve and
- if the pain does not interfere with your quality of life
- If compression sleeves work to control the pain
- If your range of motion is well maintained and
- You can participate in your normal daily activities —
Then why would one consider meniscus surgery a necessity? Not all “tears” require surgery. Again, we as physicians need to treat the patient, and not the disease.
Consider this article which demonstrated that a sham surgery (incisions made, but nothing done) was no better than treating a meniscus tear when the patient had a degenerative meniscus tear. There are also plenty of studies which show that a degenerative tear can be treated with physical therapy.
How are meniscus tears treated?
If you have knee pain, and you’re found to have a degenerative meniscus tear — I typically advise patients to simply just wait. A lot of times your symptoms will go away. If you sustain an injury and you have an unstable tear, a tear we call a horizontal cleavage tear, a radial tear or a flap tear — those are the tears tend to remain bothersome. If after four, five, six weeks, you still have the same degree of discomfort and quality of life issues, then you might be a good candidate for surgery, which we call an arthroscopy.
Physical therapy can help those of you whose knees feel unstable or weak, and it can help those of you with significant swelling to gain back your motion, stability and strength. Therapy can be beneficial before surgery (pre-habilitation), instead of surgery, or after surgery.
Many patients feel that a compression sleeve makes them feel better and improves their sense of stability – see some of our patients’ favorite knee compression sleeves here.
Do all meniscus tears require an arthroscopy?
What exactly is an arthroscopy?
Basically, an arthroscopy involves bringing you into the operating room, inducing a light sleep, injecting local anesthesia and then placing a fiber-optic camera into your knee through a ¼ inch incision. We then inspect the entire joint, find the tear and determine if it will be removed or stitched back into place. Most procedures take 15-45 minutes and you are able to go home the same day. Whether or not you can return to sports soon will depend on which procedure you had — repair versus removal. More on the recovery from meniscus surgery here.
Do you have questions regarding an Orthopedic injury or longevity?
Do you want to talk to an expert who can listen to you for 45-60 minutes and explain the options in detail?
Dr. Howard Luks offers remote guidance sessions to review your X-ray or MRI images and explain your options.
Dr. Luks has also received hundreds of requests for educational sessions on the topics discussed in his book, Longevity Simplified.
So if you have a meniscus tear, it’s not all doom and gloom. Many tears do not require meniscus surgery. Some of them do. Some meniscus tears are repairable. Sometimes the torn portion of the meniscus is simply removed.

We try to repair – or suture- meniscus tears whenever possible — but only certain tears are in fact repairable. One caveat: If you have a meniscal tear and you’re experiencing instability or giving way, be very careful with your activities. You don’t want to find yourself on the stairway carrying a load of objects and your knee gives way. If you have instability symptoms, make sure that you have a hand available to hold onto something at all times while you are in your recuperative phase or awaiting surgery or simply waiting to see if the symptoms are going to recover on their own.
Hope you enjoyed this post. For more information there is a more in depth section on meniscus tears here.
And by no means is meniscus surgery or emergency surgery. Take your time, rest and consider a second opinion.
After your meniscus surgery, what should you expect as your recovery from an arthroscopy for a meniscus tear?
Due to the overwhelming popularity of this post, I want to make sure that the many and varied needs that each of you have is met during your visit here. With that in mind, you may benefit in reviewing these related posts on this site:







Mladen
Dear Dr. Luks,
last August I injured my right knee when playing football. On 30th August, 2013 I had a surgery – ACL reconstruction and repairs on both menisci. There were two tears in each meniscus. After the surgery I was on crutches for 30 days with no weight bearing on the “repaired” leg. Since than I have been doing rehab and working out for muscle strength. Gradually I started running and got to running 4 km without any pain in the knee :)
I also started doing some plyometric exercises – like box jumps with both legs. At 8,5 months after surgery I decided to start one leg jumps. One they I did 3 sets of 10 reps jumps with each leg. Right after that I ran another 4 km. I was feeling well at the end of the work out – no pain at all.
However, on the next day my knee felt stiff and flexing was more difficult than before, although I was able to flex both legs almost equally. It’s been almost two weeks, I have been resting, the knee is not stiff any more and flexing is fine, however, sometimes I feel slight pain when walking. I am worried that I did something to the repaired menisci with these one leg jumps… :( Is this possible or its just that this exercise introduced a completely new type of stress to the knee (after almost 9 months) and the muscles around the knee need some time to recover and get used to it?
Next week I will see my orthopedist to discuss this issue with him, but I have been really down and worried that I have injured myself again. I would really appreciated Your opinion.
Thank You in advance!
Kind regards,
Mladen
It’s not unusual for a reconstructed knee to respond to a new activity like this. Hopefully your exam shows that all is well.
Good Luck
Howard Luks
Antoni
Hey,
I am a 24 year old male who is extremely fit. I have been playing soccer since I was 6 years old pretty much. I just wanted an opinion on my MRI report before I discuss this issue further with all the medical professionals. I have been working as a car detailer for the last 2-3 years pretty much full time and over these last few years I have had 2 injuries to my knee when I was off season from soccer where the inside of my right knee would hurt a lot from all the twisting I did on my knee getting in and out of cars over 200 times a day (it would only put me out of soccer and work for a week). Anyways towards the problem, 2 weeks ago I slipped over while playing indoor soccer and I heard a few pops in my knee. It swelled up over the next few hours and for about a week I struggled to get out of my bed with pain and swelling and limited movement of my knee. Its 2 weeks later now and my swelling has significantly improved and I am able to move my knee around a lot more without the pain.
I just picked my MRI report and this is what it said,
patella and supra-patellar recess
the articular cartilage appears within normal limits for the patients age. there is a moderate knee joint effusion. there is a small amount of fluid in the deep infrapatellar bursa
anterior cruciate ligament
there is increased signal intensity and irregular contour of the anterior cruciate ligament indicative of strain injury
Posterior cruciate ligament
there is normal signal intensity and contour of the posterior cruciate ligament
medial meniscus
there is evidence of increased horizontal signal extending to the inferior articular meniscal surface in the posterior horn and a vertical component in the anterior horn extending to the articular surfaces, involving the annular fibres
lateral meniscus
there is no evidence of increased signal extending to the articular meniscal surfaces indicative of a meniscal tear
medial collateral ligament
there is increased signal intensity adjacent to the medial collateral ligament in keeping with a grade 1 strain injury
lateral collateral ligament
there is normal signal intensity and contour of the lateral collateral ligament
medial compartment and lateral compartment
the articular cartilage appears within normal limits for the patients age
femur and lower leg bones
there is a focally increased T2W signal intensity of the bone marrow of medial femoral condyle and medial tibial plateau indicating bone oedema secondary to a medial compression injury
Comment:
there are features of a complex medial meniscal tear as described
And on a seperate X-ray they found that my hoffa’s fat pads had some soft tissue swelling.
Do you think surgery will be necessary?
HI Antoni..Hard to say if surgery is the answer. Last thing you want to do is loose part of your meniscus at your age. Many doctors recommend physical therapy, etc for a short while before determining if surgery is necessary. In addition, keep in mind that many surgeons, myself included might be able to repair (sew back together) horizontal tears as opposed to trying to remove the torn portion. Try to find a surgeon who is willing to give it a go if it is possible. The decision to repair vs remove is actually made during surgery .. but many products, like the Centrix repair device have made it easier to repair certain tears. Good Luck
Howard Luks
Anas
Dear Dr. Luks,
I am a 29 yrs old male, fit and have been playing soccer for many years.
I injured my right right knee after playing soccer recently, it was painful and swollen initially. It has been 10 days now since the injury and it is still swollen – though less swollen that before – and the pain has reduced, though I cannot squat my right leg fully, and pain will be stronger if I am to move my leg in certain ways – including sudden movements. I had an MRI scan which showed the following:
“Within the medial compartnment there is a large horizontal tear of the body and posterior horn of the medial meniscus extending to the inferior articular surface. The Chondral surfaces are preserved with no focal defects. The medial collateral ligament is intact. Mild bone oedema is present in the medial tibial plateau.
Within the lateral compartment the lateral meniscus is intact. The Chondral surfaces are intact with no defects. The posterlotaral corner structures are unremarkable.
Within the patellofe,oral compartment the chondral surfaces are preserved with no focal defects. The quadriceps and patellar tendons are intact.
The anterior and posterior cruciate ligaments are intact. A large join effusion is present. There are no intra articular loose bodies. There is no Baker’s cyst.”
I am scheduled to see the specialist – orthopedic surgeon – soon, but it seems I would need a surgery (orthoscopy) done… Do you think this is the case with certainty, based on the MRI findings?
Many thanks for the assistance and the response in advance.
Kind Regards
It’s possible Anas… but keep in mind. Many of us might repair a tear like that at your age. It might be hard to find someone to repair it as opposed to removing the torn piece. Do your research and seek a few opinions if necessary.
Dr. Elliot Sklar
Dear Dr. Luks,
I am a 33 year old male and injured my right knee while salsa dancing on New Year’s. I had no major pain – just felt like I had twisted something. I walked several blocks home from the party I was at and have improved vastly over the last 3 weeks using the RICE method with a reduction in swelling, increased mobility, I can walk slowly but normally and can do stairs. I saw a D.O. who examined me and did not feel it was more than a sprain or at worst a possible meniscal tear. I had left ACL and meniscus surgery 2 years ago this month, and saw my surgeon for my recent knee injury to ensure it was nothing beyond a sprain. He examined me and felt that no ligaments were torn but wanted to rule out a meniscal tear. I just got my MRI results which indicate peripheral vertical tears in the posterior one thing of the posterior horn on both the medial and lateral mesicii, a complete tear of the ACL torn in the mid substance and a grade 2 MCL sprain. This injury has been a completely different experience than when I previously tore my ACL and my surgeon did not detect any possible ligament tears during a physical exam. In your opinion, how should I proceed? Could this be a bad read on the MRI or could it be possible that despite my limited symptoms I have suffered this much damage which would clearly require surgery?
Thank you!!!
It could be an over-read.. or it could also be a poor physical exam. Maybe your knee was swollen and difficult to examine ??? Tearing an ACL graft doesn’t usually produce the same symptoms as tearing your native ACL. There are no nerve fibers, and if an allograft was used, there is very little blood supply. So there tends to be less pain and less bleeding. With new peripheral tears, it is likely that your knee buckled… but I can’t say 100%. Did they mention a bone bruise on the end of the lateral femoral condyle or the posterior lateral tibial plateau? That would confirm that your knee gave way.
Good Luck.. time for another exam.
Howard Luks
Elliot Sklar
Dear Dr. Luks,
A million thanks! Yes, my knee was swollen at the time of exam, but the exams were involved both times (testing range of motion, ability to bend, squat, bear weight, etc.) This injury occurred to my right knee – not the one previously operated upon – so this is my native ACL. The injury experience was entirely different than when I tore my ACL previously – no major pain at all, and I was able to walk home. Last time I could not get up off of the ground. The MRI report does state:
“Complete tear of the ACL. Grade 2 MCL complex sprain. There is edema in the popliteus muscle belly and muscle-tendon junction as well. Bone marrow contusions are seen in the posterior medial and lateral proximal tibia as well as the mid lateral femoral condyle extending anteriorly. Intact extensor mechanism.”
With that said… I don’t feel instability in the knee as I did with my left knee when I tore it – so something isn’t adding up for me.
Thank you!!!
Elliot… those bone bruises unfortunately give it away. They imply that the knee buckled when your ACL tore. The edema in the posterolateral corner goes along with that theory as well. Having seen many many patients with ACL tears, so are more traumatic, thus more painful — some tear with less force, cause less bleeding and inflammation and tend not to bother people as much. Good news on the lack of instability feeling!
Good Luck
Howard Luks
Aloke Saha
Good Day Doctor Luks
I am Aloke from Malaysia. I was doing some study about lateral meniscus tear and stemcell therapy, and thus found you on the web.
I had a football injury and was found to have lateral meniscus tear in MRI. Then I had gone through arthroscopy surgery in January 2010.
But now for last 1 year I have got a pain full knee specially while climbing stairs and running. In the recent MRI it was found that there is “Horizontal tear of body of lateral meniscus with adjacent parameniscal cyst”.
I have been consulting a Dr Saw Khay Yong in Kuala Lumpur and he advised me to go through another arthroscopy and stem cell therapy (culturing from Bone marrow).
The surgery is due next month.
I am bit afraid to go through another surgery, because i come to know from some study on internet that this will create some more hole/void in my knee with a possibility of arthritis in future.
Can stem cell therapy resolve my issue? any other alternative we can adopt?
I Request your kind advise on this issue.
** I have sent you a request in Twistle. I can send you my MRI images if you advise.
Best Regards
Aloke Kumar Saha
Locked Bag No. 1, 98009, Lutong, Miri, Sarawak, Malaysia
HP: +60 11 158 63 081
Softphone: +60 85 45 4568
Email: [email protected]
Good Morning Aloke…
Sorry.. I use Twistle for patient communication only.
You should talk to your surgeon about the possibility of trying the stem cells before considering surgery. You could also ask if he would consider a repair (many of us will try to repair certain horizontal cleavage tears), expecially since the stem cells “should” increase the chance of healing. The most recent study on stem cells and mensicus tears shows that the meniscus can partially grow back — that’s a very interesting area of study.
SAURABH
Hello Doctor,
Yes he did removed a portion of damaged meniscus at that time when I undergone ACL reconstruction surgery, but he is saying still it need to be operated as that damaged portion can hurt joints in future resulting in arthritis problems. So kindly suggest on this, he will be removing damaged portion of meniscus. Should I go ahead on this?
SAURABH
Hello Doctor,
I had ACL tear surgery in April,2012 . Now again last month I got knee twisted and doctor advised me to go for MRI.
MRI report shows
1.Meniscal tissue in the region of the intercondylar eminence- possible bucket handle tear with significantly attenuated meniscal tissue in the body of the medial meniscus. Mildly attenuated anterior horn of the medial meniscus.
The Surgeon who operated me earlier advised me to undergo arthroscopic for cleaning of the damaged portion, I have consulted another orthopedic, he suggested to try physiotherapy then come to a decision.
What should I do ?
Surgery or it can be cured by Physio and exercises?
Check with your initial surgeon … he may removed a portion of your meniscus during your ACL surgery. If he did… then your second opinion sounds like a good option. If your first surgery did not involve the meniscus — you will likely find that bucket handle tears tend to remain bothersome and can damage the inside of your joint. Therefore many of us prefer to operate on bucket handle tears sooner rather than later.
SAURABH
Thanks Dr. for your reply. I will concern him but isn’t it risky to for surgery a second time ? Will this surgery be as big as ACL Repair one which I had earlier? Surgeon told me like this will be a minor one and I can walk from next day?
Sarvesh
Dear dr,
MRI report of one if my relative is suggesting below findings, Pls suggest the treatment option available for same and is it necessary to go for surgeries:
Finding:
Findings are suggestive of anterior cruciate
ligament tear with mild joint effusion and complex tear of lateral meniscus
Depends on what your relative is feeling, experiencing and what their exam is like… I do not treat isolated MRI findings… I treat patients :-) And each patient will respond differently.
Prof. Dr. S. Balaji
Hello Doctor, This is Prof. Dr. S. Balaji, (chemistry by profession) from India. It is nice to see your untiring response for the world community. I seek your valuable advice for my son’s case. My son aged 13 fell down 4 months back (inside the home due to floor slip) and his right side of right knee touched the floor (twisted movement). He has pain in walking and we thought sprain and after applying some pain relieving gels the pain subsided and after a week we noticed that he has click sound when doing squatting. He managed as the pain was not continually persistent. Then we consulted with a physician who advised some physiotherapy. After physiotherapy for a week he felt lesser pain and wearing a knee cap as recommended. Since it is now 4 months we consulted an orthopedic and taken an MRI.
“MRI revealed Non-displaced oblique tear of the posterior horn of the medial meniscus”.
The doctor advises partial menicsectomy. The right now problems are: (1) clicking sound during deep squatting followed by pain for 3 minutes and then pain disappears (no clicking sound on non-deep squatting and no pain), (2) mild pain during stepping up the staircase, (3) Small swelling but no pain on touching or pressing (right knee front left side). He is walking as usual and even running some steps causes no pain. I need your valuable advice on the following issues.
1. Is surgery is unavoidable.
2. Can it heal on its own, if so how long would it take.
3. Can i postpone the surgery if how long.
4. If i avoid the surgery and manage by nonoperative procedures will it cause him any issues (from your review studies).
5. His school is near by home and there is no need to change the life style pattern, so if curing by rest (after schooling hours) is possible then we can postpone or avoid surgery.
After reading most of your replies, i went for a second opinion and the doctor said partial meniscetomy. I talked about the pros and cons (as learned from your replies), they said you need to find the balance between the two.
Looking forward your reply and advice.
Professor,
Most of us (sports medicine surgeons) would try to repair the meniscus (by suturing it together) before ever contemplating removing a portion of the meniscus in a 13 year old. 13 year olds have remarkable healing capabilities. It would be worth an attempted repair (in my opinion), with the clear understanding that it may not heal and a repeat arthroscopy may be needed in the future. Removing a piece of your son’s meniscus at this age would set him up for many problems down the road as a young adult.
If the tear was going to heal, I imagine it would have done so already. Meniscus tears in children are looked at differently than those in adults. Children tend to have traumatic tears, and these tend to heal nicely. Whereas adults tend to have degenerative tears which do not heal well… and often respond to non-surgical measures.
Good Luck to you and your son.
howard luks
Name sean
Dr Luks , I’m 54 , I’ve been playing tennis for a number of years , anyway last year I swelled up one of my knees playing , got the MRI : in the medial compartment , there is complex abnormal signal intensity noted at the level of the meniscus. Specifically , there is a horizontal oblique component extending to a vertical component closer to a free margin of the meniscus . There is additional extension of the more horizontal oblique component to the undersurface of the meniscus . The medial collateral ligament is intact although thickened with faint increased signal intensity tracking along the ligament . The articular
Cartilage overlying the medial femoral condyle and tibial plateau are grossly within normal limits .
In the lateral compartment , there is visualization of a bow – tie type configuration to the meniscus on
Four contiguous Sagittal images , consistent with a borderline lateral meniscal discoid variant . The lateral collateral ligament is within normal limits . The articular cartilage overlying the lateral femoral condyle and tibial plateau is minimally thinned , with small osteophyte formation noted .
Both the ACL and PCL are within normal limits .
There is loss of the normal trilaminar appearance to the patellar cartilage with thinning medially .
There is increased T2 signal intensity noted subchondrally at the level of the medial patellar facet .
The extensor mechanism , patellar tendon as well as the medial and lateral patellar retinacula are grossly within normal limits .
There is no significant joint effusion . A trace amount of fluid is noted in the bursa between the medial head of the gastrocnemius and semimembranosus tendons .
I would like your opinion on wether to get repaired , the way I see if I want to continue to play tennis , I don’t have a lot of choice , your thoughts please and thank you .
Sean … After allowing a few weeks to see if the pain settles down and allows you to return to sports .. it becomes a quality of life decision as to whether or not surgery is in your best interest. Some tears simmer down and will not bother you.. some will not simmer down and would benefit from an arthroscopy.
good luck
Howard Luks
Name william winter
I’VE BEEN TOLD I HAVE BILATERALL PATELLA TENDONITIS,I CANT WALK UP OR DOWN STAIRS,CANT STAND UP AFTER BENDING DOWN WITHOUT HAVING SOMETHING TO HELP GET UP,AND FOR NO REASON AT ALL, EITHER KNEE WILL GET A SHARP PAIN FROM OUT OF NO WHERE AND SEND ME TO THE GROUND.I CANT DO ANY CRAWLING AT ALL.I AM A BOILERMAKER AND WORK IN BOILERS INSIDE POWER PLANTS AND HAVE BEEN OUT OF WORK 3 YEARS BECAUSE OF THIS.MY SPORTS DOC. SAYS HE HAS TRIED EVERYTHING UNDER THE SUN WITH NO LUCK,EVEN TRIED PLATLET RICH INJECTIONS 3 TIMES,NOW NO INSURANCE AND OUT OF MONEY BECAUSE INS. DONT COVER P.R.I. DO YOU ANY THOUGHTS ON THIS CONDITION I HAVE?THANKS
If your pain is truly due to patella tendonitis, and PRP injections have failed, there are surgical alternatives, with a great track record which could be performed to try and get you back up on your feet!
Good Luck to you!
Howard Luks
Reshma
Hey Dr.luks,
i m from india,As i got meniscus tear in age of 22.from past two months healing is not complete and i use to get sudden jerks/attacks while walking.I am able to fold my legs but pain didnt went.
I got fear whenever i walk ,i dont know why this suddenly started,can you please tell me what i should do to get relief from this sudden pain in knee?
You may wish to speak with an orthopedic surgeon to explore your options.
Good Luck
Howard Luks
Rescue
Dr. Luks, thanks so much for having a site like this with great information and providing personal responses.
i got meniscus tear two months ago,now i m able to fold my knee by doing hamstring exercise,but while walking i m getting sometimes jerks and sudden pain in nerve.
can you please tell me what will be the problem??whether it is serious problem or healing is not complete..what i should do now??
suggest your advice…..thanx alot
You have a quality of life decision to make. If you have tried rest, activity modification, and physio and your pain persists then you might want to explore surgical options with your Orthopedist. Make sure you discuss repair vs removal.
Good Luck
Howard Luks
Rescue
thanks for fast reply…..:)
i hv tried rest for a week only as i m working.
but the condition is improving,i want to know how much time healing takes as per your opinion.even i hv shown to orthapedic in starting he told to do all activities and he told not much serious.
does it requires surgery?
Name Judy
Dr. Luks: I fell recently on cement, hitting my knee hard. i had fallen 5 years ago, same knee injured. I had arthroscopy at that time. My MRI this time indicates I have a horizontal free edge tear of mid body of medial meniscus, with a minimal parameniscal cyst formation. There is also a horizontal free edge tear of the mid body and anterior horn of the lateral meniscus. There is also grade III-IV chondromalacia of the weight bearing surface of the lateral femoral condyle. My Ortho MD gave me an injection today to try and reduce the pain. He indicated that because of the arthritis I may be facing a total knee replacement in the near future. Do you think I should have the arthroscopy and then just try to deal with the arthritis with periodic in jections?
The pain in my knee radiates down the front of my leg and keeps me awake at night. I am 61 and planning to retire in 4 months.
Be very wary of treating arthritic knees with an arthroscopy. The current literature shows that physical therapy can be as effective as surgery in managing the pain associated with mensicus tears in the presence of osteoarthritis.
Good Luck
Patricia
Dear Dr. Luks,
Six weeks ago I started with severe knee pain and effusion with knee instability. The only previous history is I went to a triplex vacatiojn home for a wekend and I used the stairs quite a bit. The pain was better aftyer a week, not mobility though. Then a week later it came back with revenge all the pain, it lasted for 4-5 days and better again. It just a little instable but the pain hits me with just walking some times, when I go downstairs and when I get up from sitting position. I cannot kneel because of the pain. My knee feels tight and supino position does not help, it only relieves the pain ice and crossin my legs with the sore knee on top of the healthy one. I don’t like to take anti-inflammatory drugs unless the pain is unbearable. I just got the MRI results of:
1- Complex tearing of the posterior half of the emdial meniscus with reactive marrow edema in the medial tibial condyle. It says horizontal cleavage tearing of the mid third segment of the medial meniscus and partial thickness, inferior surface tearing of the posterior horn of the medial meniscus on sagital image. Coronal image shows partial-thickness inferior surface tear of the mid third segment of the lateral meniscus.
2- It also says partial thickness inferior surface tearing of the mid third segment of the lateral meniscus.
3- Mild chondromalacia of the medial patellar facet and mild cartilage thinning diffusely in the medial compartment?
What is your opinion about my best choice of treatrment? I am secretly expecting a : physical therapy. Knee brace makes my knee burn after a while. I don’t know hat is recommended or not while I wait for my long waiting list on my orthopedic doctor.
I would really appreciate your expert opinion. Thank you for the website.
Patricia… the “injury” you sustained is not enough to have caused the meniscus tear. You likely had it before the pain occurred. Reactive edema in bone under the meniscus is a common and very painful situation. The pain from the edema can go away in as little as 3-4 weeks. Many people live with meniscus tears for a long time without the need to “treat” it. A very astute surgeon can tell you whether or not the pain is from the meniscus or the edema or fluid in the bone. Time will tell… there’s certainly no rush as long as you symptoms are improving and your feeling of instability is no longer present. I might hold off on PT and use a cane to help the bone heal and allow the fluid to decrease. Then you can start therapy after a month or so…. but that’s not an actual treatment recommendation! It is something for you to research, consider and discuss with your doctor when you come up with a plan.
Good Luck
Howard Luks
Walt
Dr. Luks, thanks so much for having a site like this with great information and providing personal responses. If I end up needing surgery, I will definitely consider coming to you.
I am a veteran and had my knee evaluated by a Veteran hospital PMR doctor. The VA is not known for the best care, so I would love a second opinion. After moving my leg around, I was told it appears my meniscus was torn. I have not yet had an MRI and the doctor did not suggest one. He seemed to think it is minor and I can’t do much about it. He suggested I stop activities that aggravate it. I am a competitive mixed martial artist and instructor, and stopping forever is not really an option.
I am trying to decide if there is a reason for me to insist on an MRI or further evaluation. The inside of my knee is sometimes in minor pain and movement is not hindered. It just sort of feels like there is something wrong. There is a tightness if I bend my heel toward my butt, but it doesn’t hurt. It feels more like a tight knuckle that wants to get cracked. If I continue bending it, the knee pops and then feels fine. Sometimes it is a little sore the next day and I ice it etc. Is that popping a bad thing if it doesn’t hurt? The popping noise scares me.
How would you suggest I proceed? Just rest, insist on MRI, continue activity lightly, surgery or what? I haven’t stopped my training, but am taking it much easier than normal.
Thank you very much in advance. I look forward to your response.
Walt
Thanks Walt !!!!
This is exactly why I often say that we need to look at patients as individuals. The same pain affects each person differently. We all have different goals, activities, etc.
You’re correct.. the popping in your knee could be an issue.. such as a meniscus tear. Frequently a physical exam and Xray can give us a good idea about what the likely problem is, but an MRI may be needed to prove it. Why not start by asking to see the Orthopedist? If that’s not an option then you may want to take it out of the VA system ???
Good Luck ~!
HJL
Walt
Thanks for the speedy reply. My plan is to insist on being seen by ortho and having an MRI. I definitely need more answers than I was given last time. If there is something wrong, then I want to know exactly what is wrong. I at least need to speak with another doctor, as the last doctor basically told me to simply stop doing anything that hurts. I actually have a friend in ortho that also trains in martial arts. I will try to get in touch with him and see what he thinks. After that, I expect to follow up outside the VA System, so maybe I’ll be talking to you again soon.
Thanks Again,
Walt
Peter
Hello Dr. Luks,
I am writing this to get your opinion regarding my knee.
I had an ACL reconstruction surgery about 2 years ago and I have been playing basketball and lifting after 5 months of surgery.
Recently, when I was playing basketball, I heard a pop in my knee and I could not extend my knee.
The knee swell up slowly the day after.
Got my knee checked out by my orthopedic doctor and he advised me to take a MRI.
The MRI discovered “Complex Tear of the medial meniscal posterior horn and body. The medial meniscal tear demonstrates a posterior horn horizontal component, as well as a bucket handle tear component displaced into the lateral aspect of the medial compartment. Lateral meniscus remains intact without tear, degeneration or discoid morphology.”
The swelling has gone down a lot and I have good range of motion without any pain except when I squat down all the way or last 2-3 degree of full extension (very little pain; more of a restrict feel?)
Do you think it would be necessary to have a surgery?
I feel like I should wait and see how my knee does after the swelling has gone down completely.
Your opinion and advise is greatly appreciated.
Thank you in advance! =)
A bucket handle tear means that a large piece has flipped over and is caught in “the middle” of the knee. You may find it impossible to obtain full motion until that piece is repaired back to its normal position… or removed if it is not repairable. Good Luck
Howard Luks
Asem
Hello Dr. Luks,
I suffered an odd ‘injury’ 4 years ago (by standing and walking on one leg for a prolonged period of time). This was in the 8th grade. Ever since, I have had constant cracking and popping of my knee but it was very mild. A few months later, I was doing a trivial physical activity when I heard and felt a very loud pop in my knee. For the following 4 days, I was in a lot of pain and was hardly able to walk.
The doctor told me I had suffered ‘knee trauma’ and x-rays showed nothing was wrong.
I went on to do physical therapy (straight leg exercises) for 6 weeks. This therapy seemed to help for the time (less pain and popping) but unfortunately I did not follow through with my exercises (I do not know if I was meant to continue doing them). The pain and popping came back but it was always mild.
I continued to play sports and never truly gave my knee rest for more than a couple weeks. I play sports vigorously and I guess I tend to put a lot of stress on my knee as a result.
I am now a freshman in college and I have realized that the last few years have not helped my knee to heal.
After consulting another doctor and getting an MRI, it was found that I have a “small radial tear on the posterior horn of the lateral meniscus.” I have an appointment with a renowned surgeon in 6 days. However, I was wondering if you had any input before I see him.
The reason I am asking for input is because as he is a surgeon, I imagine he might directly assume surgery is necessary.
However, I would like to see if you think it might be possible for my tear to heal given I have this new information. I know they say that if it has not healed after a certain number of months (and my 4 years far exceeds that), then the patient probably needs surgery. But is it possible that my injury has not healed because I did not stop playing sports? Maybe if I do the right physical therapy, perform exercises that increase blood flow to the damaged area, and stop strenuous exercise for at least 3 months, my meniscus might have a chance to heal?
Thank you so much for your time,
Highly appreciated,
Asem
Ankur
Good Evening Dr Luks,
I recently twisted my knee and was recommended MRI. Following is the report of my MRI scan. Can you please have a look and suggest me what should I do next. The examining doctor has suggested surgery.
MRI OF THE LEFT KNEE.
CLINICAL HISTORY: Twisting injury while running. Possible ligament or cartilage injury.
TECHNIQUE: Multiplanar, mu1tisequential HRI of the left knee without intravenoue contrast.
COMPARISON: Conparison was made to the previous x-rays of the left knee done on July 21, 2013.
FlNDINGS:
There io a high-grade partial-thickness tear of the anterior cruciate ligament. There is a small area demonstrating mild depression in the posterior cortex at the lateral tibial plateau, indicating a mild impaction fracture associated with mild bone marrow edema in the posterior aspect of the lateral tibial plateau (image 20 of series 7). There is also mild edema in the posterior aspect of the medial femoral condyle, in the lateral aspect of the medial femoral condyle, and in the head of the fibula (styloid proceoo of the fibula). These are consistent with bone contusions from a pivot shift injury.
There is also a small incidental oval-shaped low signal intensity lesion in the proximal tibia metaphysis which is probably a bone island.
The posterior cruciate ligament is intact.
The medial collateral ligament and lateral collateral ligament complex are intact.
There is a T2 hyperintensity at the junction of the body and posterior horn of the medial meniscus, which is probably due to a post traumatic meniacal contusion. No distinct tear.
The lateral meniscus is intact.
The articular cartilage in all 3 compartments is grossly intact.
The extensor tendons are intact.
There is a small-to-moderate knee joint effusion.
No popliteal cyst.
IMPRESSION:
1. Partial-thickness t:ear of t:he anterior cruciate ligament. Mild impaction fracture in the posterior aspect of the lateral tibial plateau. Additional bone contusions in the medial tibial plateau, medical
femoral condyle and in the head of the fibula in a pattern that is consistent with a pivot shift injury.
2 . Medial meniscal contusion at the junction of the body and posterior horn of the medial meniscus. No distinct meniscal tear.
3. Small-to-moderate knee joint effusion.
4. Additional findings as described above.
Thank you.
Regards, Ankur.
Ankur…
The proper treatment for you will take into account more than just your MRI findings. Some ACL injuries do not result in instability or a feeling that your knee is loose. Some ACL tears cause significant instability issues. IF you are young, active and have an unstable knee then a reconstruction of the ACL might help restore stability to your knee. If your knee is stable and getting better with physiotherapy or time then you can wait and see what happens. In certain situations where people put themselves in precarious situations because of work (on rooftops or climbing trees, etc) then we usually recommend a reconstruction. The same goes for people who enjoy extreme sports such as rock climbing.
Good luck to you.
Howard Luks
Ankur
Thank you Dr Luks.
Ivan Ospina
I had a meniscus tear a year ago and doctor adviced me to rest 2 weeks, it was enough to me because I have recovered 100% my knee movement. This post is excellent.
Thanks Ivan !!
Jennifer
Good evening Dr. Luks,
I typed this once already but it doesn’t appear to be above. LOL. soooo here we go again.
In March/April I did something to my LT knee. It started hurting to where I couldn’t walk around the block from the pain. I had been doing a “30 day squat challenge” and working out on an older elliptical. I went to the doctor in May and had a normal xray of my knee.
Over the last few months, my knee has hurt but not as badly. I have started walking/jogging on a treadmill approx 2 mi a day. I also do an aerobics-type class twice a week. My knee aches afterwards but it’s not horrible. I do try to ice it afterwards. The worst part is when I bend my foot into my thigh (during a stretch), i can’t bend my leg completely w/out pain. My knee pops when I walk occasionally, but it does not feel weak or that it’s going to give out.
I went for an MRI today and learned there is a “complex tear of the body and posterior horn of the medial meniscus”. the lateral meniscus is fine, articular cartilage is fine, quads and patellar tendons are normal. cruciate and collateral ligaments are intact. I do have a small baker’s cyst.
I will be visiting with the doc about it tomorrow, but i was wondering what you thought about it. I do not want to have surgery. I am sure that he will push for it. My thought is that I will stop the aerobics class, and tone down the walking/jogging, but my concern is that I will injure it more. How do I know when I’ve pushed too far?
I appreciate your thoughts….
Thank you for this site! It has helped calm my nerves (and fears) about this diagnosis.
Jennifer,
Many meniscus tears can be successfully managed with physical therapy, activity modification, etc. If you fail to improve with those treatments then you have a qulaity of life decision to make. Given all options, some might chose to have surgery and some might not… but at least it was their own “informed” decision.
Good Luck
Sunil
Dr. luks I’m Sunil from India i want to ask you about my mother , MRI report shows that tear of knee cartilage .Due to this she is facing too much knee pain and also she cannot walk . sometimes her knee locks. sometimes unbearable pain occurred in her knee. Doctor suggests us arthroscopy but doctor said that pain may not be go ,so i need your advice should we do arthroscopy or not . can we try some physiotherapy first.
No harm in trying physiotherapy first. You also might inquire how much arthritis is present on the Xray. That may be why the surgeon doesn’t know if the surgery will help her. Once you have moderate to severe arthritis the likelihood that an arthroscopy for a meniscus tear will work diminishes dramatically.
Michael Beitchman
Dear Dr. Luks,
Thank you for your very informative video.
I have been told (based upon MRI) that I have a complex tear of the medial cartilage of my left knee.
I am 68 and for many years have noticed that the inside of my left knee is often larger than the inside of my right knee. Sometimes it aches mildly but has never really bothered me until a month ago when I had pain and very restricted motion. My GP prescribed a 6 day RX of methlyprednisolone which totally eliminated the pain and my limited motion.
Presently I have my long-time slight swelling and occasional aches as in the past. (I think I am more aware of these factors due to being told about the results of the MRI.)
I would like to know
– should I restrict gym activities such as cycling and aerobics (which often involves rapid motion and some twisting),
– if there is a “mild” degree of discomfort during the above activities, might I be doing more damage or could I just be more aware of the symptoms,
– is there a medicine like what my GP prescribed that I should keep on hand in the event of another
serious flare up,
– can a steroid shot into my knee sooth it and prevent problems for a period of time?
Thank you,
MB
Chances are you have had that tear for quite a while. You experienced a flare up, and it subsided. Although I can not issue medical advice, it seems logical that you can return to your prior activities. If the knee acts up, you can always act on it in the future. Injections are useful for episodic pain and swelling. Good Luck!
Deborah
Dr. Luks, I want to thank you for this blog — which I read until 2am last night. I feel much better prepared to make informed decisions when I go to the orthopedist next week for what I am now pretty sure is a tear (I did a Thessaly test on myself and yup, it hurt.) I’m 61, it happened two weeks ago but there was no swelling and my pain is only intermittent sharp twinges on stairs or when walking. So if I hadn’t found sites like yours I might have waited months and wasn’t even icing as I thought it would “go away.” Ha. Also, thanks to your blog, I realize surgery is probably not going to the best option given my age. I just wish I had known more ahead of time as had I had a healthy fear of “the dreaded meniscus” I might have done some things differently.
I also wish there could be more info on workouts for people (esp 50+ ) who choose not to have surgery as being active is the key for me anyway, to managing a stressful career. I really haven’t found a good website resource for this. For instance, I have figured out recumbent bike seems good (and did that today) but would like to see specially designed workouts and maybe a site that provides good advice — such as, can you do Pilates?
It seems especially given the New England Journal of Medicine article recently about non-surgical options there may be more interest in a conservative approach and how to live with tears and stay active. Any thoughts on resources for this appreciated! Anyway, thank you!!
Deborah… thank you so much for your kind praise. Along the years I have found that many patients with meniscus tears and osteoarthritis do well with some activities, but not others. Sadly, it also varies patient to patient. What doesn’t hurt one patient, may hurt others. In general “uniplane” activites… only moving in one direction without turning, pivoting or twisting — are better tolerated. Some patients tolerate Pilates, and Yoga, yet others do not. So I try to work with each patient to see where their comfort zone is and work with the therapist or a trainer to design a program to suit each individuals needs.
I know it’s not what you were looking for… but I hope it helps nonetheless.
Howard Luks
Eshan Arora
hello sir,
My name is Eshan arora & i am from India.
On 8th July, 2012 i suffered an injury while playing soccer with my friends. At first the pain was unbearable and it took me around half an hour to go back to my house which in normal condition takes only 5 minutes. After reaching home i took some pain killers and applied pain relieving gel on my knee. For the next 2 weeks i had 0 activities and started doing my work slowly. after that i went to a physiotherapist and started my rehab their. After 2 months of physiotherapy i was finally in good condition and was able to walk properly, do my regular exercises, do my work and there was only a slight problem in going down the stairs. I continued my physiotherapy for another month and then stopped going there but i was still doing my exercise my doctor told me to do everyday.
Then after 2 months, while i was playing Cricket (As he had recommended me to not play soccer ever again) i felt some pain in my knee again, so i stopped playing and went to my doctor who told me to get a MRI scan for the knee and i went to the hospital and underwent the MRI scan. the report is provided at the end. Everything was going fine, but one day while sleeping i was turning my position and suddenly i felt a snap in my knee and pain started in my knee and it was very severe. So, i went to my physiotherapist again and with the help of a 2 week session i was not feeling pain.
The MRI report states that :-
“The study shows normal configuration and alignment of the bones forming right knee joint.
Linear hyper-intensity is seen in posterior horn of medial meniscus on PD fat sat images reaching up-to inferior articular and capsular surface suggestive of Grade 3 tear.
Altered signal intensity, appearing hyper-intense on PD fat sat images noted in anterior horn of medial meniscus extending up-to articular and capsular surface suggestive of complex tear.
Lateral meniscus is unremarkable in MR signal and morphology.
There is focal contour bulge in middle third of anterior cruciate ligament with heterogeneously hyper-intense signal on PD fat sat images sprain/ partial thickness tear.
The posterior cruciate ligament is unremarkable in MR signal and morphology.
The medial and lateral collateral ligaments are unremarkable in MR signal and morphology.
Medial and lateral patellar retinaculum are unremarkable in MR signal and morphology.
Quadriceps and patellar tendons are unremarkable.
Hoffa’s pad of fat is unremarkable.
Fluid intensity mild collection seen in suprapatellar bursa and in lateral and medial recess of knee joint”.
In all finding are:-
1. Grade 3 tear in posterior horn of medial meniscus.
2. complex tear in anterior horn of medial meniscus.
3. Sprain/Partial thickness tear of anterior cruciate ligament.
4. mild joint effusion.
Please suggest whether i should opt for an Arthroscopy surgery or not & if i want to play again what should i do.
Thank you
If you are unhappy with your quality of life, then a repair of the meniscus might be able to assist you in getting back into an active lifestyle without discomfort.
Good luck,
Howard Luks
Eshan Arora
thank you Doctor Howard for you reply
Sandy
Hi Dr. Luks,
This site has been super informative. I love your approach to healing.
Obviously, I’m here for a reason. I’m a 39 yr old female runner, skinny. Run 40-50km a week. I’ve had varying degrees of PFS, but I’m stymied by something new on my left knee.
I don’t recall a specific injury, but my patellas pop etc regularly, and frankly, I could have done something and passed it off. No swelling or redness. I noticed a dull ache medial joint line, approx 3/5 of the way posteriorly. Deep palpation on the joint line here is painful. Deep squats or trying to lock my knee in extension brings along something akin to hitting my ulnar nerve! I cannot bring my heel to bum anymore.
This was three weeks ago, and I still ran on it until a week ago, when my GP suggested a rest. She won’t refer me for an MRI, which is fair enough, but driving me bananas when I want to know what lies ahead. After a week, the pain has not changed, although I am still doing some light swimming, and walking.
I am suspicious its a medial menisci tear. My knee feels a bit wobbly as well. Should I continue taking time off, or can a I continue to run through this? Will continued running make it worse? I was training for a marathon in November, and have another booked in February. Add that in to my runner’s brain…and you can only guess how this is driving me mad!! I need to lace up!
Thanks in advance!!! Sandy
Thanks Sandy .. I understand your plight, runners do have a very unique personality and NEED to run to feel complete. Tough for me to say what is bothering you. Likely suspects in that area include the meniscus, the pes tendons ( snapping tendons, or pes tendinosis, bursitis) as well a posterior articular cartilage injuries. Of course there are many other less likely possibilities. Getting runners to rest is very very difficult. Especially when you do not have a source of pain, and therefore do not know if it will improve with time, etc. If not an MRI, perhaps a visit to an Ortho will set you on the right course.
Good Luck
Howard Luks
Debbie
Hello Dr. Luks,
I injured my knee 2 years ago while doing Zumba. I twisted to my right and my knee didn’t make the turn. OUCH! I rarely experienced pain the last 2 years. Lately, I have intermittent pain while walking. My regular Physician advised that I do not need to see an Orthopedic Surgeon/Sports Medicine Doctor unless it is bothering me constantly. He also agrees with you that leave it alone as long as I am having quality of life.
Now for my question? The pain is more frequent & my hips are extremely tight. I used to be able to do Yoga and sit cross legged. Now, it is too painful to cross my leg & pulls my knee. I have also been doing an exercise program called barre Amped which is isometrics including squats & lunges. I’m fine while doing these exercises but feel the pain afterwards. Is the hip pain a secondary condition to the knee and are there stretches or exercises that I can do which will loosen my hips and leg muscles? Should I make an appointment with an Orthopedic Surgeon or a Sports Medicine Dr. to get a diagnosis?
Thank you for this website. I’m so glad I found it and your wonderful advice.
Thanks Debbie… I’m glad you found it useful. I would think that a set of X-rays and an evaluation by an Orthopedist might be able to tell you why your hips are bothering you. Hip pain can be secondary to knee problems if our knee pain alters our gait, etc. But if your gait is normal, then perhaps something in the hip is responsible for your stiffness and discomfort.
Howard Luks
Vicky
Thank you so much – especially the reparable information!!! great to know and I will push this option. Other options very welcome and I really like the tart cherry juice version of an anti-inflammatory. Thank you again!
Vicky
Vicky
Hi Dr Luks
Thank you for your wonderful site and your helpful advice.
I am 64 and have medial meniscus tears in my right. The MRI scan notes that ‘There is a peripheral vertical tear of the body of the medial meniscus and there is meniscocapsular separation of the body and posterior horn of the medial meniscus. A small subcapsular medial and later joint effusion is present and extends into the suprapatellar bursa – possible media patella plica syndrome.’ Everything else is fine and my Xray shows no arthritic conditions.
I have an appointment with a sports-oriented orthopedic surgeon – my referring doctor has said that the OS will recommend an arthroscopy and, on investigation, is likely to remove the medial meniscus due to my age and the reduced healing capability of the meniscus.
What are the likely negative health outcomes eg arthritis etc resulting from the removal of the meniscus and what alternatives can I discuss with him – is an allograft at all feasible?
Thank you,
Vicky
Thanks for stopping by Vicky…
I assume you also have pain? Not a silly question believe it or not :-)
The treatment alternatives include
* time: just waiting to see if the symptoms will subside with time (not all tears hurt, and many will become nearly pain free)
*Physical Therapy — surprisingly useful for many
*activity modification – for some a reasonable option
*medications: natural (tart cherry juice) or routine anti-inflammatories (assuming you are allowed to and tolerate them)
*arthroscopy – many will do well… some will not. Middle aged women have a small, but not insignificant chance of getting a post-menisectomy (after arthroscopy) stress fracture in the bone. This can lead to numerous problems including the potential need for a knee replacement.
Lastly…. your tear IS in the repairable zone. Most middle aged folks do not have repairable tears… but sometimes they do. It is always best to attempt a repair, if the meniscus appears to be repairable. The risk is another arthroscopy down the line to remove a piece that doesnt heal. However, minimizing the risk of developing osteoarthritis is worth the risk. In my opinion.
Good Luck with your decision making.
Howard Luks
Linda
I am a 53 year old woman and recently injured my knee somehow and had an MRI done. The report says no medial meniscus tear, however there is a linear tear involving the posterior junctional zone and posterior body of the left lateral meniscus , which extends posteriorly into the posterior horn. It exits on to the undersurface. This is associated with a bilobed 4×8 mm meniscal cyst, is this something that requires surgery? It also says there is edema and fluid around the anterolateral margin of the knee. I am getting worse and worse as far as pain goes and even my hydracodone doesn’t work sometimes. I thank you for your time.
Curious to learn more about the edema… a common source of pain.. and if it did not follow an injury or traumatic episode it may be due to arthritic change ??? I can not say without seeing your images … or you. But this is something you need to nail down with your doc.
Good Luck
Howard Luks
Jeff
Hi Dr
I am a 4 day a week runner age 55. MRI shows a Linear horizontal tear within the posterior horn of the medial menial meniscus, extending to the inferior articular surface. I have an $8000 pay first deductable and can not afford the cost of arthroscopy (quote $5000 to $8000) Is this something I can shop or do you have any suggestions. I can not run and am going crazy! Thanks Jeff
Jeff…
If the quote was just for the surgeons portion of the bill then it is certainly negotiable… Let me know if I can be of further assistance.
Good Luck.
Howard Luks
Rick
(corrected email address)
Hi – I am an active 58 male and had subtotal medial meniscectomy in Jan and also had some osteoarthritis issues that were present in my knee. After numerous PT sessions and staying off the knee for a few months, I still experience sometimes severe pain just below my kneecap that my doctor says is most likely bone stress or small fractures and I should allow the bone to heal. I now have a uploader brace(DonJoy) that I use when I am walking a distance but want to get back to my activities of sports, exercising, and working out regularly. Your recent article about knee pain after surgery where you stated “bones around the knee joint “see” more stress when you walk and they react by becoming very inflamed and can actually at it’s worse, cause a stress fracture which is quite painful.” sounds exactly like what is going on with me. I have had a follow up MRI which conclude that possibly that is what has occurred, and I have tried to take it easy however still have pain in the knee that seems to tweak and hurt right at the medial joint line below the knee cap.I have had rounds of orthovisc also,
MY question is what can/should I do to get this better and will and WHEN will this heal? I do want to get active with exercises and cardio workouts again but want to know that It can heal adn what time frame am I looking at?
thanks very much for your response as I can use some more information on this!
Rick
Thanks Rick…
These post-menisectomy changes can take a while to resolve… if it is going to resolve. Sometimes people need to be on crutches for a short while — sometimes we consider a procedure called a subchondroplasty which gives the bone the support it needs to deal with the stress and “heal” the stress reaction.
I hope this helps.
Howard Luks
Christy
Hi, my 11 year old fell at school (running backwards as instructed to do in gym class) and when she fell her leg twisted and went underneath her. At first her primary complaint was her ankle. As time passed and x-rays were negative her ankle pain diminished and was replaced with knee pain. She has had a MRI which showed a surface tear of her meniscus and the tear is horizontal. The most painful spot on her knee is to the side. Her orthopedic says that is where the knee fluid has drained and formed cysts. He didn’t explain anything else except that she needed surgery and he would not know till he was inside her knee whether or not he would be able to repair her meniscus or if he would just have to remove it. That if he would remove it her recovery time would be much less but she would most likely have arthritis when she got older. She is in pain. Where it seems to be draining is swollen.
My dad is old school and does not believe in going to the doctors for much of anything and says she will grow out of it. But she is in pain and her orthopedic did not see fit to explain much to me before he left the room. Little did I know he wasn’t coming back. How bad is the pain after the surgery. Will she be in a lot of pain? I learned so much from this website, I can’t thank you enough for all this information. The video’s freak me out, thinking about someone probing in her knee like that but I do understand that’s how it is done.
Do you think an 11 year should have surgery and how bad is the pain after surgery. Is she going to be able to walk that day and if not when?
thank you so much,
Christy
Christy… Sorry to hear about your daughter. 11 year olds rarely get horizontal tears. Those tears typically occur in older adults. A child’s meniscus is different from an adult meniscus. It has more blood supply. Sometimes that blood supply confuses a radiologist who may think the signal represents a tear. That being said… Most sports medicine docs will fix nearly all tears in someone so young… assuming the tear is present. By fixing, I’m implying suturing it back together. The downside of having meniscus removed at this age is very significant. The chance of a successful repair is higher in your daughter’s age group because of the increased blood flow… and increased healing capabilities of children.
I think you need to consider a second opinion on your MRI reading. There are some online reputable second opinion services available. Assuming a tear is present, you might want to find another surgeon who is Sports Medicine trained, willing to sit and talk with you, and hopefully willing to consider a repair over a removal of the torn piece. I wish you luck and hope your daughter gets better soon!
Please remember that my disclaimer needs to apply.
Howard Luks
Jere
Hi Dr. Luks,
Thanks for those detailed and very informative videos! I’m a 40 year old male with excellent health. 4 weeks ago, I twisted my knee in a cardio exercise class. Pain started next day, knee was stiff, limp set in. Very little swelling. No locking and I had full range of motion. But, when pain/stiffness didn’t improve with Advil & ice, was forwarded by primary doctor to PA-C in orthopedic department. Did an MRI, which came back with “Partial root tear of the posterior horn root attachment of the
mediai meniscus. Mild proximal patellar and distal quadriceps tendonitis.”
From week 2, I started using crutches and physical therapy under PT guidance and pain slowly but steadily started reducing. At 4 week appointment yesterday, I was advised by the PA-C to walk without crutches, which I did throughout the whole day, albeit with a little limp but no pain. However, by late evening/night swelling came back and pain was as bad as it was 4 weeks ago. Started crutches again last night and after 24 hours, pain reduced by 50% again.
I’ve been now forwarded to meet orthopedic surgeon next week. Not sure if he will recommend arthroscopy straightaway. Do you think I should give it more time to settle or 4 week wait so far is enough? I’m scared to let go of crutches for the fear of pain coming back, but quality of life with crutches is not best either. :(
Thanks in advance.
-Jere
Jere… It’s not common for a partial root tear to lead to significant swelling. It’s possible, simply not common. Were any “degenerative”, “chondromalacia” or arthritic changes seen on the X-rays or MRI?
Jere
Thanks Doctor for your reply. Since my original post, I met the surgeon for the first time, who went over MRI & X-rays and did an exam. No, none of “degenerative”, “chondromalacia” or “arthritic changes” were mentioned. (I did ask about arthritis and he said that from that point of view knee is in good health – good spacing, full cartilage etc.)
About the surgery, he said that he doesn’t see anything compelling that is indicating a surgery right away. Instead, he advised me to continue PT for up to 8 more weeks, and only if symptoms won’t go away, then he is going to revisit the decision. His gut feeling is that surgery will not be needed. Hope things do turn out that way. :)
-Jere
Jere
I wondering why is there no response yet, when realized that I missed to ask an explicit question! Sorry.. I wanted to know your opinion on the conservation treatment plan my surgeon has recommended. Have you seen patients where they avoided surgery for ““Partial root tear of the posterior horn root attachment of the
mediai meniscus.”? Or these kind of tears never get better without surgery? Thanks!
Jere
Dr Luks,
Still waiting for your reply. :)
– Jere
Jere .. as I said on 5/2/13 and as you mentioned when u discussed your surgeons thoughts… it is unlikely that a partial root injury would lead to significant pain, swelling ,etc. Perhaps the tear is larger then it looks on MRI ??? Perhaps there is something else that the radiologist missed? Too many open questions… perhaps a second opinion on your MRI reading? Perhaps a new 3T MRI?
Good luck,
hjl
Palak
Hi Dr. Luks,
You are doing great job by giving right advice .Checked your website and videos too.
Jere
Hi Dr. Luks,
It’s been 4 1/2 months since injury and sadly all the PT routines I religiously followed have not helped. I walk to work ok in the morning, but starting around noon, the knee feels really sore, stiff and bad limp comes back. (I’ve a desk job, but I do get up frequently and stretch.) From that point onwards symptoms stay until I go to bed in the night. The knee only feels somewhat ok after waking up in the morning. I’ll be meeting my surgeon again to explore the surgical options. :( Hoping that the knee will get back to pre-injury state after the surgery and rehab. :)
Thank you again on this wonderful blog and answering all poster’s questions for a long long time.
-Jere
Louisa
Ok thanks. Are the tears quite bad – bad enough to need surgery do you think?
I was once very overweight so wondering if this has caused degenerative damage. I don’t have signs of Lyme disease or gout. As for arthritis, the only other knee related issue is non-painful crepitus in my other knee when I walk up and down stairs.
Louisa
Oh and isn’t the large knee effusion because of the tear? I still did aerobics for 15 mins a day, and some of that involved leg lifts whilst hopping on one leg. That was at the time of the MRI. I don’t do those anymore and the swelling is virtually non-existent now. I do still exercise but I avoid the knee-crunching ones!
L,
Given the findings on the MRI, even the radiologist isn’t impressed — these small tears are unlikely the source of the swelling. As the radiologist suggests, a thorough work-up (blood tests) for tick borne illnesses (Lyme, etc) and “inlfammatory” arthritis and gout (crystalline arthritis) would be a good place to start.
Good Luck
Howard Luks
Louisa
Hi
I was wondering if you’re still answering questions. I am 31 and tore my left meniscus. I don’t remember any specific injury, I just woke up and my knee was swollen. I carried on my daily exercising and after 24 hours it was swollen and uncomfortable. Not quite painful but almost. It was painful to walk up and down stairs though and when I bent my knee a lump appeared on the outside. I had an MRI and here are the findings:
Medial compartment – normal meniscus, preserved anterior cartiliage.
Lateral compartment – minor blunting of the free edge of the meniscus body, indicative of a small radial tear. Small vertical tear of the anterior horn, extending towards the root attachment. the remainder of the meniscus is intact. Normal anterior cartilage.
Patellofemoral compartment – mild heterogeneity of the lateral facet articular cartilage. No discrete defect. Preserved trochlear articular cartilage.
Ligaments – normal cruciate and collateral ligaments.
Other findings – large knee effusion. No MR evidence of synovitis. Normal posterior tendons.
Impression – large effusion with no significant intra-articular pathology to explain it. Given the patient’s age. gender and clinical history a an inflammatory arthropathy needs excluding.
___________________________
So I have 2 lateral tears – are they bad?
And what’s the blunting of the free edge mean?
And the heterogeneity?
Do you think it’s a sign of degenerative tear rather than acute? I’m only 31, no history of arthritis type diseases, and I’m female.
I don’t suffer from pain anymore. Can walk fine, up and down stairs is fine too. However my knee occasionally catches if I twist, and I can’t do a deep knee bend (eg I can’t sit on my haunches)
Nikunj
I writing in concern to the right knee pain of my mother-in-law. She is 56 years old. She has this severe pain and swelling in her right knee since 3 months now. She went to India for treatment (no insurance here). MRI was done over there and report came out as “mild changes of osteoarthritis with mild joint effusion and Grade 1 mucoid degeneration in posterior horns of medical and lateral menisci”. The fluid was aspirated and was treated with medicines and physio therapy. She felt better after that. After she came back to USA, she was ok for a few weeks and now the pain and swelling reappeared. The pain is severe affecting her sleep and daily activities. She is taking NSAIDs without any benefit. She was also dignosed with “frozen shoulder”. What would you recommend for her? And if arthroscopy needed, how much does it cost without insurance?
Thank you in advance.
It doesn’t sound like an arthroscopy would be useful. Mucoid degeneration is not a tear. The likely source of her pain is inflammation from the arthritis. Even mild arthritis can cause significant inflammation. I would try another course of injections…. hopefully an Orthopedist in your area can talk to you about the various medications we have at our disposal.
Howard Luks
Djordje Cenic
Dear Dr Luks,
First let me say how grateful I am for your objective and sincere article that puts the interests of the patient in the spotlight. I’m a 37 year old male with meniscus problems. When my surgeon recommended arthroscopy on my knee, my first reaction was to do as he says immediately. Luckily, two things changed my mind – my physiotherapist and your article, so I opted for physiotherapy first. However, two months of PT are not showing good results so far. Now even my physiotherapist thinks I should have surgery, so I would like to have your opinion on a few things.
The actual MRI findings are not convincing at all. They show “degeneration and possible lesion of the medial meniscus”. The surgeon said that the MRI is inconclusive and that the lesion is “possible” and he can confirm it only when he operates.
My knee doesn’t lock, it pops just a little, I can extend it, but I cannot kneel all the way down to the floor without a sharp pain. In fact, my problems started after I did a quad stretch that involves kneeling all the way to the floor and extending the torso backwards. My degenerated meniscus couldn’t take it – it was the last straw.
If I jog for 20 minutes, I feel strong and well defined pain in the area around the medial meniscus and I have swelling and I’m limping for 3-4 days after that. Six months after the injury and after 2 months of PT, my knees are stronger and more stable, but I still cannot jog, jump or kneel without consequences. After sitting on a low chair for an hour or so, I feel pain in the knee when I stand up.
Since I have degeneration in the meniscus, I am aware that I will have limited benefit from a surgery, that partial menisectomy is probably the only option, and also that I will have increased risk of arthritis, so I want to avoid the op at any cost.
My questions:
– General opinion is that meniscal trear with “mechanical” symptoms should be treated with a surgery because they can cause damage if untreated. Are inability to kneel all the way to the floor or sit for long periods without pain considered a “mechanical symptoms” of a meniscal tear?
– I’m ready to give up jogging and jumping and live like that. I’m not an avid jogger anyway and fast walking is good enough replacement for jogging. However, my physiotherapist disagrees. Her opinion is that I should be able to jog or jump occasionally without having pain and swelling the next 4 days. Is a patient that is unable to jog 6 months after injury and 2 months of PT a candidate for a meniscus operation?
Thanks in advance and thanks for writing this article in the first place! It is an eye opener for many patients worldwide.
/Djordje Cenic
Djordje…
I truly appreciate your kind comments!
It does not sound like you are having mechanical symptoms, such as snapping, painful popping, locking, etc.
If the MRI does not reveal and obvious tear, then something else might be the source of your pain… or the radiologist could have mis-interpreted your MRI.
Without examining you it is not possible to offer concrete medical advice. I would say,however, that the decision is yours… and it should be based on your quality of life- given the limitations that you expressed. Without a large loose piece of meniscus or debris floating around your knee, it is unlikely that you are risking further damage by not having the surgery.
Good luck to you…
Howard Luks
Joe Catazone
Hi Doctor…..I am 55 years old, 6’3, 225 and have been playing pick up basketball 3 days a week for 30 ish years. I had some knee soreness a couple years ago and had an xray and was diagnosed with osteoarthritis. I bought a couple of Ace knee braces and played with those to satisfactory performance. Last month I twisted my right leg on the court and felt a tear, had an mri and revealed “lateral meniscus posterior third tear with displaced fragment, also medial meniscus tear, lateral tibiofemoral compartment predominant osteoarthritis with antra-articular osteocartilaginous bodies, large joiny effusion, synovitis”. I have an appointment with an ortho surgeon Monday and stopped playing basketball as I can’t cut and have been doing spinning which has made my leg feel better. I want to keep playing basketball and know I have osteoarthritis but was ok playing with the braces before the tears. Will meniscus surgery get me back on the floor? Thanks!
Tough call Joe… it might… but it might not. Time to have a long sit down with a sports doc. Good luck!
marc klug
Dr. Luks,
I am 47 years old, physically fit and very active with tennis, snow skiing, and bicyle riding. In addtion to playing with my three young children.
In Oct. I crashed my bicycle and had severe pain in inner leg..Due to poor insurance I had xray but no MRI…I rested and after a month it felt better except when i twisted my toe out. I have one spot on inner knee where i can apply pressure and generate pain.
I had an MRI and it showed:
1. complex tear medial meniscus
2.moderate patellofemoral chondromalacia
3. degenertative arthritis medial and lateral
I can’t play tennis or ski without pain otherwise I am pain free unless my foot gets twisted out. The orthopedic recs removing part of meniscus up to 40%. If I opt not to do that do I risk further injury due to the tear still being there? Does the pain mean there is new tears occurring?
Thank you,
marc
Marc… this is a difficult treatment decision. Whenever arthritis and a meniscus tear is present you need to understand that the arthroscopy can not treat the arthritis… and your arthritis will likely worsen once a portion of your meniscus is removed. Any decision to treat this surgically must be weighed against the severity of the arthritis and the knowledge that your arthritis symptoms will not improve after an arthroscopy — typically.
Howard Luks, MD
jayesh
hi sir,
i am a 26 years old male living in mumbai.i met with an accident wid motorbike.from that day my right knee has got greeding sound while using stairs for going up n down.i have taken advice for this n got mri of knee.my orthopedist is suggesting for surgery n saying after putting arthoscope he is going ti decide treatment option i.e. stitching or cutting of meniscus.m not having pain while normal walking only when using stairs somtimes there is little pain in knee.my mri report is as under.
hyperintensity is noted in posterior horn of medial mensicus, not reches upto the articular surface, suggestive of grade 2 tear.
subarticular cystic changes are seen in the intercondylar region of tibia,could suggest degenrative changes.
knee jooint space is normal.
patello-feromal space is normal.
lateral mensicus appears normal.
collateral ligaments. ligamentum patellae & quadriceps tendon appear normal.
articular margins of femur appear normal.
no evidance of any fracture.
periaticular muscle plane sare normal.
my question is whether surgry is neccesary for the knee?will this tear can not be treated by medicines or some injections?pls giv me valuable advice m so much confused.thanks
Jayesh
April Williams
Dr Luks, Thank you for your site and all the information you have put on here. I wanted to see if I could get your opinion on something. I started having pain in my left knee in September of 2012. I had significant swelling and pain. I could barely walk and could not bend my knee. At that time most of the pain was on the medial side of my knee. Xrays didn’t show anything so I went to an orthopedic surgeon who sent for an MRI. I do not have a copy of the MRI, so I don’t know what it all showed, other than the doctor telling me there was no sign of arthritis, and that I had tears in the medial and the lateral meniscus. At the time I didn’t realize there were types of tears or I would have asked.
I was still having pain, but could walk a bit better after about 6 weeks. He told me that I had two options, one was surgery to remove the tears and the other was to try PT. Not really understanding, I said I’d like to try PT first. Now I’m wondering if that was a mistake because the pain is just not going away.
I am going back to see this doctor again and would like to know if there are any questions I should ask him to determine if I should have surgery or not. My knee is still not completely better. I have good and bad days, but it swells up quite frequently and I still cannot bend it. Does that suggest I should just have surgery? I am worried I will injure my knee further. Again, I wasn’t given specifics and I never got a copy of the MRI. I am also overweight, so I am wondering if that is hindering my ability to heal that area. Never had knee problems before this though.
I’d consider a second opinion, however, I am on Medicaid and there are no other ortho doctors in the state listed for my plan.
Thanks for any info.
April Williams
Alex
Hey Dr. Lucks,
I just want to have a second opinion well i took an MRI and my results said “small joint effusion. Focal incomplete vertical partial of the most posterior edge of the posterior horn of the medial meniscus with partial tear of the meniscocapsular juction posteriorly. ” My doctor said just to brace my knee so my knee wont bent for 2-4 months and it should heal . I was reading also it depends on your age I am 19 would that take any affect. I got injured playing soccer, i play competitive soccer so I want to return. I dont really have much pain. Is there anything else I should do besides putting a brace on .
T
Hello Dr. Lucks,
I very much appreciate your willingness to help so many of us out thru this blog. I am a 33 yr male that lives a fairly active lifestyle (triathlons, baseball, mountain biking etc.) I woke up one morning, about a month ago, and found that my left knee had a tremendous amount of pain when trying to bend/walk on it (likely injured from aggressive baseball game the night before). After limping along for a few days the constant pain started to subside, and it moved into only pain when I tried to bend my knee completely. As of today I can run on it with no immediate pain, but within a few hours, a dull ache sets in, and there is still a sharp pain if I try and bend the knee completely. I had an MRI done and during my visit with the dr. today, discovered that I have a complex medial meniscus tear.
Is this type of tear something that is typically repaired or removed? I’m concerned for the long term based on the dr’s comments that he plans to remove the damage, which will likely be 2/3 of my medial meniscus. What should I consider that would get me back to my active lifestyle with least chance of future problems?
Thanks in advance for your time and consideration.
-Troy
Troy … We never know if a meniscus is repairable until we are in the knee and looking at it. That said there are also surgeons who are far more prone to attempt a repair than others. Find one :-) Decision making around meniscus tears is not easy from a patient’s perspective. IT is a quality of life decision whether or not surgery is necessary. There are complex, involved options available to those who have had significant pieces of meniscus removed and have pain with early arthritic changes setting in…
Howard Luks
Renee Louise
Dr Luks, you are so right about the decision concerning meniscus tear is difficult for the patient!
After a MRI, it was discovered that I have tear in my medial meniscus, and also an oblique tear in my lateral meniscus.
I cannot ski this winter, it is difficult to walk for any lenght of time and my life is at a standstill.
I saw an orthopedic surgeon who immediately told me he would shave off the tears arthroscopic surgery. But, that surgeon fractured his right wrist! and I am on hold.
I saw another surgeon who tells me that it will heal, no surgery for that! Oh, I also have a Baker’s cyst. I happen to be 61 years old, very active, and a ski fanatic, I do not intend to stop living for a meniscus. After reading about this a lot, I discovered repairing the meniscus. I know it is usually done on young patients, but could I volunteer? I am ready to try anything. It would be awesome if you could answer me. I am from Quebec, Canada
Only certain tears are repairable… also at 61 make sure the MRI does not mention cartilage wear, arthritis, bone spurs, bone edema, or Grade 3 or 4 chondromalacia. All those could significantly affect your overall recovery.
Howard Luks
Renee Louise
Thank you so much for answering me . I just looked at my report and it specifically says: no cartilage fine, no arthritis, everything normal except many little tears at edge of medial meniscus and diagonal tear on external meniscus between tibial articulation and middle and posterior meniscus. I am trying to translate this from French!
It is mentionned that the tear on the external meniscus seems to extend all the way to the edge, unless there is another tear there.
I also have a small Baker’s cyst. No anomalies to bone structures.
I would really really love if they could repair my lateral meniscus. Am I too old???
Alex
Hey Dr. Lucks,
I just want to have a second opinion well i took an MRI and my results said “small joint effusion. Focal incomplete vertical partial of the most posterior edge of the posterior horn of the medial meniscus with partial tear of the meniscocapsular juction posteriorly. ” My doctor said just to brace my knee so my knee wont bent for 2-4 months and it should heal . I was reading also it depends on your age I am 19 would that take any affect. I got injured playing soccer, i play competitive soccer so I want to return. I dont really have much pain. Is there anything else I should do besides putting a brace on .
Bilal
Hi Dr. Luks,
Thanks for this very helpful piece of information. I just wanted your thoughts on something that I have been thinking about for the past few months. I had an MRI done last December and it said ” horizontal tear mid to posterior horn medial meniscus”. Everything else was in tact per the MRI.I did have considerable pain on the medial side but it wasn’t anything I couldn’t deal with. So even though the doctor suggested surgery I decided against it. This time around a couple of months ago I had started getting some pain on the lateral side of the knee and was worried that I might have torn my lateral meniscus after getting an MRI done the doctor (knee specialist) showed me the MRI and while the lateral meniscus was intact he said the medial meniscus showed signs of degeneration. I am not sure how serious it is but he said it was fairly common. Also I am not sure if by degeneration he meant that the tear that I had was a degenerative tear. In any case, do you recommend supplements or any other measures that I can take to strengthen my medial meniscus please?
I wish there were supplements or medications that would heal a meniscus tear… sadly they do not exist… to my knowledge.
Howard Luks
Naren
Hi Dr Luks,
Thanks for the amazing blog. I have a lateral and medial meniscus tear and significant cartilage wear. I can still bear the pain and I experience pain after the workouts and sometimes even while sitting or walking. I have future plans for triathlons. My doctor here told me that I can go for arthroscopy to determine the degree of damage since MRI doesn’t show much. I’m 35 and this injury has been there for the past 3 years, I but managed to recovery pretty good and still be active until recently where the recovery is taking a week and pain level is getting higher.
I was given 2 option by my doctor:
1. Play less (basketball,running,tennis) and do something else (swimming…etc)
2. Arthroscopy – do cleanup of the torn meniscus flaps, and floaters. If its bad replace with cadaver. With cadaver i can probably do 1 or 2 triathlon in a year and should be good. Although cadaver can tear easily within 10 year depending on the use. For my case it should last to 10year at least. So far whoever has done with him is doing good and couple of races as per him. 70% success rate
I would like to know if cadaver is really efficient? I haven’t seen any news on pro’s using cadaver (meniscus) and since I don’t have the statistics is option 2 really believable? I dont mind going with option 1 if the chances of tearing the cadaver is very high if I do triathlons and play basketball.
Thanks for the help
Naren,
I appreciate your kind comments! Cadaveric meniscal implants are an option for people who have lost a significant portion of their meniscus and have persistent pain. The only issue I’m unclear about is your mention about significant cartilage degeneration. That usually means osteoarthritis. If you have significant arthritis the results of a transplant will be far more unpredictable.
good luck with your decision making!
Howard Luks
Amy
My daughter is a college soccer player. She sustained an injury during practice and has pain lateral to her patella. If she extends her leg with walking, it buckles to the front. Her MRI shows a tear in her popliteus muscle at the myotendinous sheath, a tear centrally in her lateral gastrocnemius muscle and fraying at the anterior horn of her lateral meniscus. According to the MSK radiogogist it doesn’t look like the fraying extends to the anterior root. He thinks it is something that should scar down. The orthopaedic resident at the varsity clinic told my daughter that she had a hard to repair vertical tear in her lateral meniscus and she needed surgery. She said if she doesn’t have surgery something may break off and damage her cartilage. We will, ofcourse, be going for a 2nd opinion but we won’t be able to do that for several weeks. What is your opinion about the discrepancy between the radiologist and orhopedist opionions.
Please bear in mind that this is not medical advice… Any injury to the popliteus and its fascicles usually needs to be looked at by an experienced sports medicine physician. A unique form of instability called postero-lateral instability could exist without injury to the LCL or either of the cruciate ligaments. I would be sure she is assessed soon by a well trained experienced sports medicine doc.
Good luck
Howard Luks MD
NamePam
I have pain in my knee just under my knee cap and up the inner aspect of my knee, It has been coming and going since an injury in 2009 . Recent MRI results :moderate focal thinning of articular cartlidge with reactive subchondral marrow edema and cyst formation of the anterior 1/3 of medial tibial plateu.
moderate joint effusion .Osteochondral lesion with subchondral cyst,moderate chondromalacia patellofemoral , degenerative fraying posterior horn of the medial meniscus.
What are my best options for tx. I am a 50 yr old RN who works 12 hour shifts 3 x a week
Gerardine
Hi there,
Sorry i have copied and repasted most of my questions/concerns as seems i may have been missed,,, i would really apprecoiate any thoughts or observations you can offer please…
While I was kneeling down on both knees, and as i turned/twisted my upper body to the right, i felt intense pain behind my left knee and it was locked in a 90 degree angle with me unable to straigten my leg for 10-20 secs. It feels to me like it was the hamstring ‘snapping over’ and stopping my leg from extending, This is something which i have experienced about three times previously in my life. and in the past, it has only felt a little bruised afterwards but then back to normal, so never needed to consult a doctor. But this time. I have been in a lot of knee pain, it became sore, swollen and pain, particulary on the inside of knee, cap area and inside knee. I am unable to drive, walk up stairs and struggle getting up from sitting down or putting any pressure on it or twisting it for the last 5 weeks… although the pain has reduced somewhat, i am still very limited especially with stairs.
I have had an MRI scan and the doctor describes “some degenerative signal which is perhaps in fact indicative of a horizontal cleavage tear of the posterior horn and body of the medial meniscus. This is not an unstable tear configuration however and it is curious that this should cause such symptons and such severe symptons if indeed it is the cause”. He goes on to say that it is nevertheless the part of the knee that is hurting me and is the only obvious abnormality. I have a history of fibromyalgia and sciatica (which is occassional now) in my other leg, which are completely manageable and in my mind are unrelated to this knee problem.
He is reluctant to do an anthroscope as he would have to remove a substantial portion of the menisci and is recommending in the first instance to try physio. Though i feel its wise, i don’t really understand how physio will help a tear?
My doctor says my tear is stable and I am confused by comments on your web page that read “If you sustain an injury and you have a very unstable tear, a tear we call a horizontal cleavage tear or a radial tear or a flap tear, those tears tend to remain symptomatic —and if after four, five, six weeks, you still have the same degree of discomfort and quality of life issues, then you might be a good candidate for an arthroscopy.” I am concerned by the different descriptions as my symptoms are stlll around after 6 weeks and impacting me (cannot drive or do stairs and feels like a grating bone against bone pain) …and i am thinking surgery may be needed…?
Thank you in advance for taking the time to read this email.
Best wishes, Gerardine
Geraldine… thanks for stoping by. The laws in the US simply do not enable me to offer specific medical advice or guidance and it must be clear that anything I say is simply for educational purposes and can and should be used as a tool for you to have a more open, informed discussion with your doctor.
I admire a doctor who is willing to treat you as a patient and not treat your MRI finding. Many horizontal tears, especially those with flaps are unstable and hurt. But many tears are what we call grade 2 or small grade 3 tears and they can be very stable. Another issue is your age and whether or not any arthritis is present. IF arthritis is present then caution is advised before considering surgery. Same with people in their 6th decade and beyond. Their knees may not respond well to an arthroscopy.
You should review further with your orthopedist why he/she feels surgery is not in your best interest if your pain persists. It may be because of the presence of arthritis, or something else. You need to know what the decision making factors were.
I hope this helps…
Good luck.
Howard Luks MD
kelly
Dear Doctor,
an oblique undersurface tear is present in the Medial Meniscus body- Meniscus body extruded from the joint by appr. 4mm. Also a small near thickness cartilage fissure is suspected in the medial patellar facet.. Baker’s syst are present.. My doctor didnt explain all this with me. He just wants to do surgery.. is this my only option? does the bakers cyst dissapear??
More important… is there any evidence on X-ray or MRI of degengerative or arthritic changes? How severe are your symptoms? How is your quality of life? How long have you had the pain? Surgery is not the only option. A bakers cyst is simply a collection of fluid in the knee. If you have a source of irritation or inflammation from an injury, arthritis or sometimes a meniscus tear then the knee will become inlfamed, produce fluid… that fluid goes to the back of the knee and produces a cyst. Many many many people have these cysts, and unless they are very large they rarely produce pain and are rarely an issue to be concerned about. Sound like you need a more engaged, open minded second opinion.
Good Luck
Howard Luks MD
Audrey K
Dear Dr. Luks: Thank you for your wonderful information and willingness to answer questions … here are mine: Have you seen cases where an MRI did not show a meniscus tear, but one was found through arthroscopy? I have been having painful meniscus tear symptoms for two months (since experiencing a searing pain in my knee while climbing steps and carrying a backpack) that are affecting me greatly, but according to my MRI, my menisci are intact. Your insights would be greatly appreciated. Thank you!
Yes Audrey… I have had many occasions where an MRI was interpreted as “normal”, yet meniscal symptoms persisted and we went ahead with an arthroscopy and identified a meniscus tear. You can always seek a second opinion on your MRI reading too.
Good Luck
Howard Luks MD
Audrey K
Dr. Luks: Thank you for your quick response and these insights. It had not occurred to me that I could ask for a second opinion on reading the MRI, which makes lots of sense. Again, thank very much!
David S
Dear Dr. Luks:
I am an active 60-year old in good physical condition. About a month ago I awoke one morning to find that my knee was locking and clicking when I tried to straighten it. I had an MRI which showed:
• Grade 2 signal in the posterior horn of the medial meniscus extending horizontally without intercepting either the articular surface or free edge on two consecutive images. Intermediate probability of a meniscal tear and likely degenerative in nature.
• Joint and suprapatellar bursal effusion with thickened suprapatellar plica
• Mild chondomalacia of the patella with posterior marginal spurring
• Mild chondomalacia medial femoral condyle weightbearing aspect but no ligament tear.
I have been doing physical therapy for the past three weeks but the knee is still sometimes painful and I still take stairs one at a time. I also sometimes get clicking when straightening the leg, especially when rising from a chair.
I am due to see my sports doctor next week. He said that he could try prolotherapy injections, which he said sometimes help or, platelet-rich plasma injections which he has used with some success on knee patients.
I would appreciate any advice or observations you could make. Thanks very much.
David
David… Thanks for reaching out. A grade two signal is not a true tear. It will not be visualized at the time of an arthroscopy because it is inside the meniscus itself. It is likely that there is another source of pain. Until a definitive diagnosis is arrived at it’s hard to say what you are treating with a PRP injection or with prolotherapy. Have they tried a cortisone injection first?
Howard Luks MD
Name Gerardine
Hi,
I would like your advice….
While i was kneeling down on both knees, and as i turned/twisted my upper body to the right, i felt intense pain behind my left knee and it was locked in a 90 degree angle with me unable to straigten my leg for 10-20 secs. It feels to me like it was the hamstring ‘snapping over’ and stopping my leg from extending, This is something which i have experienced about three times previously in my life. and in the past, it has only felt a little bruised afterwards but then back to normal, so never needed to consult a doctor. But this time. I have been in a lot of knee pain, it became sore, swollen and pain, particulary on the inside of knee, cap area and inside knee. I am unable to drive, walk up stairs and struggle getting up from sitting down or putting any pressure on it or twisting it for the last 5 weeks… although the pain has reduced somewhat, i am still very limited especially with stairs.
I have had an MRI scan and the doctor describes “some degenerative signal which is perhaps in fact indicative of a horizontal cleavage tear of the posterior horn and body of the medial meniscus. This is not an unstable tear configuration however and it is curious that this should cause such symptons and such severe symptons if indeed it is the cause”. He goes on to say that it is nevertheless the part of the knee that is hurting me and is the only obvious abnormality. I have a history of fibromyalgia and sciatica (which is occassional now) in my other leg, which are completely manageanble and in my mind are unrelated to this knee problem.
He is reluctant to do an anthroscope as he would have to remove a substantial portion of the menisci and is recommending in the first instance to try physio. Though i feel its wise, i don’t really understand how physio will help a tear?
I am confused by your comments above that “If you sustain an injury and you have a very unstable tear, a tear we call a horizontal cleavage tear or a radial tear or a flap tear, those tears tend to remain symptomatic —and if after four, five, six weeks, you still have the same degree of discomfort and quality of life issues, then you might be a good candidate for an arthroscopy.” My doctor says my tear is stable, you suggest these tears are unstable if i have interpreted you correctly? or do these tears come in both stable and unstable?
Thank you in advance for taking the time to read this email.
Best wishes, Gerardine
NameCharles H
I have had pain and discomfort in my left knee for about 7 weeks.I had an MRI on 8/31/12 and this was the diagnosis: LARGE ROOT TEAR,POSTERIOR HORN MEDIAL MENISCUS.POSSIBLE SUBTLE INNER EDGE TEAR,MID BODY LATERAL MENISCUS.CHONDROMALACIA,MEDIAL AND LATERAL COMPARTMENTS.FOCAL TROCHLEAR CHONDROMALACIA.JOINT EFFUSION.SMALL BAKER’S CYST.Do you recommend Arthroscopic Surgery or is Knee Brace Blood stimulation, rest,and Physical Theraphy sufficent to stabilize and correct My condition.At present I can only walk a short period of time without experiencing stiffness and discomfort in my left knee.the pain is dull and occassional.I am not overly active but want to be able to power walk and work out with free weights in the gym eventually.Please advise A/S/A/P. Thank You-Charles H.
Viola
Hello Dr.Howard J. Luks
I am very glad that you are contanting with us.You are doing a great job!!!
I am 31 years old .Suddenly I saw that my knee is swelling and have limited range of motion.After a week I did MRI and the results are here
The axial images reveal a large suprapatellar bursal effusion,but no popliteal fossa cyst, patellar tilt, chondromalacia patellae or discrete femorotibial lesion.
The sagittal images exibit normal anterior and posterior cruciate ligaments.There is however a wedge shaped posterolateral meniscal defect=0.8-0.4cm penetrating the lateral surface consistant with a type 5 tear.There is neither tear nor hyaline degeneration of the anterolateral,anteromedial or posteromedial
menisci.The quadriceps and patellar tendons are intact;the patellofemoral space is preserved.
The coronal images confirm the posterolateral meniscal tear and mild lateral collateral ligament sprain but no medial collateral ligament sprain,iliotibial tract injury,cartilaginous atrophy or osteophytosis.
Impression: Type 5 posterolateral meniscal tear,lateral collateral ligament sprain and suprapatellar bursal effusion.
Can you give me some advice?It is 10 days that I am in this condition.Do I need to do surgery?or take some medicine?And can I put ice after 10 days?Please,give me some advice.
Thanks a lot.
Thanks for stopping by… nothing wrong with the use of ice and or moist heat at this point to improve your pain, and swelling. A defect in the meniscus implies a loose piece… those types of tears tend to remain bothersome. Is surgery the answer? You will ultimately make that determination. It is primarily a quality of life decision.
Good Luck
Howard Luks MD
Hawthorne NY
Kerron
Dear Dr Luks,
I am touched deeply by this majestic work of yours to offer the invaluable guidance to many of the sufferers like me. I could see an answer from you to almost every question asked here on the site. I feel myself fortunate to find this site.
I am Kerron, 33, Male. Six months ago, my knee got hurt while climbing a rock. I immediately went to an orthopedic surgeon and was given six months of medication (painkiller, anti-inflammatory and vitamins) saying it could be a simple muscle injury or a small tear which doesn’t necessarily need a surgery. So being unaware of the fact, I use to run, jump, exercise and lead my routine life during the medication. The knee use to pain a little, lock, pop sometimes during the period. 4 months after medication when the pain wasn’t subsiding, I went again and the Dr. referred me for a MRI scan. Below is the MRI report finding. Now the doctor is insisting for an immediate knee arthroscopy. Otherwise the tear can worsen more complex and injure other parts of the knee, he says.
MRI Finding:
Tibiofemoral, patllofemoral, and proximal tibiofibular joint alignment is normal. Bone marrow is normal in signal intensity. Anterior and posterior cruciate ligaments are normal.
Oblique horizontal high signal is seen in posterior horn of medial meniscus extending in to body region and to inferior articular and meniscocaspular surface. Branching high signals are seen from this parent signal in central zone extending to superior and inferior articular surface. 11.3 mms size multiseptate cyst is seen adjacent to it on poeteromedial aspect.
Anterior horn is normal. Lateral meniscus is normal. Root ligaments are normal. Medial and lateral collateral ligament complexes are intact. Patella and patellar retinaculi are normal. Quadriceps and patellar tendons are intact. No ljoint effusion. Muscles and tendons appear normal. Subcutaneous tissue is normal.
Conclusion:
Grade 3 complex tear of posterior horn of meniscus with small parameniscal cyst.
It will be of a great help to me if you could guide me on the below queries of my knee condition.
1. Can the tear heal up on its own?
Looking at the MRI, is there any slight chance that I can avoid the arthroscopy and the tear will heal up on its own with some medication, massage, precautions, physiotherapy or any other mean? As I am still in a younger age, healthy and physically fit (5.8’, 70 kg). The knee doesn’t pain much; locks slightly sometimes, feel some stiffness when I perform heavy activities for a longer period. But am fearing of worsening the knee further and becoming it more complex later on if delayed the surgery. I have stopped all heavy activities currently.
2. Can arthroscopic repair possible in this case?
If at all the arthroscopy is the only solution looking at a long term effects of the injury and quality of future life, then out of the three options (repair/partial removal/complete removal), can the knee be cured by arthroscopic repair only without removing the part of meniscus (MRI reference).
3. Post surgery effects.
I read many of the question answers above and found that many people complain of pain arising again after the surgery and require additional surgeries. That worries me lot about going with the surgery and the post surgery life. Will the knee be back to normal completely or there will be lifelong pain/precautions/physical restrictions after surgery with regard to the quality of life?
Please guide as I will be waiting only till your reply before deciding on going for the surgery.
Thanks,
Kerron.
Kerron… Thank you for your kind comments.
Certain tears can heal on their own… typically a complex tear will not. But keep in mind that not all meniscus tears hurt. So there are many people who “recover” and lead an active lifestyle with their meniscus tears.
Repairs are possible with some tears… and not likely to succeed with others. You need to find an orthopedist who performs a number of repairs and have a nice long discussion with them while they are viewing your study.
Arthroscopy for a meniscus tear remains a viable solution, if you feel that your quality of life is affected and limited by the discomfort you are having. If the piece is removed, the knee will never be completley ” normal” but many people return to a very active, productive and satisfied lifestyle after recovering from meniscus surgery. Some people will go on to develop osteoarthrtis… some may not. If you do, then surgery might be indicated in the future to deal with that. But a tear alone can cause arthritis, the surgery should be considered to improve your quality of life, not simply because you have a meniscus tear.
Good Luck
Howard Luks MD
Hawthorne NY
Kerron
Dear Dr. Lukes,
Sorry for the delay in response from my side. I in fact wanted to check out with few therapies whether they serve any useful to my knee. But no significant improvement as off now, so it’s become further tricky how much time I should spend just waiting it to heal it. In the mean time, my search for an orthopedist who can try go for repair through ‘suture’ only is ON. So soon I am going to get it operated rather risking it further. Its nine months already since the injury occurred. Its quite certain that it keeps on damaging the cartilage (micro- trauma) even after being cautious, but I fear if it can harm the ligaments as well during this period when left unoperated. Any suggetion?
Want to thank you again for your kind suggestions and my best wishes for the inspiring work!
Thanks,
Kerron
Thanks Kerron… Good luck to you!
Howard Luks
Name Joe Fink
Hi Dr. Luks:
I was just diagnosed with a complex tear in my right knee involving the posterior horn and body of the medial meniscus. There is a probable displaced meniscal fragment present which is situated just medial to the PCL.
This doesn’t sound great to me, but my pain has subsided (maybe due to the advil), but based on the above diagnosis, does it sound like surgery is inevitable?
Thanks in advance.
Joe
NameCHARLES H
Hi Dr. Luks I had an MRI on 8/31/12. the Diagnosis was large root tear,posterior horn medial meniscus.possible subtle inner edge tear mid body lateral meniscus. chondromalacia,medial and lateral compartments. focal trochlear chondromalacia.joint effusion.small baker’s cyst. I am 63 and have had this condition for about 8 weeks,it started when i heard a popping sound behind my left knee while accelerating my walk to cross the street. I have mild pain with taking naproxen sodium 2-3 times a week and icing my knee daily. will exercise such as elliptical machine and gentle walking in the pool stabilize and eleviate my condition or will sugery be neccessary to improve it?At the moment I cannot walk for more then 10 minutes or so on solid ground without my knee feeling stiff or achy.I wish to be ablet to power walk and work out in the gym eventually.I am not overly athletic. Than You for Your Attention to My Situation Charlie
Charles… root tears of a meniscus are a challenge. Many can be fixed, some can not. Some patients will choose to have surgery (it is a quality of life decision), some will not. The chondromalacia implies the presence of arthritis in your joint as well. Typically, joints with both meniscus tears and arthritis do not respond as well to meniscus surgery. But not having seen you or your studies, and without a clear understanding of your complaints I simply can not offer an concrete advice. Just general knowledge.
Howard Luks MD
Jaromir
Dr. Luks,
This is really great website.
I am 57, tennis player. Last year spring my RIGHT knee and upper calf suddenly got swollen. I didn’t experience any pain, really, it was more reduced mobility because of the swelling. I thought it might be an inflammation, tendons, but as it progressed I went see an orthopedist. His diagnosis was immediately a medial meniscus tear. I decided to wait, I limited tennis a little, but at the end of the summer I got MRI and underwent an arthroscopy. He found a little bit of arthritis on the cartilage as well. As I was recovering well this year, limiting tennis to a doubles or max of 2 sets of singles at the time and I did therapy and biking, last month, playing tennis, I felt the slipping motion (horizontally) in my LEFT knee while I was slowing down approaching the net. I suspended tennis since, did some hiking with the knee brace (lately). Last week I’ve seen an orthopedist, got another MRI and the result diagnosis is “flap tear” in medial meniscus. Knee is hurting mainly in the night, not when I am walking, and it hurts when I try carefully a few steps of running and it is not swollen. After my last year experience and after reading your web page I incline not to wait and let the flap to be removed to avoid further pain and possible damage. Plus – I cannot run.
So my question is: would it be a good decision to go for the surgery?
Thank you so much for your time.
Jaromir
Lindsay
Dear Dr Luks,
Thank you so much for sharing your expertise and wisdom on this site. I appreciate the forum so much. My issue is that I was a sedentary person for quite some time, and recently within 6 months or so, took up exercise. Little by little, soreness built up in the left knee, and acute pain with squatting down or rising up from sitting. Still, I overlooked it in my quest to get healthy (prediabetic) tried to work through it, until the pain became unbelievable. Its hard to say when the injury started. Now, I cant really safely exercise, I hear popping and cracking in the knee when squatting and standing, even when sitting, I feel the knee has become unstable. Pain seems to pop up on all sides of the knee. In addition, my quads shake sometimes when I try to walk downstairs, or after even mild swimming. Heat and ice seem to help.
My primary doc says its runners knee, but it hasnt improved since I stopped running and switched to swimming instead. It seems I have sustained a real injury. Im due to start physical therapy in a week but I was wondering if I need to get a MRI to see if there is anything more serious? Especially since it just wont heal, and the pain comes back, and then fades, and then comes back again. Its frustrating that it just wont heal. Im 29, 5’5, 178 lbs. I feel weird painful “twinges” on the kneecap.
What does this sound like to you>??? IS there anything else besides PT I should consider at this point? Thank you so much for help! Im so clueless about this stuff….
Lindsay
Dear Dr. Luks,
I also thank you for the generosity of expertise shared here on this site. I never paid much attention to my knees..until now, that they are injured. I was told by a Dr that I have “runners knee” from exercise. My problem is that it hasnt healed in a month, it seems like its worse since I stopped exercising. There seems to be alot of clicking especially when squatting down, standing, shifting in my seat and pain when its extended or when sitting for long periods. It seems like it is connected to issues of tightness in the glutes/alignment.
Im frustrated at a lack of healing,improvement)(1 month and no change/( I feel Im permanently damaged!) as well as legit fears of doing MORE damage, as the knee feels more unstable now than it ever has in my life. Can I be doing damage to cartilage? I am scheduled to start PT in a week, but Im worried there is more that should be done… (such as MRI) Im 29, slightly overweight, female, just recently made a a strong effort to exercise again (to lose weight) and this injury occured…Can a physical therapist determine if I have lost cartliage? I know its alot of questions, but my primary doc really seemed like she didnt know what was going to happen/ what to expect going forward….
Any insight would be so so greatly appreciated. I have never spent so much time worrying about my knees until now..amazing what we take for granted…
Eric O.
Dr. Luks,
What is the percentage of misdiagnosis with partial vs. complete tears of the medial mensicus? While I have reviewed the results with my orthopedic surgeon ‘undersurface longitudinal tear defect at the posterior horn of the medial meniscus extending to the posterior body horn junction’, his conclusion was basically that ‘we’re not going to know until we’re in the joint itself’.
If my lateral meniscus is identified as ‘unremarkable’, given your expertise, what exactly does that mean?
My main question is if the tear is removed, the meniscus becomes smaller, therefore, what exactly does this buy me? A possible pain free or less of a pain in my right knee with the potential for continual tearing and or complete tearing at some point in time. These days, it is quite common to receive a ‘surgery is needed, but only if you want to’ response.
I do understand that it’s a quality of life question, one in which I will be answering soon.
If you have a moment, please respond.
This is a great website, many thanks!!
Eric O.
Graham
Dr. Luks-
I have a question for you.
I am a 42 yo male with a ‘large’ (MRI wording) bucket handle tear of my right medial meniscus that has flipped laterally and now resides on along the edge of the intracondylar notch.
My initial injury was 18 months ago. Since then I modified activity and worked with a PT and trainer to strengthen the muscles around the knee. I would have an episode of the knee locking every 6 weeks or so but the locking would only last for a few minutes before I regained full movement. Six weeks ago the knee locked and I have not since regained full ROM in flexion and extension. The surgeon believes this is because the bucket handle is impinging that movement.
According to the surgeon removing the handle is the only option. He also believes this should be done soon in that the displaced handle could cause damage if left there for a long period of time.
My PT believes that he can achieve 100% recover and that the bucket handle will simply ‘dissolve’ over time and I will regain full ROM.
My question is this: can a bucket handle ‘dissolve’? It seems to me that this is highly unlikely/impossible and my case is one where surgery is, intact, the best option.
thank you for your thoughts.
Graham
Graham
Dr. Luks-
Thanks for the great website!
I have a quick question. I am a 42 year old male a ‘large’ bucket handle tear on my right medial meniscus. I have been managing the tear for 3 years by moderating activity. However, about 6 weeks ago the handle flipped laterally and took up residence on the edge of the intracondylar notch. When this happened, I experienced intense pain and extremely limited ROM.
For the past six weeks, I have been working with a PT and I am now (mostly) pain free. My concern is that I still do not have complete ROM due to the displaced portion of the meniscus.
My surgeon has indicated that the only way to solve this problem is to remove a piece of the meniscus. He also stated that he did not want to wait ‘too long’ b/c the displaced piece of meniscus could be damaging other parts of the joint. My PT has told me that he believes the meniscus will ‘dissolve’ on its own and I will regain full ROM again.
Have you ever heard of a meniscus flap ‘dissolving’?
Thank you!
Graham
PW
I am 51 year old female 5’3, 200 lbs. occasional stiffness in knee after walking, but short term anti inflammatory med helps. Saw orthopedic doctor because of swelling and couldn’t bend or straighten leg after walking. He didn’t think anything was torn from the physical examination, but ordered an MRI because I was limping. A week after the initial sprain, I tried walking, but felt a strong snap and knee gave out. MRI on Aug 15 showed large joint effusion, degeneration and tear of posterior horn medial meniscus root with mild meniscus extrusion, probable osteochondral bodies posteriorly within joint, severe degenerative changes of patella femoral joint, and mild grade 1 sprain of the medial collateral ligament. Doctor said…I can do nothing or see surgeon which is not available til next month….so I tried 500 mg naproxen for 30 days…didn’t help swelling and now have switched to meloxicam 15 mg. for past 2 days…
also RICE…How much time should I give these anti inflammatory medications?
Do you think the inflammation is from the debris or the tear, or both?
I think the tear is recent. This might require surgery?
Your reply is greatly appreciated.
In a knee displaying arthritic or degenerative changes, you want to try all measures possible to improve your pain and swelling prior to considering surgery. Arthroscopy is a great aletrnative when no arthritis is present… but the results become more unpredicatbale when arthritis is present because arthrorscopy can not treat the arthritis. Most heat, ice, NSAIDS (mobic, advil etc {risks included ulcer, high blood pressure, heart problems and kidney disease) can improve symptoms… as can Tart Cherry Juice (yes you read that correctly :-)). If these modalities do not improve your swelling and pain please consult your surgeon for other alternatives…
Good Luck
Howard Luks
Jayne
Hi Dr. Luks,
Your sports medicine information and perspective is amazing! And, your website is so incredibly useful. I’ve never seen anything so clear and well-designed/lay person-friendly.
Well, if you don’t mind, here’s my story:
1) Among other things, I’m a 61 year-old Zumba (dance-fitness) & Aqua-Zumba instructor. (As a dancer, I have well-developed quads & strength, but I admit to a slightly tight hamstring imbalance). My meniscus injury occurred while I was teaching a Zumba class outdoors (my shoe grabbed the rough concrete surface while I was turning to the outside with knee slightly bent. Pop! Ouch! !@$!!! This was about 10 days ago.
2) Two days later, Orthopedist ordered MRI & also gave me a lidocaine/corticosteroid shot for pain. Relevant results: ”complex tear with a dominant radial component involving the posterior horn of the medial meniscus without extrusion.”
3) Since I’ve already had a severed & surgically-repaired ACL years ago (other leg, fortunately), besides RICE-ing , I immediately started wearing my industrial-strength/heavy-duty Rx metal-hinged brace after this injury. That’s helped keep things stable laterally. 10 days out, pain is somewhat better, but not great. I can’t walk without limping, though, even with brace, and find weight-bearing a problem. A few times at night in bed (when I’m on my side, but not wearing my brace), my knee has locked up in a horrible position that creates stars-in-my-eyes pain. I have to manually adjust my knee out of that position. (So, I have decided just to wear by brace 24/7).
4) BIG ISSUE: I have Lupus. As I’m sure you know, surgical procedures can cause major & life-threatening problems for people with Lupus. I had a severe response (to anesthesia?) in the recovery room when I had one of my shoulders done about 10 years ago. Ended up with heart complications. So, surgery for me needs to be 100% unavoidable to be worth the risk. I’m also in a a rather lengthly flare, even though taking Plaquenil (which makes me nauseous or worse).
5) My orthopedist recommends I think about my options carefully, but says typically surgery (in a case like mine would be recommended to repair to the injury). He cannot really offer guidance on my Lupus issues.
Hmmm… I can’t teach like this, nor can I really live like this easily (2-story house, etc etc). BUT…
Lupus makes me look at things differently. I don’t think surgery is a good option (at least right *now*) because of my Lupus, current flare & prior history of adverse response to surgery. Still, I don’t want to exacerbate the injury, but (even without Lupus to worry about) given the type & location of the tear it seems that surgery might be less effective at my age or not heal as well as if I were younger. Makes me question the benefit.
So, here are some questions: If I try to re-hab the knee with PT… how long should I spend trying PT to achieve some results? (I’m a highly-motivated patient who does her exercises). Essentially what I am asking is about how long should I invest in PT before seeing whether it’s really doing anything… or not? Could this type of injury resolve on its own? If surgery eventually seems like the only real option, can they do it using an epidural? Do you have any comments relative to my Lupus concerns?
Thank you so much! I can’t tell you how thankful I am for your concern, experience and knowledge!
— Jayne
Jayne… I appreciate you visiting my site and very glad you found the information useful! Yes.. Lupus complicates the issues signfiicantly. If a meniscus tear, and the resultant pain is going to simmer down and resolve on its own it may take a number of weeks —sometimes 6-8 weeks, before you start to feel better. It sounds like you are going everything right. Continue ice/moist heat, range of motion and perhaps PT…. ( NOT medical adivce — I really have to say that :-( – sorry). Check back with us in few weeks if your symptoms persist.
HJL
Jayne
Thanks, Doc! I sincerely appreciate your comments & affirmation. I’ll do my best to behave (pain is a great motivator for good behavior & surgical avoidance is another!) and follow your suggestions. I’m fortunate to teach aquatic fitness classes in an aquatic/physical therapy facility with exceptional & gifted/experienced PT professionals (who are also caring friends). I can’t help but be consistent about doing my exercises regularly/properly/responsibly with them hovering around. :-)
Thank you for the estimated time frame for some self-healing improvement. That really helps me have a realistic perspective.
Your website is a treasure trove of good stuff! Your approach to caring for patients is elegant. Thank you for all you give of yourself to so many of us whom you will probably never even meet. No, this isn’t medical advice, rather very compassionate information, words of wisdom & experience. :-)
I’ll check back in a few weeks. In the meantime… thank you again.
Jayne
Thank you !
Doug
Dr. Luks I am 63 yr active guy (run two 1/2 marathons a year and teach skiing full time). I was diagnosed with a complex tear per MRI and have had a couple of consultations. I am presently asymptomatic and have been running and walking up to 8 miles. I have run a couple of three milers , but I can’t seem to get past that mark w/o pain setting in. I am scheduled for surgery on the 24th next Friday and was told that if i wanted to keep the distance running i needed the menistectomy…I am signed up for a 1/2 marathon last weekend in September. Long trail hike (100 miles in Oct). I am assuming that my age and activities point to a degenerative tear and was told that it could go away on its own. My instincts are telling me to postpone and try to keep training, and maybe have another conversation with my surgeon. I ski at a very high level and really don’t want to risk anything there. So, after all that ramble; what are your thoughts and is there a diplomatic protocol for sharing my apprehensions with my surgeon.
Thanks this is a great site.
Tough call Doug…. If there is a small flap that is bothering you within the degenerative tear, then you may feel fine… BUT, if there are any arthritic changes present, chances are you will not feel better. When both arthritis and tears are present, we as surgeons need to be very very careful who we indicate for surgery. They should have buckling, instability and giving way… or mechanical symptoms. Treating pain that occurs a few miles into a run may or may not be only related to the meniscus ??? I obviously can’t tell being that we have never spoken, nor have I seen your images.
Good luck with your decision making…
Howard Luks
GY Kim
Hello,
I saw a doctor, I took MRI and doctor wanted me to take surgery.
MRI reading says:
– Meniscus : grade 3 signal intensity, contour change and parameniscal cyst on lateral meniscus anterior, posterior horn&body. No abnormal contour or abnormal signal intensity on medial meniscus.
…and everything else is normal.
I wonder if I really need arthroscopic surgery because my doctor said he will cut out the part where meniscus is torn and it’s not possible to recover in my case. And he says after cutting off the meniscus, the remaining part will be small and will wear out fast. He recommended meniscus allo-transplantation after 6 months of the arthroscopic surgery!
But Is it really necessary if I only have clicking and popping, not much pain? Actually, I only feel pain like when I walk a lot with hills..etc. and I feel pain INSIDE the knee ( not outside..where the meniscus is torn). It hurts like i have bruise under the skin.. I guess it’s from the cyst???
I have pain when I turn my knee outwards, but If i don’t intend it, it’s fine. It just has popping and clicking when moving..normal walking, going up and down the stairs are fine.
What I worry is I still have popping and clicking on my knee..Does it mean that I have loosing body to remove??? Or Could it mean that the flags can act like a sand paper to bones or the flags might progress the injury ????
And How are the out-turns of meniscus allotransplantation so far??
Thanks in advance,
From Korea
GY
Jeff
Hi Dr. Luks
Thanks for the great information.
I am a veteran and was diagnosed by he VA as having a ” complex tear with a dominant radial component at the junction of the body and posterior horn in addition there is a horizontal component in the posterior horn that extends to superior articular surface” I would like to know if physical therapy is an option? I dread the thought of surgery.
Any thoughts would be greatly appreciated
Bobby
Hi doctor,
If possible I’d like to ask you some things about my meniscus injury.
I landed awkwardly coming down from jumping in football and immediately felt pain. A couple weeks later I had a MRI that said I have a 1 cm tear in my lateral meniscus and a microfracture in my femoral chondral i believe. I am schedule for surgery next week, but with football coming soon, i am afraid i will miss most the season. I feel as if i can play on my knee. I did so 3 days after the injury without knowing its severity. I personally have been doing some research and from what I have read, with a tear that size, i should not be able to do the things i can still do. My knee does not buckle, lock or feel as if it is going to give out. I would say its about a 4 on the paiin level not doing anything, and a 7 when i run or jump. The only issue i have personally is the swelling, which makes it stiff and not as flexible. The pain i can deal with. I am just wondering what you think? Could the MRI or doctors mistaken the size of the tear? How long is the usual recovery time if i do opt for surgery? And with a brace (which makes it feel much better) could I play football as long as I can deal with the pain? I feel as if i could, but would like your input on the whole matter?
Bobby… some of these tears.. especially lateral meniscus tears can heal on their own. That process can take 6-8 weeks. Pre-season injuries always present us (and you) with difficult decisions to make. If you have a repair, where the tear is sutured you will be out for the season. At your age a repair is much preferred over an excision or removal of the piece. If you’re going to wait to see if it heals on its own that time frame can be 6-8 weeks.
Hope this helps.
Good luck
Howard Luks
Bobby
Thanks Doctor!
I tore it 5 weeks from yesterday, I woke up this morning and feel little to no pain and about 85% motion wise. They said the surgery will not be a repair. My season doesnt start for 2 1/2 more weeks so maybe i can talk to my doctor to see what he thinks. But you are saying that even a 1 cm tear could heal on its own? I know since this is over the internet I should take all this with a grain of salt, but I have kind of been disregarded from all my own medical decisions so far, and my surgery is something I want to have a say in if possible.
Thank You, Bobby
Carlos Diaz
Dr. Luks!
This truly is a great forum, I am so happy to have found this site.
I landed akwardly on my right foot and my knee buckled. It felt as though the top part of my leg hyper-extended over shin and foot, I herd no crack or pop but felt as though my knee cap slid down. I fell to the ground immediatley and experienced mild pain. After a minute, of painless stretching, I stood up and was able to limp around. After five minutes I was able to walk normally and bear weight on the afflicted knee. After an hour, I was able to hop around and most of the pain had subsided. Currently, 19 hours later my knee is not swollen and I feel only slight discomfort in my right knee. I can walk normally. Getting up from chairs, straightening my leg and going up stairs are not a problem. My knee feels weak and when I lock my knee it feels as though it might buckle again. I am guessing this is just a sprain, then again I am an overly optomistic individual. Is there any advice you can give me?
Sorry Carlos… I’m not going to be much help here. Too little information and I can’t examine you :-) ! Give it a few days and if your instability symptoms persist I would let someone examine you.
Howard
Ahmad
Dear Dr. Luks,
I found your website and various answers highly informative.
About 4 months ago I started feeling pain in the back of my right knee. I could not link it to a specific event but I play tennis and at the age of 49 anything could have caused a tear. I had an MRI done and the findings were:
– Horizontal line of hyperintensity in posterior horn of medial meniscus, connected to a vertical defect of the inner tip
– mild joint effusion
– normal ACL, PCL, MCL, LCL, quadriceps and patellar tendons
– normal bone marrow signal intensity and appearance
– no intra articular loose body
– findings suggestive of horizontal tear of posteror horn of medial meniscus, connected to a radial defect
– mild inflammatory reaction
Since the MRI I’ve limited my exercising to swimming. I feel only limited pain when I walk slowly and straight but I certainly feel increased pain when I walk a lot or when my leg is twisted slightly (or if my leg is fully stretched). I’ve tried walking with a knee brace but it does not seem to help. The pain does not seem to be reducing with time.
In your view is surgery unavoidable based on the above? would it be wiser to wait some time and see if the pain will reduce? I’m concerned though that, with the consistent, even slightly increasing pain, delaying surgery could risk more significant consequences if I were to fall or twist my leg leading to a more severe tear.
thanks in advance.
Ahmad… at 4 months you have a good idea of what your knee is going to be like going forward. Most healing takes place in the first 6-8 weeks. The decision to have surgery is based on your quality of life. It is ultimately your decision to make. You need to take into account your pain, current limitations, etc and figure out if that is acceptable or not to you.
Good Luck!
Howard Luks
Name Angie
Hi Dr. Luks,
I am 37 years old and was diagnosed with a horizontal meniscus tear, (degenerative tear) with a meniscal cyst. I had the tear for a few years and decided it was time to get the surgery because it would hurt when I was at work standing on my feet for a few hours at a time or if I went walking for a mile or played tennis. The MRI did not show any arthrits. The doctor told me that it would be 3-6 weeks recovery. So, I had the surgery 10 weeks ago. I was on crutches for 4 weeks and I am still walking with a little limp. The doctor said that I had grade 4 arthritis under my kneecap. He also said I had a very bad tear and a big cyst that he drained. He trimmed the bad meniscus away. Now, after surgery, it’s been 10 weeks and I’m feeling more pain than I had before the surgery. Now, it hurts to walk up the stairs and down the stairs. When I walk around for a little bit, I feel pain behind my knee. The tendon behind my knee makes a cracking noise sometimes when I walk. The physical therapist said I’ll have a hard time going up and down the stairs because I have very bad arthritis. He also said it may take 6 months or so to get my quad muscles strong enough so I won’t feel the pain as much, but I will still feel it. My concern is that I did not have any pain going up and down the stairs before surgery and now I’m feeling worse pain.The top of my knee where the knee cap is also hurts when I extend my knee Does this sound right to you because I didn’t feel any of this kind of pain before? The only kind of pain I felt before was when my knee felt like a sharp pain and I couldn’t bend or straighten it and that was only when I was standing on my feet for a couple hours at a time or walking for about a mile or playing tennis. Thank you so much for taking the time to answer my concerns.
Angie… Many possibilities. I would consider a second opinion and perhaps a second MRI. Issues such as “post-menisectomy osteonecrosis” or bone marrow edema, stress fractures and residual tears can all lead to symptoms like this. It’s time to work it up….
Good luck
Howard Luks
Shah
Hi,
Sorry for disturbing! But reading your post and knowledge i got some courage, as i am feeling quite low and also confused.
Brief History:
Once while playing football in school (8-10 years ago) , somehow injured, knee injury couldnt move or walk, i was taken to doctor, advised rest, some tablets and got better!
BUT, once in a while my knee( or leg) used to get lock and not opening beyond 80 percent (approx) , two days rest and i was able to walk and 100 percent opening..
Somehow i discovered a technique of twisting or touching few spots at bottom (sole) of my leg ( i mean below the leg where you touch u feel laughter… ) and it used to get good immediately, unless severe (which used to happen once in 2-3 years)
i had done X ray and medical check up, i was suggested rest and build muscle fitness of that leg. and got recovered.
PRESENT TIME
I was changing clothes a week back, i kicked them, and got something pulled or went wrong… went to doc, took some medicine but leg wasnt opening for 2-3 days… and then it opened.. but this new doctor asked for MRI scan.
I did that.
it says “probable tear in posterior horn of lateral meniscus”
My doctor suggested to meet some expert of Arthroscopy.
Thus have booked a appointment on Monday, but was real confused, but atleast reading your post gave me some knowledge… but i cant get this as because after that injury years ago, i have plauyed football, learnt swimming, climb moutains and waterfalls…. so just puzzled… .
Rachael
Hello, Dr. Luks. Thank you for this informative post, and for providing a message board for inquiries.
I had an acute medial meniscus tear (flap) 2.5 weeks ago. I caught myself before falling after slipping by “braking” with my knees – my right knee was slightly bent and twisted to the right. Immediate pain. I did RICE that evening and the next morning. I was unable to fully extend or fully bend the knee and there was significant pain when I did any side extension. I went to the hospital the morning after the accident. I live in South Korea and all of my treatment has been done by an orthopedic surgeon here. I also had a consult with a PT. At the initial hospital visit, I had x-rays and was fitted with a full-leg splint. I did RICE for 3 days, and had an MRI. Four days after the accident, I had a follow-up appointment with the orthopedic surgeon, who determined, based on the MRI, that it was non-surgical. For treatment, I have a full-leg hard cast for 4 weeks. Then I’ll get a brace. The doctor wanted the cast to stay on for 6 weeks, but I’m leaving Korea at the beginning of August.
I’ll be in the U.S. for 4-6 weeks starting the second week of August. My PT friend (who lives here) is going to determine an exercise plan after the cast comes off, but I have a few questions that I hope you can help me with. My Korean language ability is fair, but it doesn’t extend this far.
First, some general information about me: 29 years old. 5’6”, 125lbs. Very active/fit. Daily intermediate-level yoga practice, swim, hike/trek, run, mountain climb/bouldering, etc. No previous injuries. (However, I did have a minor motorcycle accident about 3 months ago and banged up the same knee, but swelling and pain was at the front, rather than side. Pain and swelling went away in about 2 weeks with RICE.)
Okay, questions! Thank you!
1. According to North American practice, is it rare to cast a non-surgical case? Korea tends to be a bit cast-happy. I understand that the knee should be immobilized, but I’m a bit concerned that I’m not able to ice or compress the knee (and haven’t since 4 days after the injury). In your opinion, is there any risk of additional damage with this treatment?
2. What should absolutely be avoided in the first week or two after the cast comes off? First month? (I was planning on trekking through the Indian Himalaya and the Annapurna Circuit after leaving Korea when this happened. I realize that probably won’t happen for probably a few months now, but a gal can hope…)
3. What indicators of the healing process can I be aware of when I’m in the brace? How can I tell when the knee is strong enough to go without it?
4. Less than a week after the cast is removed, I’ll be on a 10-hour flight from Seoul to Seattle. Is there anything I should keep in mind while I travel? I’ll have the brace then. Should I wrap the knee? I assigned myself a seat on the left side of the plane so that my leg can stretch out in the aisle, if needed.
5. Is there anything else you can recommend, as far as follow-up treatment?
Thank you very much for your help! It is greatly appreciated!
Hmmm…
There are big differences in terms of how we manage certain injuries. I’m not sure what the MRI shows? Without that I really can’t comment further… sorry. You should be concerned about blood clots or a deep vein thrombosis..escpecially if you take birth control pills or smoke and should review this with your doctor.
HJL
Rachael
Hello, Dr. Luks.
Thank you for this informative post on meniscus tears. My apologies if you have covered my area of concern in previous comments — I skimmed earlier comments, but did not fully read all.
I am currently living in South Korea. I had an acute medial meniscus tear (flap) 3.5 weeks ago. I stopped myself from falling by “braking” my knees — dumb, I know! — my right knee was slightly bent and twisted to the right. Significant pain. Immediately afterwards, I elevated my knee and iced it throughout the night and early morning. I went to the hospital the morning after the accident. (I could not fully extend or fully bend the knee, and certain side movements were very painful.) They did x-rays and put me in a full-length splint. I did RICE for the next three days (during this time, I saw my friend here who is a PT and had an MRI at the hospital). Fourth day post-accident, the orthopedic surgeon at the hospital discussed the diagnosis — surgery was not necessary — but to immobilize the knee, I’m in a full hard cast (foot to upper thigh) for a total of 4 weeks. He originally wanted the cast on for 6 weeks, but I’m leaving South Korea at the beginning of August, so will get a brace when the cast comes off. Korea tends to be cast-happy, and while I do realize it’s necessary for the knee to be immobilized, I’m also concerned that I’m not able to ice or compress the knee during this time. I am, as to be expected, still experiencing some pain — with subtle increases/decreases throughout the day. I elevate as often as possible, and use crutches 99.9% of the time.
I will be in the United States for 4-6 weeks starting the beginning of August, with the brace, and a PT treatment plan from my friend who is here in Korea. My questions for you are:
1. As far as North American practice is concerned, it is rare to cast the leg for a non-surgical case?
2. Are there any risks involved with casting the leg, and not being able to ice or compress so soon after the accident?
3. Are there any indicators (pain, mobility, etc) that I can be aware of when I’m using the brace, to determine when I can stop using it?
4. Less than a week after the cast is removed, I have a 10 hour flight from Seoul to Seattle — is there anything I should be mindful of when flying/sitting for so long?
5. Is there anything else I can do to aid the healing process? Or to watch out for, given my case/treatment?
6. What should I avoid the first week or two after the cast is removed?
Some general information about my current health: I am very active and fit: 29 years old. 5’6″, 125lbs. Daily intermediate yoga practice, run, hike/trek, mountain climb, swim, etc. No previous injuries. (Although I had a minor motorcycle accident and banged up the same knee — though on the front of the knee cap — about 3 months ago. Pain and swelling subsided in 2-3 weeks with RICE.)
Thank you so much for your help and feedback. It is much appreciated!!
James
Hello Doctor,
These are the findings of my MRI ( I have not seen an Ortho yet….insurance dragging feet).
Findings:
MEDIAL COMPARTMENT: A Horizontally oriented tear in the posterior horn of the Medial meniscus is present. Also, inner edge tearing is present. No meniscal fragment displacement is present. Small partial-thickness cartilaginous defects of the medial femoral condyle are present. The collateral ligament is mildly thickened.
LATERAL COMPARTMENT: The lateral meniscus is intact. No cartilaginous defect is present. The lateral collateral ligament complex is intact.
INTERCONDYLAR NOTCH: Mild intrasubstance degenerative changes are present in the anterior cruciate ligament. This ligament is otherwise intact. The PCL is intact.
PATELLOFEMORAL COMPARTMENT: Mild medial facet cartilaginous softening present. No cartilaginous defect is present. The patellar and quadricepts tendons are intact.
MISCELLANEOUS: Small fluid is present in the joint space. No bone marrow edema is present.
IMPRESSION:
1. Tearing of the posterior horn of the medial meniscus. No meniscal fragment displacement.
2. Small medial femoral condyle partial-thickness cartilaginous defects.
3. Mild intrasubstance degenerative changes of the anterior cruciate ligament. This ligament is otherwise intact.
4. MCL ligament scarring.
END
I am 29 years old and have a very physical job that requires I get back to optimal shape to keep working.
Im not overweight and have no back problems.
The swelling from the initial time of injury is gone but I still get popping in my knee and it feels weak compared to how it once was.
So I guess my question is. Do I fall in the category of possible surgery to get back to working shape?
Thanks to any responders.
~James
OK… now I see this :-)
In the US… we do not cast meniscus tears. We tend to mobilize the knee since our cartilage is fed by the fluid in the knee and thus the more the knee moves, the better it is for the overall health of the cartilage.
Howard Luks
Name Larry
Hello Dr Luks
Last Wed i was Playing a softball game. Triped as i was picking up a ground ball from 3rd. The knee poped but I got back up. Hurt some but i stilled played on. Was batting and started to run to first, got half way there and my knee gave out, left like it was being pulled out of the socket. Went to the er at that time. Swelling was small then but was showing. x rays taken. No bones broken. Was told to keep ice on it, take inflammatories and was put in a brace to keep knee from bending.
Then was told if it didnt get better in a week or two, that i would need to see a orthopedic DR. and have it exam and or MRI. It is 7 days later. Swelling is still there. A knot like feel is just above the knee cap and to the outside of left knee. I am able to put some weight on it. But it still pops and feels that it is going to fall off when the tibia is pulled or pushed forward. I do have better movement in the knee now than before. Pain when leg is full out on inside of knee, feels better in a sitting position now. Do you think that I have a meniscus issue and not a mcl or acl issue. I do want to play again if possible. I am 52 male, Healthy . My mine is young but i guess my body is saying something else.
Can you comment
Cassidy
Hi. So I have a question! This happened like a month ago while jumping into the shallow end of a pool and landed with a bent knee and I’m pretty sure it twisted a little. I felt a really sharp pain for like 5 minutes but then I walked it out and it felt better. Every once in a while I make sudden movements with my leg rotating it to the side and it locks up. I try to straighten it but the pain is unbelievably painful. I get it straightened, it pops and it stops hurting a lot but it would still be unstable to walk. Im not sure if its torn. But I needed to ask what you thought. Any ideas on what it could be?
Cassidy,
Unfortunately is sounds like you have a flap tear or something we refer to as a bucket handle tear of the meniscus. These tend to be the more common causes of these symptoms… but without an exam, X-rays, etc … this is just for information purposes.
Good luck.
Sushil Puri
I am 47 years old diabetic patient since last 15+ years. Living in Gurgaon, India. I am 5′ 7.5″ (77 kgs). On December 23, 2011, I was playing a game ‘dodge the ball’ out in a resort. Suddenly while dodging the ball, I twisted my knee and had a lot of pain, felt darkness in front of my eyes, unable to stand on my own. The xray didn’t reveal any fracture but was advised to undergo a MRI test. MRI revealed:
– Haemoarthrosis
– Fracture left lateral tibial condyle with depressed fractured fragment
– Contusion of Hoffa’s fat pad
– Soft tissue contusions along lateral aspect
I was given option to undergo a surgery or get plastered for 6 weeks. Since surgery wasn’t insisted upon I opted for a plaster for 6 weeks and thereafter advised to undergo a physiotherepy session for 2-3 weeks. I took physiotherepy sessions for 5 weeks and felt better in walking. But after that 3 weeks down, I suddenly felt a lot of pain while climbing up or down the stairs. The pain persisted and didn’t go away, instead increased everytime I tried to climb up / down the stairs. I am however able to walk on plain surface properly. But feel pain in the knee sometimes, when I put my foot on the uneven surface.
Hassled with my problem, I consulted another Orthopedic Surgeon, who suspected of an ACL break and did not trust the earlier MRI report. He however advised me to do certain exercises at home for 3 weeks but of no avail. I was advised to undergo another MRI test, which revealed the following:
– Schatzker type II fracture of lateral tibial plateau with bony depression of 3-4 mm
– Adjacent floating anterior horn of lateral meniscus
– ACL partial tear / myxoid degeneration
After this nothing much has been advised except that a surgery should have been performed at the first place instead of putting a plaster on my left leg. The bone has since joined but depressed by 3-4 mm, which is a big depression and nothing much can be done now. I have been asked to do an exercise for 4 weeks applying weight of around 2 Kgs on both my foots and then to lift the legs. But its been 6 weeks and am unable to lift the weight. It pains too much at the following spots:
– Centre of the knee cap top
– Left hand side corner beneath the knee, and
– I have swelling on the thigh side on top of the knee, it hurts there, whenever I put my foot on an uneven surface.
Please guide me with respect to the possible best treatment with options, if any, time frame required for the same, for how long one would need to be immobile etc.
Im sorry… this is a difficult situation. The majority of your pain is PROBABLY coming from the depressed joint surface. It like has, or will result in post -traumatic osteoarthritis. Without examining you and talking with you I can not comment further. If osteoarthritis has developed or is developing, I would talk with your surgeon about your options. I would not consider an ACL procedure… but there is an outside chance or slim possibility that an arthroscopy simply to deal with the meniscus tear might improve your symptoms. Unfortunately, a knee replacement is likely in your future.
If you look at my sports blog, there is a guide to management of degenerative or arthritic knee.
https://www.howardluksmd.com/sports-medicine/degenerative-joint-disease-treatments/
Howard Luks
sasha
Hi, I’m 27 years old and have torn lateral meniscus in the posterior horn in both knees. I had a partial removal in the left knee with no improvement. They also told me that I had wear on the articular cartilage in both medial compartments bu tthe medial menisci are intact. his doesn’t seem to make sense to me, I would think the articular cartilage would be damaged on the same side. Can you shed some light on why this would happen please? I’m considering an allograft but I’m worried that this means I’m not a candidate. Thank you for your consideration.
Tough questions and issues today! Sasha.. Without examining you and understanding far more about your symptoms etc it would not be possible to comment about a transplant, which is a big procedure. Degenerative changes in a 27 year old are rare, but do occur. It is important to identify your pain generator. I would probably talk to your doctor about a new MRI to assess the knee already operated on to see if there is a residual tear or degeneration because of the excision.
Good Luck
Howard Luks
Robert
There is an acute, minimally depressed intr-articular fracture seen along the medial weightbearing surface of the tibial plateau. There is 2 mm of depression along the weightbearing surface of the medial tibial plateau. it is seen in association with small chronic osteochondral defects along both of the weightbearing surfaces in the medical compartment. These fragments are displaced and are prrobably loose within the joint space. There is a small to moderate-sized joint effusion present. there are plica seen in the suprapatellar recess of the joint space. There is also a small complex Baker’s cyst seen in the medial popliteal fossa. The cyst is complicated by multiple thin internal septations.
The anterior and posterior cruciate ligaments, as well as the medial and lateral collateral ligaments complexes are normal. The quadriceps, patellar tendon, flexor retinaculum and itiotibial band have a normal appearance. There is a grade 2 reparative signal seen in both menisci. There is also a horizontal cleavage tear seen in the posterior horn of the medial meniscus. The tear extends to the superior surface in the middle one third of the meniscus. There is no meniscal cyst formation present. the surrounding soft tissues and popliteal fossa are unremarkable.
Do you think i will need to have suregery to repair this?
This sounds like it was the result of a traumatic injury? No?
Katherine
Hi Dr. Luks,
My eleven year old daughter is a level 7 gymnast and injured her knee last November in a dismount /fall from the uneven bars. We thought she had just hyper extended it, did some RICE. Since then the pain in her knee (and popping sound) has gone away and come back several times. We saw an orthopedist in April, and after an MRI, he diagnosed discoid meniscus and a femur bone bruise right where the knee joins to the femur. He wanted to err on the conservative side, so she practiced for a few weeks at the gym doing no pounding moves like dismounts and vault, etc. Then we took her out completely for 3 weeks. Recently back at the gym, and all seemed well until yesterday during running warmup, it started hurting her again. We are seeing the orthopedist again this week, but want to go in with plenty of information. Is it time for surgery to trim the meniscus to make it fit correctly? Will it usually fix it with no problems in the future? How long is the recovery? She is a small girl, about 65 lbs. and in excellent physical shape….
Any information you can give me, would be greatly appreciated.
Tough decision… if too much of the meniscus is trimmed she could be subject to osteoarthritis, etc. Is the meniscus torn, or simply a discoid meniscus? If her pain is due to the meniscus it should improve… however, the bone bruise should probably be re-imaged to be sure it has not evolved into something else like osteochondritis dessicans, or an articular cartilage abnormality.
Just my thoughts… not meant as medical advice.
Howard Luks
Cenk Koz
Hi Dr. Luks
I had a meniscus surgery and it was repaired. 6 months after the surgery, I slipped in the shower and hurt the surgery area. It healed but not %100. About 3 years later I went on a trip and walked about 7-8 days. I started feeling pain and could not walk more than 30 mins after the incident. I went back to the same dr and he got my knee drained with a cortisone shot and most of my pains are gone. I still have slight pain and when I wear dress shoes if I dont use my foot more than my knee ( I guess it is a pressure issue) my knee hurts. I wanted to know if there is more liquid left in the knee. Can the person who drained the knee could have left some in there? My dr said it would be diminishing returns if I went to get it drained again. He said I should be ok now. MRI looks ok. I can squat. I can jump. For some reason I dont feel confident in making every move though because of the slight pain that I have. I would appreciate your opinion. Thanks take care.
Hassaan Zuberi
Hi! Dr.Luks
I found this thread of meniscus tears very useful and informative. And i have learned a lot from it. And Thanks to Dr. Howard J. Luks of giving such fine and logical advices.
I am 21 yrs old university student. Occasionaly play soccer—-2 months ago i twisted my left knee during playing soccer and the sudden pop is very painful, made me to kneel down. But after few seconds i got off the field on foot and walked to hostel that is 1 km from the ground. After 12 hours, pain increases and i m not able to walk properly. Then intially i messaged the knee and i felt better but after that i googled my injury which suggested me to do R.I.C.E (Rest, Ice, Compression and Elevation). I did all that and felt better but walk with a limp. After a week minor swelling starts and i started some pain killers on the recommendation of GP. After three weeks i stopped eating pain killers and the pain subsided , but not able to bare weight on my left knee. I kept doing quadriceps exercises which helps in reducing stiffness. After month and a half i am able to kneel down and bend my knee but cannot bend it to full extension– such that my ankles touch my buts( much like the child pose in yoga) but still its improving. There is some swelling in the medial side of the left knee which is still present but never got worsen. I can do elliptical trainer and cycling without hesitation and feel more better.
Now i have visited 2-3 orthipedicians which suggested me arthoscopy surgery based on my MRI report. My MRI report says:
Findings
Abnormal linear signal intensity involving the posterior meniscal horn, more medially.
Abnormal signal intensity with edematous thickening seen, involving the proximal ACL and LCL; otherwise cruciate and collateral ligamnets are intact.
Considerable joint effusion seen, more at retro-petellar region, extending cranially.
Rest of the things are perfectly normal.
So Doctors say that i have a medial meniscus tear and are pushing me for an arthoscopic surgery to remove the torn piece.. I ‘m double minded that what should i do——-go for arthoscopy or just wait for few months.
Current Condition:
I can do swimming, cycling and jogging at a resonable pace. Feel no pain in walking and doing stairs. Only feels a sharp and pinching pain at the medial portion of the knee when in full extension (like in child pose or squatiing). Taking no pain killers nor anti-inflammatry medicines.
So Doc, Please help me what should i do!!! Kindly Reply me…….
Jeen
Hi Dr. Luks,
I was diagnosed with small tear on the inferior peripheral part of posterior horn of medial meniscus.
I have gone to two doctors and they have two different opinions. Tough case for me. The first one said I can wait, but he would rather suggest an arthroscopy for partial meniscetomy since I am over 40. The second one said there is nothing to worry and he wouldn’t do anything. So I should pretty much adjust to reality and have an occasional pinches from twists and turns but overall I should be able to live well since I have very good ROM (I can walk straight, jog a little and squad without any pain). He sent me to PT for 6 weeks and I am pretty much done with it by now. My leg muscles are much stronger now and I feel much more stable. PT said they have done everything they may offer.
The problem is, that I still have painful sensations almost every time when I twist or turn in the form of sharp pain, but pain almost immediately disappear. The second problem is that I have a definite click or snap every time when my knee comes from bending position to full extension. I have been reading a bit about joints and understand knee anatomy by now. So, the main concern is: If I let it go without surgical intervention (considering that my pain is minimal), should I worry about damage to cartilage on the femur and tibia as torn meniscus is rubbing against it? These clicks and snaps constantly make me feel nervous in the sense that if I don’t take care of it now, I may have troubles down the road. Or this is something I should not think and as long as I don’t have pain associated with clicks and snaps I have nothing to worry about?
Appreciate you thought.
-JG
Jeen…
This is a common worry that people with meniscus tears mention. If a tear is large, or if a flap is present, then the tear can rub on the articular cartilage, or the cartilage that coats the ends of the bones of the knee. It would be unlikely that a small tear would do that. That being said… if your tear is creating these “mechanical symptoms” then the tear might be larger than the MRI alluded to. It’s a difficult decision, because you have very little pain. Unfortunately I can not answer the question the for you… Time to have a long sit down with the doctor you feel is most likely to listen to your concerns and engage you so that you can make a proper informed decision.
Good Luck
Howard Luks
Tarun
Hi doc,
I had an accident 1 year back which injured my knee, I’ve done mri n the report says ” Small mildly displaced osteochondral fragment along the medial facet of patella”……
I have intense pain while bending my leg to the extreme positoon near my butt….
My doc says its a minor issue n can b resolved by exercise n no surgery is required……
What r your suggestions…..?
Time will tell… but even small pieces of bone and cartilage can annoy the knee joint. If your pain persists beyond a few weeks I would talk to your Orthopedist, or a second opinion, about the options available to you.
Good Luck
Howard Luks
Maggie G
Hi Doc,
Just had my MRI results back and the outcome is as follows:
Conclusion: The MRI of the left knee reveals partial thickness horizontal tear of psoteror horn of medial meniscus. The lateral meniscus is is discoid.
Minimal chondromalacia patella.
Important to note that i am a 33 very active woman – yoga, biking, hiking, rock climbing, Roller blading and trekking. I am very very worried at the moment.
I am getting physio for my chondromalacia and the result is amazing. The partial tear is a bit of a challenge for me.
My ortho gave me a list of Not to do activities and the list is quite large and depression inducing. He also told me that a complete tear is inevitable! WTF
My sports injury doctor was more cool about it and said that I should not stop doing the activites I want and he will see me next week.
What are your thoughts on this one? I am very very worried.
Thanks
I typically treat patients, and not MRI findings. The tear may complete itself, and it may not. No one knows for sure. Even if it does complete itself, it may not be painful. I generally allow my patients to participate in activities that they tolerate. The decision to proceed with surgery is typically based on a patient’s perceived quality of life and the impact that the meniscus tear has on it.
Good Luck….
Howard Luks
Maggie G
Hi Doc,
So I can bike and swim ( knee extensions over 90degrees) and do squats? or these should be avoildable? Anything you would rather I NOT do at all?
Love the “I typically treat patients, and not MRI findings”!
Thanks!
Name Rocky
Dr. Luks;
I have performed significant research on-line related to my knee injuries over the years and have found the information you share to be among the most thorough and informative. Kudos to you for taking the time to respond to the inquires you receive.
Like many here I have a conundrum, to have, or post pone surgery.
At 52 I still maintain a very active lifestyle and make great efforts to maintain fitness so that I can continue to purse the activities I enjoy (skiing, kite boarding, surfing, hiking, etc.).
Six months ago (December 2011), while kite boarding in Maui I heard a loud pop and felt pain on the lateral aspect of my right knee with immediate instability. A week later I went to my Orthopod, who I feel has my best interests at heart and understands the quality of life I get through my sports. By the time I saw him the knee was feeling a bit better. He felt I may have sprained the knee in some fashion and suggested I wait and see how it went; no MRI or X-Ray was performed. The knee seemed to improve over time to the point where I was able to finish out the end of the ski season and return to pretty much normal activity.
About Two weeks ago (June 12), while simply putting on my sock I again heard a loud pop and felt pain on the later aspect of my right knee. There was immediate instability, and swelling very similar to what happened in six months ago in Maui.
I followed up with my Doc again after about eight days later. MRI revealed tear of the lateral meniscus in the white zone. Dr. recommends a partial menisectomy. The rest of the knee (articular surfaces) was unremarkable so no significant signs of arthritis yet.
If I go forward with the procedure this will be the second surgery on the right knee. The surgical report of the previous menisectomy on my right knee (in 2003) indicated that 80% of my medial meniscus and 30% of the lateral meniscus was removed (the rim was intact both medial and laterally). I also have two previous surgeries on the left knee, a full ACL tear repair and partial mensiectomy).
Though my knee has been improving (after two weeks) it still pops, I still limp (not as bad) and I am unable to fully extend or “lock out” the knee with out pain. I have been to the gym and have no problem getting on a stationary bike for 40 minutes and have been stretching.
The Dr. thinks the tear probably occurred while kite boarding six months ago, was asymptomatic, and I reinjured it while putting on my socks. Friends (former ski patrollers in Canada, not MD’s but educated and knowledgeable) have cautioned me about rushing in to surgery. Their views are consistent with literature regarding the hastening of osteoarthritis from removing too much menisci.
My Doc. seems to feel that by not having the surgery done I may be risking even further injury as lose pieces of the torn meniscus could cause instability in the knee. Also, as I understand it, if the meniscus is torn in a fashion that causes uneven pressure from the meniscus on the articular surface, that not having the meniscus trimmed could cause greater ware and tear than having it removed.
So, my question: Given the history I described, do you think I am risking greater injury by either not having the surgery or waiting longer to have it perfumed to see how the knee goes, particularly since I want to continue to pursue an active life style?
I’ve had good luck with my previous surgeries, in terms of being pretty much pain free and returning to a fairly high level of sporting activity (considering my age). I am obviously not shy when it comes to surgery, but do not want to be over zealous looking for a “quick fix” that may have adverse implications down the line by hastening the onset of osteoarthritis.
The decision is weighing heavy on my mind. I am a counselor and assist people making life choices so I don’t want to let me emotions overrule my intellect.
Sorry for the length of this inquiry, tried to make it short but did not end up that way. Any feedback you could offer would be greatly appreciated. If you are a skier and ever make it to Tahoe, I would be happy to show you some good runs! Thanks gain Doc, the service you provide here is outstanding.
Rocky… I appreciate your comments !!!! Unfortunately my spam folder caught this so forgive my tardy reply.
When patients have mechanical symptoms, popping, snapping etc, we (orthopods) worry that the meniscus might be damaging the other cartilage in the knee— the articular cartilage. If that occurs then you will develop arthritis due to the defects created by the loose piece flopping around.
Most people don’t realize that the risk of developing arthritis actually begins when you tear your meniscus… because it is no longer functioning normally. You are correct though… if the surgeons resects “too much” or is a bit aggressive then that can certainly accelerate the process (sometimes).
You face a tough decision… but it needs to be thought of in the framework of your quality of life. If you can not pursue the activities you want to, at your usual pace, etc then you need to decide if that is ok with you or not.
Hope that makes sense.
Best of luck to you!
Howard Luks
Name Lisa Bates
Hi Dr. Luks:
Normally, I would never seek advice on the internet from a doctor whom I have never met or seen in the office, but….after viewing your video and reading the comments in this long thread of questions and answers, I feel like it is worth an inquiry to see what you suggest or advise.
My husband is currently 49 years old. In February of 2011, he had a seizure and was diagnosed with an AVM. He was in the ER at the time of diagnosis and the neurosurgeon recommended immediate surgery to seal off the leaking AVM. We did not seek a second opinion because my husband was described as “an excellent candidate for the procedure which the doctors at this nationally ranked hospital performed successfully several times a day, thousands of them a year.” The doctors said “he had no risk factors for complications from the surgery and that he would be back to his normal schedule within two weeks.” I received a phone call from the surgeon from the OR telling me that the embollization was a success, but that when they did a repeat CT to check the repair for leakage, they found that my husband had developed a blood clot deeper in his brain as a “direct result” of the procedure and they needed my permission to do emergency brain surgery to evacuate the clot or he would die. Of course, I gave them permission! He had another brain surgery a day later because of extreme swelling in his brain. We were told he would die without it and that even if he survived the surgery, he would probably never wake up, remember us, or be able to think, talk or walk again. He was in a coma for about 30 days, then he woke up, he did remember us, he could think and he can talk. There are some deficits – serious vision cuts, but he can see and, of course, he has left side neglect and weakness. He has been to several rehab facilities and he is now in a nursing home because he can still not move his left arm or leg and is considered a “two person assist”.
I shared that background with you because I felt it was important to know before you gave me any advice about how to approach his medical issues relating to his knee. Within the past month, he fell out of his wheelchair while he was riding in the nursing home shuttle on the way to an appointment with his orthopedist. He was going to see the orthopedist because of a torn rotator cuff in his left shoulder that was extremely painful. Within a day of the fall, his left knee swelled to the size of a cantaloupe or small watermelon. He indicated it was extremely painful. He takes regular meds for pain including tylenol and tramadol, but they were not enough to relieve the knee pain. So, as a last resort, he took oxycodone. He has been wearing a knee brace since we visited the ER two days after the injury. The swelling has gone down. He reports minimal pain, unless his leg is moved. He has not needed the oxycodone since the swelling subsided a few weeks ago. He had an MRI about two weeks ago which revealed that he had a “non-displaced tear to the medial meniscus”. We are waiting to see the orthopedist again to discuss options. I trust our orthopedist, but I am feeling like I need to do more research and be prepared because of how unprepared we were when it came to the surgical repair of the AVM!
I am thinking that a conservative approach regarding surgery on the medial meniscus tear is appropriate given my husband’s situation. I would rather take a wait and see approach. The problem is that he is not able to move his left leg. There is no clear evidence as to whether this is permanent or if it could improve with time and/or rehab with him. He was able to stand with assistance when he first entered the nursing home in December of 2011, but he could not walk or take steps. If he could stand and pivot from a bed to a wheelchair or a wheelchair to a seat in a vehicle, his whole life would change. If he could stand and pivot, we could probably bring him home to live with us instead of him having stay in the nursing home, which he describes as “prison”. We have three sons, ages 17, 15, and almost 12. They are big guys – the 17 year old is over 6 feet tall and close to 300 pounds, the 15 year old is over 6 feet tall and close to 220 pounds, and the 12 year old is 5’7″ and 160 pounds. So, the 3 of them could definitely help manage their dad in terms of helping him stand to pivot, etc.
My questions are :
1) If we take a wait and see approach regarding the tear, how long should we wait and see?
2) If we don’t do the surgery, does that mean that Tim will likely not be able to stand and pivot
even if he improves enough neurologically to do so? ie: would the tear prevent him from being
able to do so mechanically without a neurological deficit regarding movement.
3) Would you recommend any physical therapy in the mean time to keep his left leg moving, etc.,
to facilitate the healing of the tear since he can’t move the leg/knee himself?
If you have any other thoughts or advice, I would be open to hearing it! I am sorry for the length, but I knew that the complexity of Tim’s medical status needed to be taken into account :) I completely understand your disclaimer and know that you may be limited in your ability to give any advice because you are not Tim’s treating physician and you have not examined him or his records. I just figured it was worth a try :) Thank you so much for your time and dedication to patients. There needs to be more doctors like you in the medical community! We are lucky enough to have found a family physician who approaches medicine in the same way you do. To everyone else, they are out there, I promise…..it’s just a bit harder to find them :) Once you do, though, don’t let go!
With deepest gratitude and respect,
Lisa
Thanks for reaching out….
My questions are :
1) If we take a wait and see approach regarding the tear, how long should we wait and see?
This varies by individual… if you see progress and notice that the pain is diminishing then you can continue to wait to see if the issue resolves itself. If the pain persists despite non-surgical measures, then surgery is certainly an option to pursue.
2) If we don’t do the surgery, does that mean that Tim will likely not be able to stand and pivot
even if he improves enough neurologically to do so? ie: would the tear prevent him from being
able to do so mechanically without a neurological deficit regarding movement.
Not all tears behave the same way. Meniscal tears rarely incapacitate people. They typically hurt with turning pivoting and twisting — or kneeling and squatting. If there is a large, unstable tear, then the pain and catching can be more severe….
3) Would you recommend any physical therapy in the mean time to keep his left leg moving, etc.,
to facilitate the healing of the tear since he can’t move the leg/knee himself?
The tear rarely “heals” in the true sense of the word… instead many tears simply become asymptomatic or do not hurt any longer. Physical therapy may be of benefit, especially in light of his other issues he is dealing with.
Good luck!
Howard Luks
Name Lisa Bates
Dr. Luks:
Thank you SO much for your quick response and your advice! I really appreciate your time and effort in reviewing and responding to my questions. Your advice will definitely help me in considering what to do with Tim’s meniscus tear.
Thanks again,
Lisa
Nancy
Dr. Luks,
Thank you very much for a very informative website. My mother, age 59, started having knee pain about 3 months ago. MRI showed possible radial tear. Ortho suggested conservative treatment and asked to come in if pain is not improved. She has been doing PT for about 5 weeks now. Pain has improved but she is still having problem doing all daily activities without pain. She stopped taking Meloxicam three days ago to see if she can go on without medicine, however, pain became worse off of it and swelling is three times worse. Do you think she needs surgery at this point? Would surgery increase her risk of OA? I have heard of chiropractors who claim of cold laser therapy being very successful for meniscal tear. What are your thoughts on that?
Thank you very much.
Thanks for stopping by Nancy…
Your surgeon sounds like he/she is conservative and you need to respect that. Whether or not an arthroscopy is warranted is a decision for your mom’s healthcare team and her to decide. It is predominantly a quality of life decision. Yes, arthritis usually occurs after a tear, and/or after surgical excision of the torn portion. But for many, having a few more pain free years with the knee is worth the risk of developing OA. There is no literature on cold laser and meniscus tears…. so I can not comment on that. Time to have a sit down with her surgeon and discuss these issues and then your mom will have all the facts necessary to make an informed choice.
Good luck
Howard Luks
Nick Angeloni
I tore my meniscu about 5 weeks ago and with rest and ice i have seen much improvement. However, even though no specific motions give me bad pan like they were when i first tore it, then is a very slight pain that a cures almost all of the time. It is very slight and like i said i can do all movements without pain. But just sitting down or standing i feel a little something, will this always feel this way or is this a sign that i need more rest before returning to sports?
sagar
Hello Doc,
I am 27 years old. Exactly a year ago, I had undergone ACL replacement surgery and thereafter completed the physiotherapy sessions religiously. But my knee is still wobbly and unstable. So, I met the doctor who had performed ACL surgery on my right knee. After brief examination, the doc said there is no problem and knee is absolutely fine. He gave some pain relievers and recommended ice packs.
Since the doc said there was no issue, I continued with my regular activities. But surely there was a big problem. Every now and then when a little extra stress is applied on the right knee, it would pop. The situation now is such that before placing my right foot on the ground, I pray it doesnt pop.
Even before last year’s surgery, the knee used to keep popping in a similar fashion. The difference now is that after popping, it doesnt swell like a balloon.
I decided to show my leg to another doctor. He suggested MRI which concluded –
– Tibio femoral tunnel with ACL graft in situ.
– Minimal knee joint effusion.
– Grade-II horizontal tear in horizontal tear in posterior horn of medial meniscus.
Now this doctor has recommended a surgery. Should I go ahead with the surgery? I am very confused and frustrated. Please advice.
Thank you.
Regards, Sagar.
Sagar… For various reasons many surgeons may not want to recognize or reveal that their reconstruction wasn’t tight enough, positioned properly, etc… If you leg still feels loose, then the graft or new ACL might be loose… and there are many reasons for this. An MRI will show that the graft is present, but it will not tell you if it is tight enough… only a properly performed exam will tell you that.
I’m not sure why the second surgeon is recommending surgery… it is not indicated for a Grade II signal (which does not mean tear). Are they suggesting a new ACL be placed, etc…
Sounds like a third or fourth opinion is necessary, but this is clearly a case where you need to rely on a good, qualified sports medicine trained orthopedic surgeon —and their examination, which will tell you whether or not the ACL graft is functioning well.
HJL
Name Erica
Dear Dr. Luks –
I was diagnosed with a chondral flap that had “peeled” away from the right kneecap. I am a runner and 8 months ago completed my first half-marathon. Since then, I had striven to keep up my mileage to mid-twenty miles a week, and had most recently (mid-March) run a 7-mile “extreme” race up and down very steep trail hills. It was after this extreme run, and a yoga class in which I splayed my legs out so far that I felt it pull on my knee cap (I’m not sure which event was the cause of my pain, but it was a couple of days after the run and the yoga class that the pain started).
Anyway, as a result of this chondral flap issue, I can no longer run. If I run, I can only run a couple of miles before it starts to hurt. And, the next day, the pain is so bad I can barely walk on that right leg. I was able to ride my bicycle without too much incident until last weekend.
Last weekend, I was working in the garden and using a large shovel to try to dig out some large weeds. As I placed both feet on the shovel, and put my full weight onto the shovel, I felt and heard something snap in my right knee – there was pain, and it gave out. I limped inside and iced it and took ibuprofin. It hurt more than usual for a few days, and I initially was not able to put much weight on it. Over the course of the week, it has started to feel better.
However, I am still — after 2 1/2 months – unable to fully bend my knee. When I accidentally pivot, it is very painful. I am beginning to feel that I need to have surgery for me to be able to resume my active lifestyle of running, hiking and biking. What are your thoughts? Thank-you. – Erica
Erica…
A chondral flap is a much different issue than a meniscus tear. It is also an issue where we have techniques available to us to try and substitute for the resulting defect when the flap is removed. Time to find someone well versed and experienced in dealing with cartilage restoration to review your options.
Good Luck!
Howard Luks
Ahmed
Hi Dr. Luks, Thanks for this great website.
I have a grade 3 tear in the medial meniscus of my right knee. It’s not that painful, but there is a lot of discomfort due to the very frequent clicking (it feels like something gets out of place, and then needs to be clicked back into place). I’ve had the tear for a few years now and have avoided surgery, but over the last few months it got aggravated when I tried light exercise of my legs. I can’t walk a few steps without having to stop and ‘click’ it back into place… Is surgery my best option, or is there a way I can strengthen my leg muscles enough to compensate?
Also, my left knee has started to hurt a bit at the same medial meniscus area, which shows ‘mild degeneration of the meniscus’ on MRI but no tear. I’m trying to figure out what exercises I can do to strengthen my leg muscles (which are quite weak) without aggravating either knee. When I try basic leg lifts or elliptical, it aggravates both knees. Any advice?
Lastly, do you think prolotherapy is a good option for me? Thanks again.
Shivani
Hello Dr. Luks,
Thanks a lot for this wonderful load of information. I am due for surgery tomorrow for my meniscal tear. But my instincts tell me not to go for this surgery. The doctor who suggested surgery sounded like he just wanted to put it on record more than anything else. That kind of mindset made me doubt if in fact I needed surgery.
History- about 6 months ago, I had this acute pain when I could not walk at all. That’s when we went for MRI which showed meniscus tear. As far as I understand, it is a transverse kind but as I write this, I am asking them on phone on what type is it. Doctors could not be sure if it was becoz of injury or wear and tear type. I am usually too lost with my kids to recall if I had some sudden pop or injury.
Then the pain subsided within a couple of days. After that it has been very minimal pain. Sometimes goes up depending on how I spent my day but totally under control. I have 3 kids out of which twin toddlers and therefore we have a moderately active lifestyle. This includes taking them to parks, helping with bars and occasionally playing tennis with my beginner 7 year old.
I don’t have time margin to go for another doctor’s opinion, at least not before our trip (if I had to undergo surgery afterall).
We are headed for a hectic Europe trip in exactly 27 days from tomorrow. My question is how necessary it sounds like a case of surgery considering I am very much fine and doing my regular business every day. But just the fact that I have this medium-large level tear. Also will it be enough time to get back in shape after surgery (less than 4 weeks).
Concern-if I choose not to go for surgery, will it be causing increased rate of damage to my cartillage and ultimately knee, welcoming arthritis?
Pls help, I am ready to make that phone call for ‘cancellation’.
Thanks a bunch in advance.
Shi
The decision to proceed with surgery should primarily be based on your current quality of life. Can the tear become larger, yes… but that chance is small. The risk of developing arthritis starts the moment you tear the meniscus… and if too much is removed it actually increases the risk further.
It sounds as if you have already made up your mind… step back and think of the things you shared with me…
you’re feeling well
you’re not entirely happy with your relationship with your surgeon
you have questions that have not been addressed
etc….
I hope this helps!
Good luck in your decision making…
Howard Luks MD
Shivani
Thanks a lot for your quick response. I am unsure about this small part of my question ‘the fact that I have this medium-large level tear’. Are you suggesting (your disclaimer taken into consideration) that its ok to carry medium-large tear? And I may not need surgery if my pain is under control for another few years? Is surgery more for pain management or fixing some mechanical/technical things in my knee.? Pain is certainly under control but I don’t want to postpone something that may affect me negatively long term.
Thanks a lot in advance for clarifying this last piece for me.
Shi
Name wayne
hey doc
quick question ?
pre-season traing feb 2012 soccer
twist knee tear in miniscus but not a bad one
things seem to have healed but unsure wether or not to go back to soccer yet
as it has been 3 mnths or so
knee stable never was unstable
so when is the right time to go back to sport?
by the way im 49 yrs old which may not go in my favour
so im a bit unsure what 2 do?
thanks for your time great website have learnt alot
cheers wayne
Wayne…. Three months or more is more than enough time to go and test out your knee and see what happens. Decision making in whether or not surgery is necessary for a meniscus tear is not straight forward and is typically geared towards suiting issues which effect your quality of life. Either you will tolerate turning, pivoting, twisting, etc or you won’t. If it bothers you when you attempt to play, that’s when you face the decision of changing your knee to suit your lifestyle or changing your lifestyle to suit your knee.
Good Luck!
Howard Luks
miracle ear prices
Ok so I am thinking about removing my site from Tumbler and get it to a WordPress site. I think this is a wordpress site right? If it is, may I ask where you got the theme? Thanks a bunch!
Julian… Do you want to know which theme I used? The paid versions of wordpress offer a HUGE number of available themes…
Ethan
Hello Dr. Luks,
Thank you for having this thread/blog. It must be a lot of work and I’m sure everyone here very much appreciates it. I am a 37 year old male. I have a history of degenerative disc disease in my lumbar spine. While doing PT for a recent exacerbation of this, I started to suffer knee pain. The PT involved “bridge” work (pilates/yoga style) and wall squats which kept my knees flexed and bearing weight. It wasnt a sudden injury, rather an insidious onset. On exam and MRI I was diagnosed with a right medial meniscus tear. Partial meniscectomy was recommended. Then, with no other stress put on my knees, my left knee developed identical pain albeit with less effusion. MRI confirmed a medial meniscus tear on the left knee as well and surgery on both knees (simultaneously) was recommended. I know the right knee he said probably 10-15% has to come out. Havent asked how much on left yet.
I think I am sold on having the surgery. The pain is by no means unbearable. I dont think i have any instability though i havent pushed it too much. However, the pain is definitely exacerbated by my golf swing (particularly the left knee which twists and bears weight with a right handed swing). And this is the one activity I desperately dont want to give up.
The real rub is that my family has a vacation planned in early july (six weeks from now). We are going to South Dakota/Wyoming to national parks. An outdoorsy trip. I plan on cutting any hikes down to only easy and flat ones (or just long walks). We will be going into caves that have many stairs to go up and down. Maybe a horseback riding tour (never been) but not sure if this is too unpredictable. My surgeon thinks its OK to go and we’ll do it when I get back. He says be smart, wear my braces, expect some increased pain and to treat it. He doesnt think I’d be taking a risk in terms of short or long term success of surgery by taking this trip.
My questions I have for you are:
1.) Is it reasonable for me to take this trip? Is the increased activity and possible increased pain going to worsen my chance for a successful surgery or increase the amount of meniscus to be removed? Or is it simply a matter of what I can bear? Will it make my risk of arthritis development greater in the future?
2.) Is it commonplace to do 2 knees at once? Intuitively, it seems scary doing a procedure on both at once. It seems if things go wrong, then both knees are effected. Only having one procedure (one bout of anesthesia, etc) does seem appealing and taking twice as much time off of work would be tough.
I have an appointment with another ortho in a week and a half ( I got into this guy sooner). I may keep this one and get a second opinion with it.
Thank you so much!
Ethan… Is it possible to increase the size of the tear …sure. Is it likely, no. Most patients heal rather quickly from the removal of the piece … and your vacation should not be in jeopardy — but if you have it repaired (sutured), then that entails a longer recovery period and might interfere with your planned vacation.
There are many occasions where a bilateral arthroscopy is performed… there are upsides and downsides to having both done under the same anesthesia. This is something you need to explore with your surgeon.
Good Luck
Howard Luks
Ethan
Hello Dr. Luks. Thank you so much for your reply. Just a quick follow-up if I may. I saw another doc and he doesnt like doing two knees at once unless he absolutely has to. I believe I am more comfortable with this situation. He wants to do the worst knee first then see how it goes before doing the second one. He is a well respected Sports Med doc from a major university. It looks like I am having the first knee (left) done in early August. I’m told he doesnt like doing another surgery until 3-6 months later.
This would mean having the first knee done about 4 months after onset of symptoms and the second about 8-9 months after onset of symptoms.
In general: Will waiting 8-9 months to have surgery profoundly effect likelihood of short term success and/or greatly increase the risk for long term complications? Like I said my knees arent in great pain, I’m quite sure I can wait that long with respect to symptoms.
If it helps here are my two reports:
Right knee: 1.) Horizontal, slightly oblique tear of posterior horn of medial meniscus 2.) Mild arthrosis at medial margin of medial compartment 3.) Small effusion.
Left knee: 1.) Oblique inferiorly surfacing tear in posterior horn of medial meniscus 2.) Small septated cystic focus adjacent to PCL, from synovial recess versus small ganglion syst. 3.) Mild cartilage degeneration in mid patellar apex without focal loss. Similar changes in mid trochlear nothch.
Thank you so much!
Nicole
woahhh sorry Dr Luks*** not Luke…my bad mate…I saw your website and scrolled down as quick as I could to ask you a questions ehhh. :|
Debbie
Hello Dr. Luks,
Thank you for the very informative video. I have an interesting symptom along with the classic meniscus tear symptoms. Let me first say, I was squating down for about 15 mins and when I stood up it felt like my knee was “locked up”. I straightened it out but I felt a tightness above my knee that shot up the front of my thigh. I was at my sons wedding when this occurred. I did put ice on the knee as there was significant swelling on the inner side of the knee cap. I am now 48 hrs post injury and I still have the same amount of swelling and I can not bend that leg more than 90 degrees in. There is that tight, pulling sensation above that knee all the way up my thigh. I went to the er when it happened and they did an xray and said there were no bone problems. Does this sound like it could be a meniscus tear or something more serious? I was recently laid off and do not have health insurance. I guess I am wondering if I should see a specialist or just give it some time to heal. Thank you for any help or info you can provide me.
Sincerely,
Debbie
Tara
Dr Luks,
9 years ago I fell while in the military and landed on my knee on a sharp edge catching all of my weight just under my left patella. I watched my knee swell twice its size immediately. I went to medical and they told me they were busy and to come back tomorrow…. for 4 days I was told to come back until the 4th day my leg was so swollen I couldn’t put my boot on, and I was bruised from my knee half way down to my foot. they finally did an x ray. the first diagnosis was a fractured patella. I wore a brace for about a month and was confined to a bed most of the time due to being underway on a ship. when we returned home they informed me my x ray was reviewed by someone and there was never a fracture. I didn’t land on my patella I landed under it. I continued to have pain for a while and it went away for a while. I got out of the service and it started to bother me more and more and I kept going to the VA about it and all they did was x rays and they kept saying they didn’t see anything and it was fine. the pain got worse and my knee started giving out and locking up and swelling for no reason. I finally talked them into an MRI and they found that I have a torn meniscus. the only trauma I have had to this knee is that incident. the person I talked to said that because the injury is so old and is getting worse as far as pain and stuff that I would more then likely have to have some sort of surgery. I don’t know yet the type of tear or anything, all I know is its the left medial meniscus. my work requires me to be up and down ladders and stairs all day and allot of time squatting and kneeling which causes allot more pain and discomfort but, I absolutely love my job and want to continue with it. I was just wondering if you had an opinion or some incite to what I need to ask and discuss tomorrow when I go see ortho. thank you very much for your time!!!
Ibrahim
I am 26 and I have my meniscus torn, I have pain since 12 years but it was jsut during winter or when the weather used to be too cold. In 2010 this pain becomes permanent and I was suffering from pain in my knee. I went to Doctor unfortunately in Afghanistan we do not have knee treatment through Orthroscopy hence Doctor told me not to do open surgery as it’s not good in future.
Could you please tell me if I wait till get opportunity to have orthroscopy, is it dangerous for my bones if I dont do the treatment soon.
Please advice, thank you so much.
Deepak
MRI report for right knee shows.
Donna
Dr. Luks,
I am at my wits end, I injuried my knee 2 years ago, it swelled within 12 hours. I went to a doctor the following day who basicly exrayed it, all looked fine so just told me to use RICE and take motrin for a week….It only got worse, I had MRI which showed nothing, still continued over the next year to give worse as far as swelling, had steriod shots several times, no change, had fluid drained a few times but they never got alot considering how large my knee was.
Finally after a year and 2 months a doctor I went to said I had a torn Menicus. I had surgery swelling went down some but never got alot of motion back and swelling started back. Went to this doctor over the next 3 months, lastly he want to give me shots for lubercation. I decided to go to Duke University for a 2nd opinion.
The doctor immediately done surgery again, took out all my knee lining (this was very inflamed )and done a patella release, Instant relief, before surgery I had maybe 30% motion–i got 80% with in a few weeks. Did not have alot of pain after surgery and thought I was good to go. But with in that 2 week period my other knee start to hurt badly and swolled from the knee down. Went to doctor who’s first thought was to check for blood clot—it was a baker cyst very large, most likely cause from using that leg for now a year and a half for everything, he could not draw fluid out because it was very thick fluid.
So to surgery again, removed cyst, swelling went away within 2 days, leg feels great. Post surgery 2 weeks on bakers cyst. However within this 2 weeks the injuried leg has become stiff and thicking again above the knee as it was before surgery (post 10 weeks) motion is now at 60%. I had done PT after injured knee but had to stop a couple of weeks due to the cyst in the other leg being so painful. I am supposed to start back PT on Tuesday. The doctor as did the other doctors run alot of test on the fluids and tissue and all was negitive..I am in no way upset with my present Doctor , he has help me more then any other doctor giving I went to him after a injury that happened to years ago .I have good pain tolorence but not having motion is very hard on me since i have my job consist of alot of stairs. Any suggestions I understand you can not give me medical advise and this is a little information for 2 years, but thank you in advance for anything you can think of that my help me.
Sorry to hear you have suffered for so long … I assume tests for Lyme, Lupus, Rheumatoid Arthritis, other tick borne illnesses were all negative ??? What did docs say about whether or not there was any “arthritis” seen at time of scope? Some people simply have horrible inflammation with even mild arthritis… but I would be interested in Rheumatological results of diseases and entities I mentioned above….
Please keep in mind…. this is just general advice to aid you in your discussions with your doctor(s) and not meant as medical advice.
Marv
Hi Dr. Luks! Thank you for your website and for all of you information. I have read your suggestions regarding surgery for a meniscus tear and have been consumed with the decision to have surgery or not. I would be extremely grateful for your advice:
I am a 36 year old male with off and on knee pain for at least 7 years. Within this time, I have had approx. 6 major acute flare ups of pain and immense swelling, due to gout (for which I am now taking allopurinol to control). On two of the occasions, the pain and swelling was so bad that I had my knee aspirated and injected with cortisone. Once the gout flare ups subsided, I would have no pain and would be able to resume normal activities and exercise….until the next flare up.
Anyhow, since October/2011, I have had chronic knee pain and swelling which I again attributed to gout. The pain and swelling subsided approx. 80% until January when I had another major gout flare up in my knee. It was so bad, that I had it aspirated and received another cortisone injection. Well, it is now almost May, and although most of the pain and swelling is gone, I still have slight swelling and pain in the knee. In the past, once the gout flare up subsided, my knee would be fine, but this time, it is not fully recovering, thus I got an MRI which revealed:
1. Small tear of the anterior form of the medial meniscus with suspected debris/meniscal fragments anteriorly.
2. Slight attenuation of the ACL, however the ACL and PCL are intact.
I was not surprised to find out about my meniscus tear, because in the past, my knee would fully heal in a month or sooner from a gout flare up. My current knee pain and swelling has been ongoing for 7 months, thus I believe it is due to the meniscus and not the gout. Due to the length of time of my knee pain, I saw an Orthopedist this month. He recommends surgery to cut out the torn medial meniscus.
My current symptoms:
Medial knee pain on average, 3/10, however sometimes 7/10 when exacerbated, then subsides back down to 3/10 after 5-7 days.
Slight chronic knee swelling
Medial knee joint is tender to palpation
I can fully extend my knee, and I have about 90% of full flexion.
I have never had popping or locking, however, my gait is not normal. I have a very slight limp and feel a slight pain in my knee with each step. Sometimes this pain is very minimal and sometimes it worsens and I can not normally walk down stairs. For the most part, my pain is tolerable, however annoying and uncomfortable. I can not run, jump, or ride a bike without exacerbating the pain and swelling.
I sought a second opinion, and the based on my MRI, the Doctor didn’t think I needed surgery.
I have been doing conservative rehab to my knee focusing on strengthening my quads, hamstring, and gastrocnemius.
Anyhow, I cannot decide if I should have surgery or not because I can still function, however I no longer lead an active lifestyle, due to fear of exacerbating my condition. Also, I am wondering if the chronic swelling and knee pain is due to the meniscus, or from the residual effects of the major gout attack I had in January.
I am scheduled for knee surgery next month. Should I postpone it and give it more time to heal? Or is 7 months of discomfort and pain that I have experienced enough to justify the surgery.
My normal inclination is to not get the surgery and just try to rehab my knee, however, due to the length of time (7 months) of chronic knee pain, I am starting to lean towards the surgery. What do you think?
Thank you for your consideration.
Unfortunately I can not give you direct medical advice ….
The MRI findings are not “impressive” and, unless the scan wasn’t read well, the gout could be the cause of your persistent swelling. It seems like your are reasoning through this process quite well. It also seems like you have already made the decision. It truly is a quality of life decision… 7 months is enough time, in general — but in your case the gout is complicating things.
Good luck with the surgery and let me know how things go
Howard Luks
Christina
Hello, I am a 30 year old female, who has had 3 knee surgeries, all before I was 23! By the 4rd surgery I had my meniscus removed. I thought about 2 years ago I was in pain, would suck it up and only take a pain reliever when I was on my feet working for 20 hours for holidays. About 2 months ago I have been terrible pain, (the pain I thought was bad WAS NOTHING) I walk up steps and my knee feels weak, it hurts to stand, sit, walk, you name it. What can possibly be done for me? My worst fear is to go to the doctor and for them to tell me there is nothing that can be done. I have tried fish oils, joint juice, minerals, vitamins, anything I have read about that would ease the pain. I can’t imagine the amount of pain I am in getting any worse but I know I am young and I need my knee :(
Thank you for your time.
Time to see an academic fellowship trained sports doc… time to do some homework on meniscal transplants, scaffolds etc… That way you can have an educated discussion with your NEXT :-) surgeon.
HJL
Tim
About 15 years ago I had an acl and meniscus tear repaired and have had no real problems until about a year ago when I started having sharp pains in my knee when i walked. At first the pain would come and go then became more constant. I guess I learned to walk a certain way so I didnt feel the pain but it put a strain on my hamstring because it hurts now. Would scoping the knee and resting the hamstring be the answer?
First you need an X-ray and a good exam by a fellowship trained sports doc… An ACL tear that is 15 yrs old sets you up for possible arthritis, etc… A good exam and proper imaging will let you know what the next steps might just be.
Good Luck
Doubt it… have you had an X-ray and examination? This long after and ACL and meniscus tear you are likely suffering from osteoarthritis… Come back and visit us after the X-ray is done.
Howard Luks
Wendy
I was running on the treadmill two weeks ago when I heard and felt a pop in my knee. I had an MRI on Monday and called today for the results. I tried to Google the results so I could have a better idea of what treatment is to come but I could only find physician level information.
The MRI results are that there is a complex degenerative tear of the posterior horn and apex of the medial meniscus extending to the root attachment and a small partial tear of the anterior root something attachment of the lateral meniscus.
Can you tell me what this means? I go back to the surgeon for a consult in a couple of weeks and would like to have a better idea of what this all means so that I can take an educated and active part of my treatment decisions. Any insight would be appreciated.
Root tears of the mensicus are tricky. There are good repair techniques out there for them, but not many sports docs are performing them… after you discuss the results and the treatment plan with your doc, see if they feel comfortable specifically with meniscal root repairs.. if not you may need to find someone who is and who is willing to review the alternative available to you.
Good Luck
Lisa
Hi Dr. Luks,
I am an active 44 year old mother who was skiing with her kids 3 weeks ago when one of them ran into me while I was standing on the slopes. She hit me laterally causing me to fall backwards and my knees went medially and I heard a ripping sound with instant pain. I did have swelling and pain for a week with decreased ROM. I am a physio so I self treated and also had a colleague take a look at it and confirmed my suspicion. I am continuing to have aching pain, minimal swelling through the day and night and of course can’t squat or twist on it. I also have increased pain when I sit with my knee bent for too long or stand in one spot.
I am registered to do a half marathon in May which I realize now I can’t but I am also registered and paid for the NYC marathon in November which is a big goal for me to run in. I have already ran two marathons and qualified for Boston but wasn’t able to go. I also do triathlons olympic and half ironman and enjoying riding in Gran Fondo bike rides. I am very careful with my training and have not had any injuries or pain prior to the skiing incident. I am very conservative in everything I do as I am well aware of the consequences.
My dilemma now is that I am Canadian and there is a long wait to see an orthopod and even longer wait to get an MRI and if necessary surgery. I do know a number of them locally and can call in a favour but I would still have to wait for the MRI. I can go to a private facility and pay out of pocket, but it is $$$, Should I go this route or wait it out for another few weeks. I am trying to think optimistic and conservative but I will have to starting running on it by June to get ready for the marathon.
I am looking for your opinion because I like the way you think and totally believe in treat the problem not the MRI. I have worked as a highly trained physio in the US and Canada for many years all outpatient ortho and private clinics my whole career and have seen it all.
Look forward to your reply. Thank you.
It sounds a bit like an MCL tear mechanism too??? If so, then you know that pain from MCL tears can persist for months :-(. Perhaps if you describe your symptoms better and when they occur I can be of more assistance. Are you tender at the medial epicondyle of the femur ?
HJL
Tressa
Good morning, my husband had a large bucket handle tear in his meniscus, his doc insisted he have surgery and said he would be fine within days of the surgery and be back to work after a week. We agreed to the surgery as my husband was not able to walk without severe pain, popping and crunching. The surgery took a lot longer than the surgeon said it would. He stated it was a bigger tear than he first thought. After the surgery he was on bed rest for three weeks, then sent back to work on pain meds. He has had constant swelling since, increased pain and popping as well as crunching. He wakes during the night with his knee locking up or worse popping and not able to move it. When he started to complain he was told to take more advil, was given more pain meds and that it would get better When I insisted his doc look further he agreed to do another MRI, however first he wanted to try a shot of cortisone in his knee. Asked to come back 10 days later, did so no pain relief in fact felt worse once again. Another trip to the doc brought on oh we cannot do the MRI for a month since we used the cortisone. Waited this out, tried again, now the doc is saying we don’t need a MI he wants to inject something else into the joint. We are stumped as when we go back in all he gets now is more pain meds and nothing. We are told our insurance will not pay for the injections as they are very expensive. We asked if he is doing more damage to his knee and are assured he is not. However the pain increases, and his knee is swelling all the time as well as bruising on the outside of the knee on the side of his leg more and more each day. When we showed this to the doc he asked if he is using asprin. No only Aleeve at this point. We are then told to use 800mg of advil 4 to six time a day for swelling. Please help tell me what to do we are afraid he will lose his knee or worse his leg over this. My husband also has diabetes which does not help matters any.
Was the tear repaired and sutured or removed? If removed then response is unusual unless something else such as arthritis was present. If the tear was sutured or repaired then the repair may have failed. No need to wait for MRI after injection. No cause and effect there. Sound like it’s time for another MRI and another opinion.
Not medical advice… just something to ponder.
Please keep us informed.
thanks
NameGary
Dear Dr. Luks,
I strained my right knee playing tennis, and it was diagnosed as a strained ligament or tendon. Turns out it was a torn meniscus. After an MRI, I received a cortisone shot. Scoping may be indicated. I bought a knee brace that may allow me top play tennis again, even without surgery. My tear is lateral, with a small bit of debris in there. I am about to start a round of physical therapy. In the last round of PT I did exercises that may have aggravated my condition: 1) grapevine walking, where you move sideways, crossing your injured leg alternately in front of and behind the other one as you move, and 2) moving sideways in the direction of the injured knee and exerting some slight force as you plant the foot of the injured leg, ostensibly to strengthen the knee.
Your observation?
Thank you,
Gary, Minneapolis
Avoid inciting activities and if you can continue playing tennis with a brace, I see no reason to change up anything… but of course —this is not medical advice.
Angie Byl
Hi Dr. Luks,
I’m 37 years old and have a horizontal meniscus tear. I have pain in my left knee when I am active, such as walking, standing on my feet 2-3 hours at a time, and playing tennis. I was wondering, would having surgery make my knee pain go away so that I could walk without pain and play tennis without pain? Thanks.
Sean
I have been struggling with whether to have my knee scoped. MRI pointed to degenerative changes, but my second opinion doc said pretty much everyone has that. They did pretty thick slices on the MRI, too, which complicates things, leaving it inconclusive, at least in the second opinions view, though my symptoms point to a tear and justification for a scope. I have been leaning towards trying prolotherapy first. With 1.5 million arthroscopies performed yearly, I am really surprised at how little outcomes research there is, at least, I haven’t found it. Seems that grouping the tear type, meniscus, anterior vs posterior etc. would be easy enough to do, and then follow people 5, 10, 20, 30 years post-surgically. My feeling/fear with possibly getting the surgery is that it will create more instability, degeneration, and ultimately lead to a knee replacement. A veritable orthopedic revolving door cash cow. Lots of people get these and are good to go, but many others are not. So challenging to figure out. I was hoping you could speak to the outcomes part and maybe prolo. Thanks.
Mustafa
Dear Dr. Luks,
I have been diagnosed to have Grade II intrasubstance mucoid degeneration noted in the posterior horn of the medial meniscus, so is this some thing serious? and does it need surgery?
I feel that my knee is ok most of the time, but i some times have swellings in my knee, and cannot bend my knee, and when i run it really hurts, so how can i restore my normal life?
Lynda
I kinda have a short question. I play roller derby and have injured my knee in Dec 2011. Dr. said My ACL has a tear but not bad and I have a meniscus tear. I started wearing a ACL brace about a month ago and it feels so much better. BUT now the only time I have pain is when I fall on it playing derby. It is a very sharp and cramping pain. Then it’s gone. There is no swelling or tender anywhere. Everyday life is easy just can not fall on it. What does that kind of pain mean? I can full extend and bend my knee. I can squat but can only put some weight on that knee.
Dave
I seem to have recovered much better about 80-90% since my post on March 2nd. I did go see the Dr and he took x-rays and said my bones where is great shape then he did the usual testing to see if I had any muscle or tendon tears etc. He suspected Meniscus tear but could not conclude anything without an MRI. I told him I wanted to wait another 2 weeks before I do an MRI which is way to expensive in my budget. I have been walking with out my QUad cane now for about 1 week but noticed a slight pain a bit different than before yesterday so I am taking it easy again and using the cane for a little while to see if it gets better. Funny thing is I damaged my meniscus on my right knew 35 years ago and did not get any surgery then and continued to play Ice Hockey for 30 years later and only quit because I got a little to heavy. I have no idea how I could have injured my left one but I am giving it more time. How long could it take to heal if it does heal naturally? 6 months? 1 year? The Dr said I could re-injure it again and at that point I guess I would need the Arthroscopic?
Jason
Hi Dr Howard,
I’ve recently had lateral meniscus repair + partial meniscectomy. I work in the operating theatre and was wondering how much time off work I should be getting?
Thanks a lot.
Nancy Nelson
I am 72 years old. About a year ago I started experiencing a slight pain in my right knee on occasions, usually several weeks apart. The pain location felt internal. It felt like something was out of place. The pain lasted only seconds. As time passed the pain got progressively worse but still far apart and still onlly lasted a few seconds. In December, 2011, I was walking and the pain became very sharp. It lasted several days after which I contacted an orthapedic surgeon. I had an open type MRI with the following results: The medial meniscus demonstrates a minimal truncation-type tear along its medial edge beginning in the midplane and extending anteriorly. The rest of the MRI indicated all is normal: The lateral meniscus, cruciate ligaments and capsular ligaments are intact. The medial facet of the patella demonstgrates mild chondromalacia. The surgeon wants to do arthroscopic surgery and remove the torn part. I still do not have much, if any, pain or instability. Just popping sometimes when I first start walking. He said it will keep getting worse if I do not have it fixed. He really hasn’t given me an option. You say over and over surgery with a Medial Meniscus tear depends on quality of life. If it does not hurt hardly at all and so many people a lot younger than I have so much trouble after surgery, would it seem to be wise to wait or does the type of tear I have keep tearing if not fixed?
Nancy, thank you so much for stopping by and taking the time to comment. There is very little room in orthopedics to recommend surgery because something might worsen. Something I occasionally call “what -if ” surgery. Meniscus tears do not fall into that category. Although this can not be taken as medical advice… I would look for a second opinion. Meniscal surgery, in your 70s carries more risks than the same surgery in an 18 year old— and the #1 driver should be your quality of life… not because it may worsen. If it does worsen… surgery may be an option later down the line. Just something to think about…
Howard Luks
Orthopedic Surgery
Westchester NY
Dave
I should have told you in a seated position it would be the inner side and above the kneecap because when standing that area is not exactly the upper side anymore.
Dave
The medial side and slightly above my kneecap is extremely sore and hard to walk. How would i know if this is either a Meniscus or MSC issue? Would a sprained MCL feel more pain overall? It got swollen for a couple days and took Liquid Advil for about 5 days and the swelling went away never to return but the right side is very sore and if I push my fingers into that soft tissue are it actually hurts a bit.
Matt
Hello,
I did something very idiotic about 6 months ago where I was trying to mimic someone and have my feet face opposite directions (if you can picture that in your head). Anyway this required a twisting motion in which I twisted my leg a bit too far. It did not seem like a huge deal right afterwords all it felt like was maybe a pulled muscle at worst. About a week or so later I was at a party and danced…. the next day I was in extreme pain and since then my knee has been in pretty bad shape. I got an MRI that showed now tears, but a osteochondral defect in my patella. I took my results to an Ortho and he said that I most likely just sprained my knee and should be fine with Naproxen. That was 3 months ago……. I spoke with another radiologist and repeated another MRI. He confirmed the Osteochondral defect on the patella and I again took my results to another Ortho for anoter opinion. This new doctor felt that the symptoms I am having were likely not caused by the defect in my patella. From what I have read I really feel that my meniscus is damaged. It makes the most sense. I am only 27 years old and have had joint many joint problems thus far (Shoulder, Wrist, Ankle) and now the knee. Please give me your opinion on this situation as I am feeling very down and depressed at this point.
bryan
I am a 27 yr old male. I took a job construction job a few years ago and was working a lot on concrete bending my knees constantly. Both knees bgan to hurt and swell so I took a mostly sedentary job. The pain and swelling progressed so I had an MRI on both knees and was told I had significant oblique tears in both lateral menisci. Last month I had a partial menisectomy of the left knee and the surgeon told me he found arthritis in the knee, wich he cleaned up. I have no history of arthritis in my family, I’m not overweight, and have not played a lot of sports. Can you tell me why I have it? I went years with the injury before surgery, could this cause arthritis? My leg muscles have atrophied some bacause I’ve gotten less active due to pain, could this contribute? Any info you could offer would be apprieciated, I have a 3 yr old boy and hope i will be able to carry and run and play with him in the future.
Tim
Hi Dr. Howard
it would be good if you can shed some information about my current condition.
i just had an operation on my left knee (bucked head meniscus tear). and the doctor said it was fine and i can get back to soccer but probably not that often as i used to.
then i found out that 70% of my cartilage has been removed.. can i still get back to soccer??
i am 25 years old quite active player.. played 3-4 time a weeks indoor & outdoor.
Kind Regards,
Tim
Joe
Thank you for your time. I am 40 about 170 lbs. I am 8 weeks out from a medial menisus repair.
Went from no weight bearing to full weight bearing at about 4-5 weeks. Everything seemed fine but all of a sudden, this past friday morning i woke to excruciating pain and stiffness. Seemed to get worse as the day progressed to where there was sharp pain in the front joint line area. Very painful if i am not walking gingerly and slowly. Could i have done something the night before to mess it up again? The only thing i can recall is getting into a friends tall truck. I feel like just getting another MRI as i have a bad feeling about this. Could the stitches havd busted? Any info will be greatly appreciated. Very sharp pain along front joint line and at inside incision area. Stiffness and sore. Thank you
Joe, Tough call… Meniscal repairs tend to have a lower success rate as we age :-(. I can not offer medical advice via the internet or this blog due to privacy laws among others. What I can say is that, in general, if someone who underwent a repair starts having symptoms once again — and they do not subside, then a contrast enhanced MRI is usually the next step to see if the repaired meniscus is still in position.
Good Luck!
Howard Luks
Orthopedics, Westchester NY
http://www.facebook.com/Howard.Luks.MD
Chris
Hi Dr. Luks,
Thank you very much for your post! It is very informative and insightful. I currently do not have insurance. I am a 23 year old male college student. I am pretty active- exercising almost every day either by playing basketball or weight lifting. I have never had problems with my joints until about 2.5 years ago. I was playing soccer and as I went to plant my foot in order to turn direction toward the ball, someone mistakenly stepped on my foot. My body turned but my foot didn’t. Next day I could not lift my leg. After about a year of intermittent resting and still playing sports, I finally gave it the appropriate time to heal and was able to use my knee without pain in activities such as basketball and squatting. However, after about 4 months I somehow ended up damaging the meniscus on my other knee (right knee). I don’t know the exact movement or day it happened but even after much rest, it does not seem to improve like the other one did. To self-diagnose myself, I bend my knee in a squat type movement. As soon as I bend my knee even 45 degrees above horizontal, pressure starts building up on the joint which culminates, once in a deep squat position, in a feeling of large amount of pressure mixed with the feeling that something is being stretched past what it should be. Being 23 years old and active, having a knee injury annoys me to no end. Hence, I decided to do what I could to at least keep my leg muscles in shape- I started cycling some and doing body squats above parallel, along with a squat machine at the gym that manages to allow me to load my knee without any pain. Additionally, I have been wrapping my knees with elastic band, leaving just a small opening for patellar movement. What I find interesting, weird, and somewhat hopeful is that when I workout my legs and follow a warmup regiment that entails about 5-7 minutes of light cycling followed by 10 minutes of stretching, I am afterwards able to bend my knee without pain and even do a full deep body squat without the pain/pressure feeling I get typically. This only seems to happen when I do the extensive stretch/warm-up before hand. Additional to this, I have realized that since starting, I am feeling less and less of a pain/pressure when I load my knees (very light weights) doing lunges (which I couldn’t do before without the pressure/pain in my right knee).
After observing these things, I am a bit perplexed. I thought resting my knee would help it to heal and feel better. However, it seems that the more I left my knee without any type of activity/loading, the more it was subject to pain in even the slightest bending; alternatively, as I have slowly been working it out and increasing activity volume, it has begun to feel better. My biggest worry right now is that although it feels fine when I work out, I am actually doing more damage to my meniscal tissue. Based upon these observations, do you think the type of injury I have necessitates surgery, when available, in the future? Any insights, advice, questions, etc you have would be most appreciated!!
Thanks!
Chris
Chris, I appreciate your comments on the meniscal tear blog~!
Your are a very thoughtful young man. Since we’re not sure you even have a meniscus tear it would be even harder to determine if surgery is necessary and if so when.
In general meniscal tears in young folks are repairable… which means that we can suture the meniscus back together. The is far more preferable than removing the torn piece. Unfortunately, with time the torn tissue degenerates which could degrade the success rate of a meniscal repair.
I can not say based on the info given if surgery is necessary or not, but I sure would like to see an MRI.
Good luck … keep me informed… here or on Facebook.com/Howard.Luks.MD
Thanks
Howard Luks
Orthopedic Surgery Westchester County NY
Dan
I am 26 year old (male).4 week ago I met with accident and my ACL got damge. Orthopedic Dr. Suggests 4 week rest ,after 4 week rest now I am able to walk but unable to bend leg.
Dr. Suggested me 3-4 week excersize. After 4 week if there is no improvement then ACL surgery may require. Is surgery is only cure for ACL.
Can u pls tell me why m not able to bend leg, and how can this cure.Is ACL surgeryis require for this.
please suggest what should I do.It will be great help, thanks in advance.
If u need I can send MRI report also.
It is unlikely that the ACL is the reason you can not bend, and unlikely that it is a good reason to proceed with surgery. See this topic on ACL reconstructions… https://www.howardluksmd.com/education/common-injuries/anterior-cruciate-ligament/ THe most common reason for a locked knee is a unique meniscal tear called a bucket handle tear… or a large loose body. I would strongly recommend you try to get your motion back and see if you knee is unstable before considering ACL surgery.
Howard Luks
Orthopedic Surgery Westchester County NY
Amy S.
Dear Dr. Luks,
Thank you for this very informative site, I only wish I had run across it 5 months ago. I am a 57 year old female who injured my knee while kneeling for an extensive period of time at work, when I stood up I felt a sharp pain in my knee. MRI showed meniscus tears, loose body, and prepatellar bursitis. After 8 weeks of physical therapy I did feel some improvement but not to the point where I could walk or stand for any length of time. I ended up having arthroscopy in Oct of last year. I have completed 10 weeks of physical therapy and now have swelling, a hard lump over where the miniscus was repaired, constant stiffness, pain and my knee feels as though it is in a vice. My surgeon said I have bursitis, gave me a shot of cortizone and told me to come back in a month. The shot helped for 24 hours then the pain and stiffness gradually returned. I see my surgeon again in two weeks, his nurse told me that he will be releasing me to return to work. I have a very physical job which requires me to be on my feet up to 16 hours a day and have to push carts weighing up to 500 pounds. I am still limping, go down stairs backwards and know I am still unfit to return to work.
I need your advice as to how I should communicate with my surgeon. He seems anxious to be rid of me, after my last visit he took xrays and showed me where I have arthritis in the joint and that is causing the pain, it seemed to me like he was looking for an easy out and a reason to blame my problems on a different source. This arthritis never bothered me prior to my surgery and I was told by other dr.s that what I have is normal and minimal for someone my age. He is rated one of the top surgeons in my metropolitan area, I am fearing this next visit. His nurse told me the dr. said I am wll past the time for being healed from this surgery. Should I start looking for another orthapedic dr. or should I expect my surgeon to continue with my treatment. I wish I had never had the surgery, the pain I lived with before the arthroscopy was nothing compared to the constant pain, swelling and stiffness I have now. I hope everyone who is considering arthroscopy will look for other options before they rush into surgery.
Amy…
Thanks for stopping by… I appreciate your comments and I’m glad you found the mensicus tear post useful!
It’s hard to say why you still have pain… it could be the arthritis… it could be a residual tear or something we call post menisectomy osteonecrosis http://goo.gl/6hJFA . You and your physician need to be a team — you need to be able to work together towards a solution to your issue. If you find that the other side is not responding to you … or not giving you the attention you require or desire, then it is time for a second opinion.
I’m sure, with a little searching and effort you will be able to find a surgeon who is willing to work with you to identify the source of your current symptoms and the design a treatment plan to address it.
Good Luck!
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
David.T.
Dear Dr.Howard Luks
Thank you for this very informative site that i have read your article and the responses with great interest and I thank you for taking the time to address these questions so informatively.
I am 33 years of age, in which i sustained a supercondylar fracture of the left femur late 2006.
A left retrograde femoral nail was inserted into my patellor tendon to fix my fractured femur with
cross bolts intact into my left knee to hold the rod up.
In mid to late 2007 i had a cross- bolt removed because of slow union & ongoing pain with my rehab which it was flicking on my ITB. In early 2008 i had the femoral and the last cross bolt removed because of slow union and ongoing pain again.
In 2009 a MRI was performed which showed that i have patellorfemoral chondromalacia, also show’s an anterior lateral meniscal tear.
So than my surgeon performed an athroscopy to fix that, which now i have a degenerative knee and have more ongoing pain. I have had another MRI since and it show’s that my posterior horn & medial meniscal is torn with patellar tendonosis/ tendonopathy also mild osteoarthritis & mild thining with fibrillation of hyaline articular cartilage is noted at the medial femorotibial.
Also findings is a diffuse thicking of the patellar tendon.
My surgeon wants to do another arthroscopy to my left knee, i am not sure if i shound because i have had so many surgery’s in the past & would you think that i need an (TKR) very soon….. P.S Dr Luks…. Thankyou
David… Thanks for your comments…. I would first recommend another opinion. The changes in your patella tendon are from your prior surgery. You have not elaborated on your symptoms or when your knee hurts so I can’t say that the pain may be meniscal or not. Is the fracture healed? LEt us know what your second opinion says….
and feel free to stop by http://www.facebook.com/howard.luks.md to keep us informed.
Good Luck !!
Howard Luks
Orthopedic Surgery Westchester County NY
siya shah
Hi doctor!
I am a student and I am 22 years old. 2 years back I fell on a rock thereby damaging my knee. My MRI report says:
” Bony contusions at lateral condyles of tibia and femur. Posterior horn of lateral meniscus Grade 3 tears seen. Lipohaemarthrosis is seen in knee joint ”
My doctor gave me some medicines and I recovered within 2 months without surgery.
But after one and a half year I am experiencing little pain in my knee during winter. What shall I do? Do I need a surgery? Kindly help me.
shiji spencer
HI
Doctor,
i am a nurse in profession.i had a knee pain for last months continuously.before two weeks i consult an ortho surgeon and he advised me to take MRI.the report told that i have a posterior meniscus cleavage tear and low grade interstitial tear in ACL.What i hve to do?
Raj
Hi Dr Luks
Than you for your informative website and forum. I am hoping you can give me some general advise wrt my injury. I got knee pain while running about 5 weeks ago. I have been seeing a physio but because the knee wasn’t settling I got a MRI done last week. The finding was ” a predominantly radial tear extends from the free margin to the peripheral third of the mid body of the medial meniscus, with no associated displaced fragment”. There were no other issues from the MRI. I am 38yrs and have been fairly active in sports. Is this something that will settle over time or will require surgery repair/removal of tear. If surgery is required, can I return to running?
Thanks.
Raj… While the radial tear of your meniscus will not heal… the pain can settle down to the point where you can return to an active lifestyle. As I frequently say, the desire to have surgery should be based on the effect that the pain is having on your quality of life. In orthopedics we typically treat pain… as such it should be the patient who ultimately makes the decision. Most patients are able to return to running after meniscus surgery, especially if no arthritis is found.
Good luck!
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
Ruairi
Hello Dr. Luks, thanks for hosting conversation above.
I equally have meniscus problems (I think). If you have time to give my opinion, I would be grateful.
I’m male, 45, 175 lbs. A lifelong soccer player, cyclist, runner in my later years up until two years ago when everything came to a dead stop, after I had to break off marathon training with knee issues.
After initial consultation with a doctor and ultrasound, I was diagnosed wth tendinitis in my right knee. As one leg was found to be shorter than the other (abut 3 mm), it was suggested that I insert lifts in one shoe. With this, I tried to start running again during the next year but it was never really viable.
At some point, I developed a limp on my left leg. The symptom was pain while walking in the knee joint. It felt like my knee was unstable at one particular point during a normal gait, and I had a searing pain on the inside of my knee along the line of the joint, especially when I apply twisting motion, like turning a corner or turning away from the fridge for example.
After more consultation, I was sent for an MRI o my left knee. Result came back to be (i) a degeneration of the meniscus (with no specifics of the degeneration, I assume thinning, but no features identified), (ii) a medial condyle edema.
Knee specialist said to wait for a year as edemas take 6 to 12 months to heal.
This is 12 months later. The pain during walking is gone (95%’ish), but the pain on turning around a corner on the inside knee is still largely there, somewhat diminished in intensity, but fairly stable now. To avoid pain when turning turning, I feel like I have to straighten my leg and turn at the hip.
So, everything I’ve read says that the edema should be gone, which is why I don’t have pain on walking, or could it still be there, after so much time ? Could the pain on the inside of the knee be associated with the edema or does it have to do with the degeneration, or could it be something else?
My running career is finished, I wish to keep whatever meniscus I have intact, but I would like to be able to hike, or walk for distances without feeling pain.
Yours gratefully, Ruairi.
Curtis
Dr. Luks,
I had a torn meniskus repaired about 4 months ago. I had it done because I was in terrible pain and could barely walk. Each time I put weight on my knee, it hurt severely. The pain begain to deminish slightly before the surgery, but I opted to get the surgery.
Anyway, I tried physical therapy for a short time and it hurt, so I didn’t do it anymore. It has now been 4 months since surgery and my knee hurts almost as much as before surgery. Every time I put any weight on the knee, it hurts enough to make me flinch. Every step I take hurts.
Also, when I have been sitting for a while and stand up, my knee does not want to straiten. It takes a couple minutes before I can feel comfortable straitening my leg again. And then it still hurts once I start walking on it. Each time I put weight on my knee, it really hurts.
What sort of non-surgery options do I have to resolve this? How long will the pain stay around? Do I need another surgery, or will the next surgery just make it worse?
I weigh 335 lbs and am 6′ tall and 43 years old. Sometimes I wonder if just getting a knee replacement would be the answer, because It just feels like there’s broken glass inside my knee joint every time I put any weight on it.
Any advice, and wisdom you could share about this would be greatly appreciated.
Thanks so much,
Curtis
Gregory
Good day. I would love to thank you Dr. Luks for your wonderful website and for your time and help you provide for us, readers. I was an athlete until a year ago when I had my first injury which put me off for almost a year. As soon as I recovered I got back to my sports and got back to the level at which I was before. I was leading a normal life, eating healthily, exercising obviously and all was fine until one day (16th last month) I was walking home from work and all of a sudden my knee started to hurt quite sharply. The next 10 days I spent in pain and when I was going up or down stairs the pain would be a lot more pronounced. I went to see the doctor who treated a friend of mine with the same problem and he said that it was a meniscus tear. My friend completely recovered and does not complain of any pain. He did not undergo any surgery. I really do not want to go for a surgery and hope for a full recovery.
This particular doctor told us to take Glucosamine Sulfate 1500MG a day and I would really like to hear your opinion on this particular supplement. I also would like to hear your opinion on using braces and tight bandages for the knee while it is healing as I would like a second opinion.
Thanks a lot
Greg
Greg… thanks for the kind comments !!
Here’s some info that was just published on Chondroitin Sulfate … http://onlinelibrary.wiley.com/doi/10.1002/art.30574/abstract but it speaks to improvement of pain scores in patients with arthritis… Nothing wrong with waiting things out … trying physical therapy and see how your knee feels in a few weeks. If your symptoms persist, a quality exam and possibly an MRI will be useful.
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
Ashley
Hello Dr. Luks,
First off I would like to thank you for this very informative site and the advice you are giving to help others, (hopefully) including myself! I have been having knee pain for some time now and would like to see if I could get your input on my situation. I had an ACL repair back in 2007 in my R knee so I am familiar with how painful post op surgery can be. I went to my orthropeadic and he said I suffered from patellofemoral pain.I went and had an MRI on my L knee after putting up with the pain and swelling for a prolonged period of time, and the results are as shown:
There is a mild lateral tilt of the patella w/ mild lateral patellar subulaxtion. Extensor mechanism remain intact. No abnormal plica. The articular cartilage at the patellofemoral compartment is also preserved throughout.
There is a focal vertical radial tear defect at the free edge of the lateral meniscal body spanning approx. 4-5mm. Medial meniscus remains intact. Intact cartilage in the medial and lateral femorotibial compartments. ACL & PCL are intact. The medial colateral & posterolateral corner stablizers are intact.
There is a small joint effusion. There is a 10mm x 7mm low signal band of tissue which extends from the Hoffa’s pad into the anterior margins of the lateral femorotibial compartment possibly representing focus of scar from chronically impinged fat or synovial tissue. No stress fracture or osteonecrosis. There is a 4cm x 1.5cm bakers cust. There is an upper limits of normal sized lymph node in the popliteal fossa which demonstrates short axis measurement of approx. 9mm.
The imperssions were the 1.focal radial tear 2.band of scar tissue and 3. mild tilt of the patella.
I merged away from the option of surgery at first and started with the PT instead to see if that would minimize the pain and get the kneecap back into place. After about 2.5 months of that (1-2x/week) I stopped and I am still in pain as it comes and goes. I am physically active. Gym 4-5 times/week and would like to get back into playing basketball & softball (knee permiting) I feel a small bulge on the back of my knee, that can sometimes be extremly painful, and the other pain is around the anterior of the knee and along the IT band. My surgeon recommended he do a lateral release. Your thoughts would be greatly appreciated, and I apologize for the lenghtness of this post! Thanks again!
Ashley… I appreciate you reaching out… We are not defined by our MRI findings… https://www.howardluksmd.com/orthopedic-social-media/treat-patients-as-people-not-diseases/ . That said… it is impossible for me to even postulate what is bothering you simply because you havent indicated where the pain is, when it occurs, etc…. I treat patients :-) Not MRI findings…. a little more history might help me guide you.
Thanks again for stopping by…
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
Ashley
Dr. Luks..Thanks for such a speedy reply. I have some pain when going down steps, its mostly on the front side of my knee. At times when im doing cardio, like on the ellipitcal or treadmill I have a “popping” or “cracking” sensation. I usually just push through it and ice my knees when I get home. Often times it is the day after when the pain really gets me. Sometimes it will wake me up during the night. I have noticed that I get extremly uncomfortable and my knees start to bother me if my leg is fully extened for a prolonged period of time, or even when I am sitting for a long time (work, school, flying). Some days I can go with no pain or discomfort at all, and other days it hurts me to even walk. I can also pinpoint where i usually have pain on the distal end of what I believe to be my IT band, but of course this is hard to explain via words! Overall, the front and lateral side of my knee is what gives me the most discomfort. Also, it might be helpful to add that when walking for a while at a steady pace I can feel the “bulge” on the back of my knee getting inflamed and is sometimes tender to touch when it it is. I also can not tolerate squats, the pain hits the worst on the front of the knee as well. I hope this helps you a little. Thanks again for any help or advice you can provide.
Again, I tried PT for roughly 2-3 months, have been prescribed voltaren-xr, and ice regularly after exercising, swelling was a major issue at first, but it has been very minimal lately.
Ashley
Dr. Luks..Thank you for such a speedy reply. Most of my pain comes from going down stairs. I have also noticed that when my leg is fully extended for a long period of time I get extremly uncomfortable and experience a lot of pain/discomfort. I also get this pain when I am sitting for prolonged periods of time (school, work, flying) Most of my pain is on the front side of my knee. I can also pinpoint the pain on the distal end of what I believe to be my IT Band, of course it is difficult to explain exactly where this pain is via text. When doing cardio (treadmill or ellipitical) I sometimes have a “popping” or “cracking” sensation. I often times just push through this and ice my knees once I get home. After walking for a long period of time I can feel the “bulge” behind my knee getting inflammed and it is sometimes tender to touch when it is. Overall, most of my pain is on the front and lateral side of my knee. I have my good days and my bad days with my knee. I cant think of anything that I am doing to onset my discomfort, as it sometimes wakes me up in the middle of the night. I absolutely can not tolerate squats as it leaves me in an extreme amount of pain on the front side of my knee.
As stated before I did PT for roughly 2-3 months, ice regularly, and have been prescribed voltaren-xr. I did have a major problem with swelling, but that has been very minimal lately. Again thanks for everything and any advice/help you can provide!
Ashley
Joelene
Dr Luks,
3 wks ago i tore my acl, meniscus, and mcl. I could not have surgery right away due to a blot clot. Since the accident, i have fallen three times due to my knee giving out. When this happens it feels like my bones pop out of place and back in, and it is extremely painful. I am very worried this has caused a lot more damage. Would i need another MRI before the surgery? And Im not sure how to prevent further damage? My doctor wants me walking around with a brace to strengthen my muscles before surgery but sometimes when i come down wrong on my foot the knee gives out.
Joelene … that is a tough combination of injuries. This video will give you a quick look at knee anatomy so you know what is going on. https://www.howardluksmd.com/knee-faq/knee-anatomy-video/ Immediate surgery is usually only indicated if the MCL tear was “complete” or what we call a grade III injury. Otherwise, MCL injuries hurt for a lonnnggg time :-( If you have the ACL reconstructed during that time it will make it very hard to rehab from you surgery. That said, stability is an issue. You must be braced… and consider using a can or crutches until your leg is stable enough. Prehabilitation ( https://www.howardluksmd.com/knee-faq/do-i-need-therapy-or-rehabilitation-before-knee-surgery/ ) is very important in these cases. If a brace, crutches or cane and therapy do not improve your stability you may be forced into considering surgery sooner rather than later to minimize the risk of further damage https://www.howardluksmd.com/education/common-injuries/anterior-cruciate-ligament/ . Typically a new MRI is not needed because we see everything at the time of an arthroscopy.
Good Luck
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
Marilyn
Dr. Luks,
I found your site today. Thank you for the time you take to help others!
I am a 55 year old woman. I have had several falls the last few years, always landing on my knees. Each time the pain was severe enough I did not think I would be able to get up. After a couple of minutes I was able to get up and surprisingly had little pain, just stiffness and some swelling, especially in the right knee.
About a year and a half ago at a physical the osteopath noticed swelling in both knees and ordered x-rays. She said both knees were a mess with arthritis present in both and I was probably looking at eventual knee replacements. She did say there was still some space present which was a good thing. When I told her I really had little or no pain she said it could obviously wait.
Several months ago my right knee began locking. The pain was severe but immediately ceased when it came unlocked. It only happened when I was sitting with my legs crossed and I quickly learned to not sit in that position. No more locking until several weeks ago. The right knee again began locking but I could not pin point what was causing it. As before the pain was severe while it was locked. I learned to slowly turn my foot from left to right and it would unlock. However there is now a residing pain behind the knee on the right side.
I returned to the doctor who sent me for a new x-ray and referred me to an orthopedist. While waiting for the appointment my knee began locking even during sleep. The pain and unlocking would wake me and the pain behind my knee would be present all day. I does not happen every night but is often.
I saw the orthopedist yesterday and he asked for my story. After telling him what I wrote above he said he was certain I had a lateral meniscus tear and surgery would take care of it. My concern is that he did not do any tests to determine range of motion or even ask for an MRI to see how much damage there is. I told him I would like to wait until June for the surgery as I do not work during the summer and the four weeks he suggested on crutches would be impossible in my current job. I work up two flights of stairs and am up and down several times a day. He mentioned how the military consider meniscus an urgent surgery so the tear does sever completely, resulting in removal of the whole meniscus. I asked if there was anything I could do until June to keep this from getting worse or anything to better the situation; ice, elevation, rest…He said nothing would be beneficial until I had the surgery.
I would like to know if the MRI is necessary and if there is anything I can do to prevent further damage. I am wondering if I should also get a second opinion.
I would value your input.
Thank you,
Marilyn
Thanks for your kind comments… and thanks for stopping by.
The first thing you need is a second opinion… I can not speak for the military, but academic orthopedists (those of us privileged to treat the next generation of surgeons) do not consider meniscus surgery to be urgent in nature. But the bigger issue for you is the arthritis. This is a very controversial area. When you have osteoarthritis you have lost cartilage in your knee. That cartilage can not be reconstituted or rebuilt. If you have mild or moderate severity arthritis then an arthroscopy for a documented meniscus tear https://www.howardluksmd.com/education/common-injuries/meniscus-tears/ might help your symptoms of locking…. but patients with severe arthritis might also experience locking symptoms as well. Therefore… if your locking persists, imaging will be useful to aid in determining the severity of the arthritis and the extent of your meniscus tear. If you do not have a large unstable flap tear of the meniscus, it is unlikely that it is the source of your locking. If you have severe arthritis with complete loss of cartilage in areas of your knee then that can cause locking… and will generally lead to a poor result following an arthroscopy.
An MRI would be useful in this situation… as would a second opinion.
Good Luck
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
NamePhylis Bernstein
Hi Dr. Luks:
I found your website and find it so informative—-thanks! I fell d have a lateral tibia plateau fracture (which fortunately didn’t require surgery) and a lateral meniscus tear (both according to my recent MRI). I had slipped and fallen in the bathroom.. My knee was swollen for about one week, but after icing and advil it is back to normal. The orthopedist put me on crutches and a short knee brace and I was told to stay off it for two weeks—-I go back today. I am a 2nd grade teacher so I stayed home. He mentioned arthroscopic surgery as an option at my initial appointment saying that my knee also has signs of osteoarthritis. (I have it in my toes and a finger—but I lead an active lifestyle and it doesn’t bother me). I would like to try physical therapy and practically anything so I can return to work and physical activity and am reluctant to have surgery, unless absolutely necessary. So my question is—-what would be your suggestion ? I will pursue a second opinion too—the orthopedist is very kind, but very busy, so a lot of my questions will probably be unanswered today when I go to see him. Again, thanks much
Any reasonably good Orthopedist is busy … if they’re not willing to give you the time to answer your questions during discussions about treatment alternatives, imagine how hard it will be to reach him/her after surgery ???
Anyway… not all meniscus tears require surgery — as long as you do not have instability, buckling or giving way and the knee feels stable there’s nothing wrong with trying a month or two of physical therapy to see if your symptoms improve. The decision to proceed with an arthroscopy for a meniscus tear is usually based on your quality of life ~!
Good Luck
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
Mark
Dr. Luks,
Thanks for the video. I’ve just started, two days ago noticing pain when I squat all the way down (or maybe a bit before all the way) almost on the outside left bone of the knee/just below. I did jump rope last night just fine, with tremendous about of lateral movement.
I have no problem getting up out of a chair at this point. But something is going on. I do not remember any specific event or moment, but that doesn’t mean it just happened at some point and I didn’t notice it enough to say, “Wohhh, What just happened/”
What’s your best “non-medical advice ;)” opinion as to what’s going on?
Thanks,
Mark
My Pleasure Mark….
Tough to say what’s bothering your knee… too little info and no exam :-(
It could be a slight strain, it could be a small meniscus or cartilage injury. It is not bothering you much —- so I would wait this out a bit and see how the knee progresses over the next few weeks. If an issue persists a good exam should be able to tell you what’s going on.
Good Luck
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
Mark
Thanks Dr Luks…
Follow up question: If I notice it feels “better” overall, does that generally mean it’s not serious?
But my assumption would be, even it feels generally well…for example I jogged from my car into the grocer yesterday (straight ahead) no problem….but if I squat down and still have sharp pain, then something is structurally damaged.
I’m very fit, – no belly fat or excess weight of any kind. So that’s no an overriding issue. I am 42.
Mark
Mark
Jeff
Dr. Luks,
I am 43 y/o firefighter in California and work a very demanding schedule and job. I injured my right knee on 8/21/11 saving a man that had gone over the side of the road in his car about 400 ft down a canyon. The pain in my knee had no relief so I went for the MRI. It shows a horizontal cleavage tear, my knee is stable, no pain walking or turning, pain gets worse only when running, maybe a 4 on 10 scale. It does feel like it is getting better, can you please recommend surgery or not? Thanks ahead of time, Jeff
Firehouse 54
Ventura County Fire
Dr. Hamdi
Dr Luks,
I hope this message find you very well.your website is considered as a reference for all orthopedic whom need your valuable and enriched experience for their decision making.After i read your all posts ,i think you need to list all of them in one booklet which can be a reference for all knee injuries and joint performance.I hope that,
My Professor,I am an ER Doctor and now 35 years old.I had got a right knee joint pain for a long time most probably 10 years ago.to get rid from this pain,i were using a billow under my right feet while sleeping .it gives me good relieving when i awake up.never use analgesics or NASIDs.
Last month,the pain and tenderness increased as i made a lot of efforts.so,i made MRI which showed that :( Presence of degenerative changes in the posterior horn of the medial meniscus with small effusion.Rest of the examination is normal).
Some orthopedics consultants said you need meniscal repair and others said no need.few of them recommend physiotherapy.??????/
Now,my all problems that minimal medial pain and sometimes creptius sounds when suddenly flex or extent my right knee joint.i start to take myself Glucosamine sulphate 500mg and i dont know if that right way or not.
Kindly,i need your final opinion, and if this site of tear in the red zone .so,healing is expected?
I know i disturbed you by this long message but forgive me ,My future job is threatened as we working some times more than 12 hours in ER.
Thank you.and always,Your effort is highly appreciated.
Dr.Hamdi
I would not rush into surgery in your case… as I discussed in my last answer to your post. I would consider physiotherapy first and see what happens. Thanks for your thoughts and comments about the information here on meniscus tears and whether or not surgery is necessary.
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
Dr. Hamdi
Thank you for your reply.i will start physiotherapy soon and update you with the outcome.
Kavita
Hello Dr Luks,
Thanks for your reply. We are really happy to learn that the meniscus tear is not that bad. He does not feel loose knee anymore but he is not very active either. We are going for the surgery on 2nd feb. We have good references about the arthroscopic surgeon and I am praying that everything goes well.
Thanks a Lot.
Kavita
New Delhi
India
Heidi
Hi Dr. Luks,
I developed lateral knee pain that is exasperated by lateral movements or twisting motions. This got so bad that I had to stop making lateral movements in my activities; both exercise and daily living. Two doctors thought I had a meniscal tear, however, there were NO findings on MRI. I began physical therapy and have gone for almost 2 months. I am no better off, and in fact, my pain has increased some, and occurs sooner in my activities with less motion than before.
Is it possible for the MRI to totally miss something important? And also, is there more sensitive imaging that can be done? My orthopedist initially suggested a possible diagnostic arthroscopy, but he didn’t feel there was much point to that since the MRI was negative. My leg strength has improved with therapy and is very good. I work out (avoiding painful moves) and have strong legs, so it’s not a muscle weakness issue. I see my ortho again next week.
Heidi… Thanks for stopping by. Lateral knee pain can occur for a number of reasons … the meniscus is not the only reason. Can MRI’s miss a meniscus tear? Well… the MRI might not miss it, but the radiologist might. Consider getting a second opinion on the MRI itself. Other less common causes of lateral knee pain include ITB Friction syndrome, “instability” or degeneration of the popliteus tendon — both of these issues usually resolve with an injection. There are other less common causes… but I would start with a second read on your MRI (they can also look for ITB thickening or popliteus tendinosis) and perhaps yet another opinion by a sports doc.
Good luck
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
Kavita
Hello Dr. J. Luks,
Your website is just what a patient needs at the depressing time of Meniscus/ACL injury. I felt that a patient could learn more from your website than the doctor.
My fiancee suffered a knee injury during a badminton match on 8th Dec 2011. He felt popping out of the knee but a doctor was unavailable so he only took bedrest and could consult the doctor only after 2 days.
The finding of MRI is as follows-
– ACL tear with anterior tibial subluxation of 8.0 mm.
-Intrasubstance hyperintensity in posterior horn of medial meniscus extending upto the inferior articular surface suggestive of closed grade 3 tear
-Hyperintensities in lateral femoral and bilateral tibial condyles suggestive of bone contusions.
-Mild joint effusion.
There was severe pain in the knee but no swelling. He has been applying RICE and was on deadrest for almost 1.5 months. He used to wear knee cap and use crutches while walking. From last 2 weeks he has started to walk without crutches and feels pain now but there is no popping.He went to physio but could do only litlle exercise and even cycling was not possible.
We have consulted 2 doctors and one says he should go for arthroscopy while other doc says no need.
He is very active and plans to join Police service hence his life is going to be very active.
From some friends he has learned that sometimes Meniscus and ACL tear never heal properly even after surgery and person is never able to walk properly. As it is his dream to join Police services he is getting depressed that he might become physically unfit for forces. This very thought scares both of us. He might have to joing by August- September 2012.
What is your opinion on this? What is more serious ACL tear or Meniscus tear? Is it true that Meniscus can not be reconstructed or replaced? Our doc says that the torn part of meniscus has to be removed?
Will he be able to resume normal activities including running by september 2012?
Your opinion will be really helpful.
Thanks
Thanks for your question Kavita….
Your fiance seems to be having more of an issue with his ACL tear. His meniscus tear does not sound like it is “bad”. He may not even have a tear with that reading. His issue appears to be his ACL, but 6 weeks later I would expect his motion to be improved —although he may feel that the knee is loose or unstable. If he feels the knee is loose or unstable he can use a brace so he can rehabilitate the knee properly. Patients with an unstable knee due to an ACL tear usually opt for an ACL reconstruction. If properly performed, and no complications occur, most patients are able to return to an active lifestyle… including joining the police force.
Good luck…
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
Dr. Hamdi
Dr.Lucks,
Kindly,i sent you my inquiry regarding my knee problem.
Thank you and your effort is appreciated.
Dr.Hamdi
JoAnn Straglinos
Dr. Luks,
I watched your video and it has me thinking. I went to get my MRI results yesterday and they said there is an irregular tear involing the posterior horm medical meniscus extending to the root, thinning of the anterior cruciate ligament. The doctor was quick to schedule surgery but I have no pain or sweling and have been going to the gym. I am a runner but have not been running .
For a complex tear is surgery really necessasry.,
chelle
hello, dr luks.
i’m chelle and i just found out from my mri results that i have (1) complex tear in the anterior horn of the lateral meniscus w/ separation of the anterior transverse ligament; (2) partial tear in the superior lateral retinaculum; and (3) minimal intra/periarticular joint effusion. i was diagnosed with discoid lateral meniscus (i had a positive result with the mcmurray test) prior to requiring me of having mri.
i’m lucky enough to have come across this website of yours as i don’t wanna go back to my ortho because i was already told that i may be up for knee surgery sooner or later. i’m quite relieved that you mentioned in your about page that “I want patients to understand that not all MRI findings require surgery…”
i’ve already given up my hiking and mountaineering activities and even jogging. do you think my condition can improve without surgery? sometimes i do feel sort of tension or tightness on my right knee whenever i go up and down the stairs and even when simply “putting” my legs to “resting” position after crossing legs.
thanks in advance, dr luks!
this is such a great help.
God bless you more!
Dr. Hamdi
Hi Dr.LUKS,
I hope this message find you very well.Actually, this page is of high valuable and golden feedback about the Knee joint problem.I searched many times on the internet to find the answer to my knee problem but was useless.Here,i found realistic and logic comments which satisfy the majority of the patients needs.Hereby DOC,I am 35 years old,had a right knee dull aching pain for a long time before and i used to put a billow under my right ankle while sleeping.1 month ago,i felt abnormal persistent pain on the medial side of knee in which i can tolerate and sometimes Rt.knee crepitus.The main problem when i am walking for long time as i fell spasm of popliteal muscles and obligate to sit down for a while. i made MRI Right Knee showing (presence of degenerative changes in the posterior horn of the medial Meniscus with small quantity of joint effusion and the rest of the examination is normal)kindly,i seek your advice Dr.Luks as my job is ER Doctor and this can affect my future career .some orthopedics suggest physiotherapy to support the thigh muscles to ease the burden of the knee joint and others said Arthroscope menisical repair.
Thank you and your opinion is highly appreciated.
Dr.Hamdi
Thanks for the question… first … I apologize for the late reply. Your comment found my SPAM folder :-(
Your MRI does not show a meniscus tear… degenerative signal is seen in most menisci on an MRI. I would only consider surgery for a true tear, and only then if my pain persisted despite non-operative measures, or if I had a flap tear or very large tear.
I agree with the suggestion that you start physiotherapy… it can be very effective at alleviating knee pain when there is no “mechanical” source of pain. I would also consider NSAIDS for a week or two, to diminish the effusion.
Good luck and let me know how the physio works.
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
Mark Stockman
Dr. Luks, thank you for this very informative web page.
I have a question re a meniscus tear. I am 57 and very active. I have had pain on the inner side of right knee joint for about a year and a half. It came and went. Sometimes it was very sore and sometimes not. It did not hamper my activities. My physical therapist did not beleive it was a cartiledge issue. Recently, past 4 months or so, My knee feel like it cathes slightly or better put, at extreme end of motion sort of bumps over something. It is not really painful. I went to my ortho and he had an MRI done and said there is a small tear on the inner part of my medial meniscus in my right knee. He said I am tolerating it well … no fluid on my knee etc. He indicated there is no hurry, but It would be a good idea to have surgery (scope) to shave the tear. He thought i would lose about 20 % of the meniscus. If we do not do the surgery the risk is that it may tear more. It does seem that the “bump” is getting more exagerated with time (very slowly ). What would you recomend? It is possible to repair at my age? (my understanding is that at my age the blood flow to the outer 1/3 is relatively poor and repair is not recommended). IS there anything else I can do (eg I have read that there is some cartiledge regeneration techiques)? Thanks for your help. Best, Mark Stockman
P.S. I believe my surgeon to be very competent and caring .. I am just interested in a second point of view.
Mark…
sorry for the delayed reply…. your original comment was snagged by the SPAM filer :-(
I find it very hard to imagine that a small tear is causing the “bump” within your knee. More difficult is that I can’t examine you to confirm that the meniscus is the source of your pain or symptoms.
I am not a fan of “operating so it doesn’t get bigger” At your age the meniscus is not repairable… and cartilage regeneration generally refers to “articular” cartilage, and not meniscus cartilage. There are occasions where we transplant new menisci into knees… but that is typically done for people who have lost most of their meniscus.
The decision to undergo surgery should be a quality of life decision… not a what if decision.
Good luck
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
hatem
Hello Dr. Luks,
What an amazing and informative link! Thumbs up all the way…
I am a 46 year old very active male, I tore the medial meniscus of my left knee when I jumped and landed on one foot, while having a boot camp class. that was 3 months ago. felt sever pain when the incident happened which lasted for a week, so I went to an orthopedic surgeon who advised me to do an MRI to confirm his suspicion that the meniscus is torn. the MRI showed ” a large complex tear of the medial meniscus” now the surgeon is suggesting an arthroscopy!
I started my research to learn more about the surgery before I take my decision, and only then I came to ur fantastic page which made me decide NOT to go for the surgery as the symptoms almost disappeared after 6 weeks and i gradually returned to my workout, and so far so good, i now do the cross machine, run, do body pump classes ‘no weights on squats’ I feel fine, with little to no pain during the activities, i may even flex my knee to my butt.. but i still am afraid to go to the extreme workouts that i use to do before the incident.
my question to you is, do u think I may start my extreme boot camp classes, hiking trips, horseback riding, cycling and climbing? What is holding me from ths is my mind so far and nothing else…
thanking you in advance for the fantabulous page, Hatem
Hatem… I’m so happy to hear you found the page on meniscus tears useful and informative. The end goal of the non-surgical treatment is that you are able to return to your desired level of activity. No reason not to try to return to activities you enjoy. IF you are able to, it is likely that surgery is not necessary. IF you are not able to return to those activites then you have a choice to make. Change your knee to suit your life, or change your life to suit your knee.
Good luck and thanks for the kind comments.
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
resor island
hi! ;) im at the office at the moment, thus i don’t have very much time to write… nonetheless! I really liked reading through the article. It was some great stuff. thanks! All the best, Bunce
Amanda
I have a question in regards to an MRI I just had. I fell down some stairs around 1998-99 when I was in the service. I have had problems off and on but more now then ever. This is what the MRI stated:
FINDINGS: A large radial tear in the anterior horn of the lateral meniscus with suspected chronic injury to the lateral collateral ligaments and promximal tibiofibular joint.
Can you explain this to me and is surgery an option??
Thank you!
Amanda….
As I mention in many of my posts… physicians should endeavor to treat patients and not their MRI findings… the premise of that is simply that the same tear or problem will not affect all individuals the same way. The indication for surgery in NOT simply that a tear exists, but that it is painful and interfering with your quality of life — and a trial of non-operative management has failed. Proximal tib/fib joint injuries can cause snapping, popping or pain too… so this brings to light the fact that you need an accurate diagnosis based on a comprehensive physical exam. That will be able to tell you whether or not the tib/fib joint and or the tear are the source of pain… then you determine what the possible treatments are —and take it from there…
Good Luck
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
Vin
Hello Dr. Luks,
I had a twist of my knee and a fall while playing badminton. I was on rest for around 2 weeks. Once the pain subsided I started playing football and later encountered the problem of knee locking. Later I took an MRI and the Observation is as follows:
Complex vertical tear of posterior horn of medial meniscus & reaches upto both superior & inferior articular surfaces
Chronic full thickness tears of Mid fibres of ACL. Loss of normal dark signal and loss of continuity of at the fibres noted.
Underlying bones including the lower end of femur,upper end of tibia and fibula and the patella appear normal. No evidence of bony destruction or marrow signal intensity changes identified.
Small amount of fluid seen in the joint space.
The lateral meniscus appears normal with no evidence of degeneration/tear seen.No evidence of meniscal cysts identified.
No loose bodies identified.
Underlying soft tissues appear normal.
PCL, the collateral ligaments and patellar ligaments appear normal.
I consulted 3 doctors and all of them were giving different opinions regarding ACL tear. They were agreeing on removal of meniscus. Since I have stopped badminton and soccer, I dont experience Knee Locking now-a-days.
Will there be any problem if I dont conduct the surgery? The Doctors were of opinion that my hamstring is strong enough to cop with the ligament issue or hamstring has accustomed to the ligament issue.
Awaiting for your precious advice..
Regards,
Vin
Vin, Not everyone who has an ACL tear requires an ACL reconstruction. If your knee buckles or gives way, then you can consider it, or alter your lifestyle. With regards to the meniscus tear. If your pain is interfering with your quality of life, then surgery may be indicated… if the pain is not too severe you can see if your symptoms improve spontaneously, or you can choose to go ahead with treatment of just the meniscus tear.
Good Luck
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
Name Gary DeSha
Dr. Luks,
I’m about two weeks into my left knee pain and swelling. Two weeks ago or so, a friend and I were moving heavy items up and down my basement stairs (4 trips) and loading them in her car. The next day my left knee began hurting; the following day the pain increased and during the weekend my knee began to swell. I iced it, wrapped it for a couple of days, but the wrap was making the rest of my leg below the knee swell, so I removed it. My office is down stairs in my basement. After I sit at my desk for a while and take a break, as I stand it is very painful and hard to walk. While standing the knee will not go back naturally like my right knee does. It hurts the knee to stand on it for a long period or to walk on it for long periods, like going grocery shopping. It is difficult to put shoes and socks on that leg because of how you angle your leg to put a sock or a shoe on…very painful. I have been icing it about twice a day, trying to keep it extended and elevated somewhat too. I have been taking motrin (600 mg) a day, no more to control the swelling and stiffness.
I went to accute care, had an x-ray which showed nothing. I had to wait almost a week before I could get an advised MRI. I am waiting and wondering if I should visit an orthopedic surgeon.
The accute care physician called me and gave me this report:
“Medial meniscal tear. Unstable appearing inner margin of central aspect of posterior horn.”
Understanding your disclaimer, what do you say?
Thank you!
Gary …Sorry, sometimes I get behind in my replies, and I apologize. Your case sounds like something we call a “displaced bucket handle tear”. That means that the meniscus has torn and flipped into the middle of the joint. When that happens, the knee cannot extend to a fully straight position. Unless the meniscus flips back into position on its own, and if an MRI confirms this, then many people will end up requiring a repair of the meniscus.
Disclaimer is implied…
Good Luck,
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
Michelle Funk
Hello Dr. Luks
I’m a 30 year old active women and I went to Orthopedic Surgeon because my left knee has been bothering me. I love to run and its extremly painful for me ,so I have not been running. I have popping, knee gives out, knee locks up, I have to “pump it” I call it to make it pop and then it feels better, and when it pops sometimes painful, aches but not all the time. He said I probably have thinning cartilage and torn meniscus. I had X-ray and he said looked fine. He ordered and MRI and I had that today. I go see him Thursday for the results. I never had a MRI before and was wondering why I’m in so much pain today?? Painful to walk and feels achy just lying on the couch. My knee felt pretty good before I went for the MRI. During theMRI I was in so much pain I asked if I could stretch my knee and the tech said no she had to keep me still and only she had like 4 scans to go. It took like 15mins for those 4 scans, so uncomfortable I just went with it and I had tears for the longest 15 min of my life.
Thanks Michelle
Michelle… Sometimes tears are quite painful, and sometimes they’re not… it depends a lot on the type and location of the tear. With some flap tears or tears that are “displaced” from the normal position of the meniscus, you will experience significant pain with the knee in the straight position.
Good Luck!
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
Agustín
Hi Dr. Luks,
I am a 37 year old male and engage in rock climbing and mountain biking several times a week. During a rock climbing session while stepping on my right knee I experienced a sharp pain inside my knee which got better after a couple of weeks of RICE and recumbent fixed bike exercise. I did not suffer from inflamation, locking or instability – just clicking. Then I got to the gym and went for a climbing session and the pain came back worse than before. Saw an OS in a sports medicine facility here at work and he indicated x-rays and MRI but even though he did not see tenderness in the joint line I felt mild pain during a McMurray test. He is guessing a lateral meniscus tear…
1) I need to sort out my insurance before I tackle all studies and possibly surgery, it is Nov15th now and the initial injury was on Oct22 – can I wait until Jan1st (2month after the injury) and still have a shot at a successful repair (should the tear be repairable)?
2) Is there any pre-hab I can do before in the meantime? should I wear a knee band of some sort?
3) As a general rule – if one wants to stay active – do you recommend any supplements?
4) (wishful thinking) Are there any other knee malaises that look very similar to a tear that are not a tear? Is there anything in the way of insufficient stretching that can make a tear evident or elicit simptoms like a tear (with no mechanical symptoms).
Thanks so much for your help,
-a
Agustin… The story you give is not entirely suggestive of a tear… although it is possible… Other cause of lateral knee knee pain include ITB Friction Syndrom (Tendonitis/Burisitis) — primarily due to overuse.
There is no reason you can not remain active within reason… I would not put myself on a rock face until I know that this is behind you to avoid potential bodily injury :-(
If your symptoms fail to improve over the next few months, you can seek the attention of a doc and perhaps an MRI will be useful at that time… no harm in waiting a few months.
Good Luck
If you like… feel free to reach out through this site where we can have video discussion regarding your knee. https://2nd.md/profile/howardluks
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
Yanche
I am 52 years old 6 feet 250lb. I recently played soccer and experienced some very nasty sharp pain on my left knee starting the very next day. I went to the regular doctor who thought I have gout: after a week of some medication I had no improvement. So, I had an MRI with the following conclusions:
1. Small effusion
2. Complex tear of medial meniscus
3. Probable small linear tear at the body of lateral meniscus
4. Grade II strain at the MCL
Is there any way to avoid surgery?
Thank you very much for your help!
Yanche, I appreciate your reaching out to me with your concerns. Of course, given the privacy issues that exist in the United States, as well as the fact that I cannot offer actual treatment advice across state lines need to recognize that what I say is not medical advice and that I must state that my disclaimer applies.
That said, it is well known that NOT all meniscal tears require surgery. Do some patients do better following surgery, yes. Can arthritis set in after a meniscus tear? Yes. Do some experience a worsening of their arthritis, yes. Do some experience worsening of their arthritis whether or not they’ve had surgery. Yes. The mere fact that you possess a meniscus tear puts you at risk for developing degenerative changes or arthritis. Those changes are not necessarily going to be worsened by your activity level.
I can not tell you if you need surgery or not. We as physicians need to endeavor NOT to treat MRI findings, but to treat patients. That takes into account the pain your meniscus tear is causing, and what the effect on your quality-of-life is. Again, if there was a loose flap, or loose piece, and your symptoms were deteriorating and your pain was increasing, we would be looking at a different scenario. That does not appear to be the case right now.
The activities which typically worsen symptoms because of a meniscus tear are turning, pivoting, and twisting. Straight ahead activities such as cycling or walking, and even jogging are generally very well tolerated.
Is surgery necessary? I cannot answer that. There are too many variables involved and each case needs to be approached individually. Are you causing more damage by waiting? It is very unlikely. It is entirely possible that the changes you are seeing on your MRI are purely related to the fact that our bodies change with age and degenerative or torn menisci, are simply a consequence of that. Should you alter, change your activities? Do so, based on your pain. Right now it is too son to tell if your pain will resolve spontaneously…. many people with meniscus tears have no or little pain and live very active lifestyles.
The next step, if you still have a number of questions — it would be nice to have a good long sit down and talk with an orthopedist who is willing to engage you, look at you, and the effect your tear is having on your quality-of-life – – – and not simply look at your MRI and tell you that surgery is necessary. Those surgeons do exist… You simply need to find them. I would also consider waiting a few weeks to see if your symptoms and pain improve on their own.
Good Luck
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
Slawomir Siemaszko
Hello Dr. Luks
Let me just say thank you very much for your sincere video , answers and all the posts from others.
I hit my knee 3 years ago it did not hurt very much so I left it alone. I work physically so I am constantly bruised up, cut ,bang up etc so any problems are usually fixed with couple of Advil pills .
However since I hit my knee I have a small inconvenience and I am worrying that it might get worse
I am able to walk, run without a pain the only pain I am getting is when I cross my legs. Also when I ride my bike the knee clicks but no pain
So it took me a year after the incident to get my first MRI (no insurance paid cash) stating:
1st Findings: the osseous structures of the left knee demonstrate normal morphology and alignment. there are no focal areas of abnormal bone marrow signal to suggest fracture, contusion infiltrative or destructive process. The patella is well seated in the trochlear groove. No Joint space abnormality. Femoral, tibial and patellar articular cartilage demonstrates no significant abnormality. The extensor mechanism medial and lateral collateral ligaments as well as anterior and posterior cruciate ligaments are intact. The lateral meniscus is normal in size shape and signal. the posterior horn of the medial meniscus demonstrates globular areas of increased T2 signal that extends into inferior articular surface suggestive of tear. The anterior horn of the medial meniscus demonstrates no abnormality.
impression:
Globular areas if increased abnormal T2 signal extending into the inferior articular surface of the posterior horn of the medial meniscus suggestive of meniscal tear. Mild subchondral sclerosis of the medial tibial plateau , probably on a degenerative basis.
After 1st MRI I did nothing for another 2 years then I got my medical coverage so i did second mri that is stating:
2nd Findings: mri of the left knee demonstrated normal joint alignment. There are no fractures or dislocations. bone marrow signal appeared unremarkable. There is a medial meniscal tear involving the midbody and posterior horn, involving the articulating undersurfaces in these areas
Laternal meniscus appeared intact.
The acl,pcl,mcl and lcl appeared unremarkable there is a small joint effusion. Extensor mechanism appeared unremarkable. Retinaculum appeared normal. Surrounding soft tissues appeared unremarkable
Impression:
Medial meniscal tear involving the midbody and posterior horn into the inferior articulating surfaces. Lateral meniscus as well as collateral and cruciate ligaments appeared unremarkable. A small joint effusion
So as u see there the mri’s were done 2 years apart and the finding seem the same to me but the join effusion
My concern is the damage in your opinion is getting worse ? i know that I want to avoid any surgery at all cost .I made it without fine for 3 years. The pain in the first year of the incident with the knee went away but then at work I twisted my leg and it started to hurt again a little from 1-10worst the pain is 2 If i cross my legs or twist my body with feet standing firm to the ground. It started hurting very little when I became active in January
, I walk 10k a day and if not walking I bike for 20 miles.
I just worry that by doing so much activity it will get worse
Is there any pointers u could give me ? the pain is still same as before
Does it look like the condition of the damage getting worse by You reading the mri?
Should I do less activity to avoid the surgery or should I just do all as I did and wait and see what would happen?
Thank you for any opinions u could provide me
I really appreciate it.
Slawomir, I appreciate your reaching out to me with your concerns. Of course, given the privacy issues that exist in the United States, as well as the fact that I cannot offer actual treatment advice across state lines need to recognize that what I say is not medical advice and that I must state that my disclaimer applies.
That said, is certainly the case that all meniscal tears do not require surgery. Do some patients do better following surgery, yes. Do some experience a worsening of their arthritis, yes. Do some experience worsening of their arthritis despite whether or not they’ve had surgery. Yes. The mere fact that you possess a meniscus tear put you at risk for developing degenerative changes arthritis. Those changes are not necessarily going to be worsened by your activity level. As someone who walks frequently and bicycles frequently the benefits to your overall self and certainly your overall health are outweighed by any presumed damages you may or may not be inflicting upon you knee. Typically, if there is not a loose flap within the knee, then there is no mechanical wear – – – and thus typically there is not an increase risk of developing arthritis above and beyond what you already possess.
We as physicians need to endeavor not to treat MRI findings, but to treat patients. That takes into account the pain your meniscus tear is causing, and what the effect on your quality-of-life is. Again, if there was a loose flap, or loose piece, and your symptoms were deteriorating and your pain was increasing, we would be looking at a different scenario. That does not appear to be the case right now.
The activities which typically worsen symptoms because of a meniscus tear are turning, pivoting, and twisting. Straightahead activities such as cycling or walking, and even jogging are generally very well tolerated.
Is surgery necessary? I cannot answer that. There are too many variables involved and each case needs to be approached individually. Are you causing more damage by waiting? It is very unlikely. It is entirely possible that the changes you are seeing on your MRI are purely related to the fact that our bodies change with age and degenerative or torn menisci, are simply a consequence of that. Should you alter, change your activities? My personal opinion, and certainly not to be construed as medical advice, would be no.
The next step, if you still have a number of questions, it would be nice to have a good long sit down and talk with an orthopedist who is willing to engage you, look at you, and the effect your tear is having on your quality-of-life – – – and not simply look at your MRI and tell you that surgery is necessary. Those surgeons do exist… You simply need to find them.
I wish you luck.
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
Pol
Hello Dr. Luks,
Before thank you for your great post.
I’m 30 years old, off road bike rider and at August I have got big crash during competition, I was broken clavicle and Knee problem.
After 3 month knee pain decreased but stability feeling not good, can’t run and can’t load.
Yesterday made MRI and result is,
” MM horizontal cleavage tear at post. horn
Otherwise no definite evidence of internal derangement of knee. intact cruciate lig., collat. lig”
And question is
Do I need surgery this type of meniscal tear?
If need is it urgent?
If I wait in second option until next summer, any chance to repair?
I would appreciate you opinion VERU MUCH .
I wrote this before but seems not uploaded”
Best regards,
Pol
Pol… From what you have told me it seems that the tear is the likely source of persistent pain.
The decision to have surgery, unless a loose flap exists, is primarily a quality of life issue. That means if you feel the pain is interfering enough with your quality of life then surgery might help you return to your prior level of function.
Is it emergent… No.
Is it Urgent… No.
Is there a chance that a horizontal cleavage tears “heals” itself… very little chance of that — however, there are plenty of people walking around with tears and do not even know it. Therefore, no all tears cause pain… and you are unlikely to cause any problems waiting to see if your pain improves.
I now have the option to offer people video discussions if you wish to learn more… just go to this address. https://2nd.md/profile/howardluks Then click “Book This Doctor”
Pol
Hello Dr. Luks,
Before thank you for your great post.
I’m 30 years old, off road bike rider and at August I have got big crash during competition, I was broken clavicle and Knee problem.
After 3 month knee pain decreased but stability feeling not good, can’t run and can’t load.
Yesterday made MRI and result is,
” MM horizontal cleavage tear at post. horn
Otherwise no definite evidence of internal derangement of knee. intact cruciate lig., collat. lig”
And question is
Do I need surgery this type of meniscal tear?
If need is it urgent?
If I wait in second option until next summer, any chance to repair?
I would appreciate you opinion VERU MUCH .
Best regards,
Pol
Name Sue Christensen
Hi Dr. Luks,
I have read your article and the responses with great interest and I thank you for taking the time to address these questions so informatively.
I’m a 55 year old female. I don’t lead an active sport-centered lifestyle. Most of my activities come from general work one might do in gardening, farming, walking dogs up and down hills… In May I started to have difficulty going up stairs with any speed . My left leg felt heavier and I had some mild discomfort, I couldn’t keep up any pace if walking. I began to have trouble straightening my left knee knee out and have to tuck a pillow under it for comfort when lying down. There seemed to be swelling around my knee.
I saw an OS who told me he thought it was a torn meniscus but to have an MRI to make sure. The results said I have a horizontal tear involving the posterior hrn of the medial meniscus, small popliteal cyst, mod-lg suprapatellar joint effusion and chondromalacia within the medial femoral condyle and fissuring of the cartilage within the lateral patellae facet. He recommended laproscopic surgery to remove the torn cartilage. I was not in a position to schedule surgery for several months so have been dealing with the situation as it stood.
Recently I read many accounts of people who had the surgery who wish they never had done so. Either the symptoms were not relieved, got worse, they had to go for TKS or experienced unremitting pain that went on for months when they had been almost without pain previously. Many seem to feel that this lap surgery is more effective for the younger, moderately active folk. This has given me pause to reconsider if I have any other options available to me.
My main concern is that osteoarthritis runs in my family, My Dad’s sisters can hardly walk. I really don’t want to encourage an earlier onset of this by having my knee even more weakened. Yet, I would like to straighten my knee more without having it frozen in the current range of motion. I end up limping and over-compensating on my right side. I’m not in pain–just mild aching in one small area that is swollen at times. Is there some way to stop the swelling/supperation? I have heard accounts where some are still plagued by this post surgery–many months later.
Thanks,
Sue
Brian
Dr. Luks,
Hello. I had a patellar tendon tear (right knee) two years ago and was working to reduce weight while officiating high school football this year. This past Monday at work I felt I slight tear or click in the area where they made the incision. It has been stiff for the greater amount of time since. I have officiated football both Friday night and Saturday and ran in it with stiffness. I am concerned based on your comments I may have some concerns. I have done nothing to this point and I do not want to stop working it. The job I do requires standing all the time and I like to ran/walk after work. What sort of advice or ideas might you have? Thank you for your information and passion.
Brian, because of your previous surgery, it is unlikely this is a meniscus tear… it may relate to scar tissue irritation, etc…. In cases where there has been prior surgery, it is best to check with your surgeon.
Howard J Luks MD
@hjluks on twitter
https://www.facebook.com/Howard.Luks.MD
[email protected]
Orthopedic Surgery -Westchester County, Dutchess County NY
914-789-2735
Online Registration or Appointment Scheduling: http://goo.gl/qFEoP
For more information on meniscus tears please visit http://goo.gl/JRCtA and for those who also have ACL ligament injuries or tears you may find this section of interest http://goo.gl/L3N3p
muhammad khalil
hay ! It was great to know that such guideline available from ur kind end. I am 27 and serving in pakistan air force. I have meniscus injuries in my both knees doctors have decided arthoscopy of my right knee.I am doing well in my dialy routine pain is very much in control the only thing i m willing for arthoscopy is that i m afraid that this tear may cause further damage &future problems although i had this injury 4 years ago.MRI findings are stated below.1.ACL is intact;no evidence of any areas of increased intensity in the region of ACL.2.PCL appears normal.3.Loss of bow like appearance of medial meniscus is seen & part of it is seen displaced towards centre of the joint cavity.4.An abnormal signal intensity area is seen in the posterior horn of medial meniscus extending to both the articular surfaces.It appears slightly hyperintense on TIWS & hyperintense on STIR sequence( Grade lll-b tear).5.both collateral ligaments are intact.6.patellar tendon shows no tear/swelling.7.No evidence of any excessive free fluid in the joint cavity/supra-patellar bursa.Opinion. Bucket handle tear medial meniscus with grade lllb tear in posterior horn. Kindly guide me in this regard. Thanx
By your description you sound like you have a very large tear. The tear is displaced, such that a piece is becoming stuck between the bones of your knee joint. Those tears are usually repairable… sometimes they aren’t. Many patients with buckle handle tears will not do well until those tears are treated. A “repair” is preferable to removing the torn piece, if a repair is possible.
Good Luck
Steve Jacobson
Hello Dr. Luks,
I wrote you a week ago – but maybe my letter was to rambling and not easy to answer. I’ll try to rephrase it better.
I have a bucket handle tear that is 5 or more years old (at least the initial injury was 5 years ago), that my Doctor wants to do surgery on (based on my MRI ). He says that he will try to repair as much as possible but from the looks of it, he may have to remove up to 50% of my meniscus.
I’ve been doing a lot of research before my surgery and found your website which helped with some of my questions. I was almost going to postpone my surgery when I saw your comment about “bucket handle tears” and how they need to be fixed. Could you please elaborate this a little more. It seems to me that this is one of the types of meniscus tears that you think should be fixed – sutured if possible. When I asked my Doctor what would happen if I did not have the surgery, he said “that my leg might go out on me while I was doing some activity and that I could be causing damage to my knee bones.”
Did I read you correctly. Is that the type of tear that should be operated on? I appreciate any advice you could give me and thank you ahead of time.
Kind regards,
Steve
Steve… Fresh or acute bucket handle tears are easily treated… and usually repaired successfully. The longer the tear has been present — and 5 years is a long time— the lower the likelihood that the tear is repairable. The tissue deforms and degenerates which makes a meaningful repair difficult at best. If a significant portion of the mensicsus is removed, there are options available, but none funciton as well as your origincal mensicus. At this time, your decision to have surgery is based upon your pain and symptoms since the success rate of a true repair is soooo low.
Hope this helps… and please understand that my disclaimer applies and this does not represent treatment advice… just some info to review on your own and with your doc.
HJL
Nicole B.
Dr. Luks,
I have a couple of questions………….
I have a 13 year old daughter. She is very active. She participates in basketball, volleyball, and track. We are in a very small school district and there are not a lot of kids out for the sports and she is very good at each of them; therefore, she plays 99% of the game. Last school year she hurt her knee. We did not have insurance and were not able to do an MRI. (I regret so much). Over the summer and up until now she complained off and on. Some days it didn’t bother her at all, a few days she would need to ice it and slow down. She now has had four weeks of physical therapy and felt no improvement so she had an MRI (we now have insurance) and it shows a posterior medial meniscus tear of the horn. (Not sure I wrote that the correct way?) Anyway, my concern is with her being so young, she has four more years of sports ahead of her I know I need to make the right decision in treating this. Is she able to injure this further? Should she be out of all sports right now? What are the risks of having the surgery? What are the risks of NOT having the surgery? What are your thoughts?
Thanks in advance,
Nicole B
Nicole… the treatment or approach to meniscal tears varies a bit when we’re dealing with tweens and teenagers. Their tissue is capable of healing well and re-establishing a normal meniscal support structure. For that reason, many academic knee surgeons will recommend and arthroscopy and repair (not removal, if possible) of a tear that remains symptomatic after a few weeks to months. There is always a risk of the tear getting larger if left untreated. There is always a risk of developing degenerative or arthritic changes if the tear is not fixed or if a piece has to be removed. The risks of surgery include those of anesthesia, infection, stiffness, and the fact that meniscus might not heal.
Good luck… and as I need to say… my disclaimer has to apply and this is simply information you can use, or ignore, when thinking about your options.
Howard Luks
Dez
Dr Luks,
First I would like to say “Thanks” for creating an informative website regarding Meniscus Tears! I believe I have obtained more information from your website regarding Meniscus tears than from my own Orthopedic Dr!
In regards to my situation, I tore my Meniscus two months ago. I was seen by an Orthopedic Dr and had an MRI done about a month ago. I had my follow up with my Orthopedic Dr a few days ago and I feel like he was pushing me for surgery even though I am not experiencing any pain. I am still limping, but not as bad as when I had my injury. I believe I am limping because I have lost muscle in my right leg due to inactivity for the first few weeks after the injury. Also, my doctor did not go over my mri results with me. Basically he mentioned that if I want to play sports or have any real physical activity that I would have to have surgery. I feel that I am limping not because of the injury but because I need to rehab it. I was able to obtain a copy of the mri findings from the mri office which I have included below. I am hoping that you can explain to me what these findings mean. I believe I might be able to benefit from rehab versus going directly into surgery. When I asked my dr about rehab, he said he does not believe in it and does not think it will do anything for me. I am triyng to make the best decision for me but I need some info in order to do so. I would like to have surgery as a last resort. Any info you could provide regarding my MRI results would be great! Thanks!
(MRI Results)
Findings: The anterior and posterior cruciate ligaments are intact, as are the medial and lateral collateral ligament complexes. The lateral meniscus is intact. There is a non-distracted radial tear reaching the peripheral hoop fibers involving the posterior horn/body junction of the medial meniscus. Cartilage is preserved. Extensor mechanism is intact. There is a small effusion.
Impression: Non-distracted radial tear reaching peripheral hoop fibers involving the posterior horn/body junction of the medial meniscus with small effusion.
Name Marie Danel
Dear Dr Luks
Thank you for having such an informative site and a place where frightened individuals like me can ask questions. And thank you for having the time…
I am 51 and 8 months ago I have experienced quite severe swelling of both knees, initially without any pain, following few days of walking across a hilly terrain . The swelling in right knee subsided after several days, but the left one started aching even during the night and I could not find the right position for my leg when sleeping. A big Baker’s cyst appeared behind, I could not walk up and down the stairs, and it felt like there was a wedge between my femur and tibia when I tried to bend it. I was sent for Xrays and USG, slight osteoarthritis was diagnosed and I was told: “Nothing to worry about” in respect to the Baker’s cyst.
Despite RICE and treatment with NSAIDs my knee remained swollen, painful and hot for more than 4 months.
Tthen MRI was done and detected ” Horizontal oblique tear extending to the inferior articular surface body and posterior horn medial meniscus with small displaced posterior body meniscal fragment within the inferior tibiofemoral recess. 5mm para-meniscal cyst at the posterior junctional zone with further 5mm para-meniscal cyst mid posterior body. Generalised chondral thinning of the weight bearing medial tibiofemoral compartment with a 4mm near full thickness chondral defect mid weight bearing surface at the medial femoral condyle. Possible small in the third radial tear mid body lateral meniscus. Small full thickness chondral defect with subchondral oedema of the lateral tibial plateau. Large 6 cm Baker’s cyst craniocaudal. ”
I waited 10 weeks in a queue for the consultation with the orthopaedic surgeon, who suggested partial meniscectomy and promised that after that the Baker’s cyst will diappear as well because the reason for inflammation woul be gone.
If that was suggested to me 3 months ago I would have jumped into the operating theatre without a second thought. However, since the MRI, most of the swelling and pain are gone, there remain just a bit of discomfort behind the knee, and a feeling of slight obstruction inside when I squatting. I can bend the left knee now nearly as much as the right one and stairs are no problem, but occasionally I still feel a small twinge of pain. So it is much better although still no good after 8 months…
My arthroscopy is scheduled in 10 days, but now I wonder if I declined it, would my knee continue to heal or would I be damaging it unknowingly even more?
Is it possible that the symptoms (and the cause) of mechanical obstruction I felt for nearly 5 months are gone for good? The OS said it would not heal itself, and that the torn part of meniscus needed to be removed. He also said that there was no arthritis even if Xrays suggested there was.
I am so afraid of surgery and do not want to have it if I can avoid it . But I do not want to risk further damage and rist that the swelling and paing comes back when I stat walking more…
I would apprecialt you opinion VERY much.
Thank you !
Marie
Marie… pardon the late response. Did you go ahead with the surgery? In general,. myself, and many other academic knee docs go very slowly with knee that possess both meniscus tear and osteoarthritis (thinning of the cartilage). An arthroscopy can improve your symptoms, but it can also worsen them if the arthritis kicks into high gear and worsens rapidly.
I hope you are doing well.
Howard Luks
Name Marie Danel
Thank You for your comments , Dr Luks!
No, I did not have surgery. I chickened out.
And because, as I mentioned in my original post, while waiting for the surgeon’s appointent I have observed slow improvement in my condition I decided to wait another several weeks. And my knee continued to improve, the pain is now only accasional: it is light and it comes and goes, and I have longer and longer periods without pain and I can now bend my left knee nearly as much as the right one.
I am careful, try not to overuse it, take lifts and not stairs and instead of my previous long walks I do medical Pilates now. And hope it will continue to improve. And perhaps in a few years time, if it gets worse, there will be some super implants availalbe???
Thanks again, and for all who are in similar situation I would like to emphasise that my knee was hot and I had bad pain , swelling and limited movement for nearly 5 months before I started to see it improving, but now it is better, very slightly, but continuously , every day!! Even it I woudl not have 100% recovery, I take it there was no guarantee that I would have 100% recovered after the surgery either…
Thanks again for your comments, especially on the risk of osteoarthritis – they reinforce my decision not to have surgery, at least not yet…
Marie
Thanks for the follow up Marie… good luck to you.
Howard Luks, MD
russell
Dr. Lucks I have a question. I am 22. The only physical activity I have done in the past few months is biking. About 3 months ago, I was simply getting up of the floor and there was a huge crunch and pain in my knee.It got better, and after about 4 weeks, I could walk and go up and down stairs with no pain or instability. However, sometimes I’ll be sitting in a chair, and I uncounsiously twist my knee in a way it doesnt like, even though it wouldnt hurt any normal person, and it spasms out my knee. It hurts so bad it is insane. Since that 1st incident, this “sitting down and having my knee spams” has happend 3 times. The last time it happend it happend in the middle of 6 hour chemisrty test, and I almost failed it because of the pain. I had to have a cop transport me out; I could not walk at all nor bend my knee straight for 2 days. My doctor said it is my meniscus, but an MRI showed no tear. What in the world am I supposed to do? Im afraid out of my mind to do any physical activity, yet my doctor said theres no tear. How am I supposed to fix a problem that is having a severe effect on my quality of life when according to an MRI, no problem exists? Can MRI’s miss tears? What should I do? Thank you so much.
Russell….
Sorry for the delayed reply… I just returned from a week away.
Can MRI’s miss meniscal pathology, yes. Is it common, no. Do your symptoms sound like a meniscus tear — maybe not.
That said, there are ways to determine if the pain is coming from inside a joint. Sometimes we will inject local anesthetic in a joint and see if the pain/spasm resolves — if it does, then you can review options with your surgeon such as therapy, cortisone injections, or perhaps a diagnostic arthroscopy. Most important is a good history and physical exam to determine if the spasm you feel is because of your knee.
Please understand that these are NOT specific treatment recommendations and that my disclaimer needs to apply… this is simply advice to follow to open up a dialogue with your doctor.
Howard Luks
GV
Dear Howard J Luks,
Thanks a lot for your valuable suggestions, only thing I want to know his leaving it as it is will not aggrevate the problem. Further to this i would like to know from you any kind of precaution that I need to take to get cure of this, or any way I get rid of f this without being under going surgery.
Pls suggest the way out.
GV
Hello Dr Lukes, firstly thanks a lot for your valuable help, I had a complex tear involving the posterior horn of medial meniscus extending into the inferior articular surfce and capsular surface with adjacent para meniscal cyst measuring 6X4 MM. and Mild knee join effusion. I need to know what should i do, will the rest for say 10 -15 days will cure it or surgery is the only way to get rid off this.
I am not having too much pain and I feel pais only when I bend or sit and stand.
Your help in this regard will be highly appreciated.
Thanks in Advance
GV
GV… as I mention quite frequently… unless your meniscus tear is causing mechanical symptoms such as locking, giving way or instability then you can most likely wait as long as you want to decide whether surgery is the appropriate option. Many patients with mild symptoms, like you, do very well without surgery.
Good Luck
Howard J Luks
Healthcare – Social Media – Orthopedic Surgery
Voted as one of Top Sports Doctors in United States :-)
Name Lily
Hi.
Well I was reading your article and it definitely got me thinking. I am 17 and about 3 months ago I started having pain in my left knee (about a year ago i had similar pain but the doctor said i was fine). I went to a sports medicine clinic and they did some physical tests and then sent me for an MRI. The MRI came back suggesting that i had a meniscal tear. I am meeting with my orthopedic surgeon to discuss my options and whether I should get a surgery or not. But i would like your opinion! I am a very active person, I practice martial arts, so doing nothing for a month now is not making me happy but the pain has stopped. The problem is that when i try to do something like running or flexing i feel a sharp pain in my knee; also when i put just a little bit of pressure on my knee it starts to hurt and sometimes it locks and i can’t move it for a while. Once i was doing a jumping kick which requires rotation and i couldn’t stretch my leg or walk for about 15 minutes and had to sit out. I really don’t know what I can do, and I’m scared that surgery at such a young age will make everything worse.
I appreciate your help, Lily
Lily…
You sound like a very wise 17 yr old… and kudos for your athletic endeavors!!
You folks with meniscal tears need to be looked at differently than us older folks. Most young kids have tears that are repairable. That means that the surgeon actually sews the tear together to get the meniscus to heal. Most meniscal tears in older people are “fixed” by removing the torn piece. Problems with the knee arise not from the surgery, but what was performed. So if you have a successful repair then you probably are not at increased risk for arthritis like people who have a large tear removed. For that reason many academic sports docs like to operate sooner on these tears to improve the likelihood of obtaining a successful repair. Now… you need to be absolutely sure that when your surgeon says repair — that he/she means that they will be suturing or repairing the torn pieces… not removing them —- unless absolutely necessary (not every tear at your age is repairable).
Hope this helps.
Howard J Luks
Healthcare – Social Media – Orthopedic Surgery
Voted as one of Top Sports Doctors in United States :-)
Lily
Thanks you for all the help!!
Jason
Thanks for your reply.
I am getting an MRI this week to assess the damage. Will the size of tear determine the risk of further injury? Ie. Smaller tear less risk.
I have played football for 13 years and never won grand final and as this is my last season I am very determined to make it back even if just for grand final in 5 weeks.
Are there any exercises I can do to strengthen area?
Jason, Yes, the size of the tear, and the type of tear can determine if surgery is necessary — and it can also tell you if you have a loose flap. If you look at the pictures in this section https://www.howardluksmd.com/education/common-injuries/meniscus-tears/ you will see what a flap looks like and you will understand how a flap tear of a meniscus can become caught, and potentially larger.
I understand your issue, and sadly need to deal with very similar issues on a weekly basis. It’s heart-breaking at times to see people train and try so hard only to be injured the day or week before an event. I can tell you are a determined young man. You need to have a sit down with your orthopedist after you know the type of tear you have. He/She can give you more meaningful advice going forward. Until then , leg extensions and curls as well as cardio (elliptical and jogging) should be fine. Try and avoid turning pivoting and twisting.
Good Luck
HJL
Social Media – Healthcare – Orthopedic Surgery
Jason
Hi.
8 days ago i injured my knee playing Aussie Rules football. I havent had an MRI as yet, but through consultation with physiotherapist’s they believe it is a torn medial meniscus. I have been icing it 4-5 times per day as well as taking anti inflammatories. The swelling is now almost gone, however I am getting a little bit of locking of the knee for 1-2 seconds at a time.
My dilemma is that we are about to enter the finals of our competition. I have a semi final in 3 weeks and if we win a grand final 2 weeks after that. If there is a tear, do you think I will be able to play and then have surgery after the season if need be? And if so, what should I be doing from a rehab perspective to enhance healing? If I do play, is there anything I can do to minimise the chance of reinjuring – ie taping?
I appreciate your assistance.
Jason
Jason … If you are having *mechanical* symptoms because of a presumed meniscus tear (catching, popping, locking, and giving way) then you risk further injury unless those symptoms abate or go away. Mechanical symptoms are usually caused by a loose flap or piece of cartilage. If the piece is large enough to cause mechanical symptoms then the tear theoretically could become larger if you return to competitive sports.
Most patients without arthritis or other issues in the knee recover rapidly from an arthroscopy… but I would find it unlikely that you could return to competitive sports within a week or two…
Good Luck!
HJL
Healthcare, Social Media and Orthopedics ~!
howard luks
Here is the wikipedia page for Ozone Therapy… if anyone is interested. http://en.wikipedia.org/wiki/Ozone_therapy
Anne
Hello Doctor,
I tore my inner right knee meniscus in Feb. this year when I slipped on some laminate flooring pieces and feel to the ground. For a few weeks after it was extremely painful! I never went to see my Dr because I thought it was similar to a sprain, where it just needed time to heal. It did seem to be making progress but the progress would go up and down, but never went completely away. Once summer hit and I was moving around more, outdoors, camping, hiking etc, the pain started getting really bad again. Now it was interrupting my sleep, and was interfering with my usual activity level. My knee doesn’t “give out/way” but if it locks it does hurt. Getting my leg into pants hurts, squatting is painful, and even something simple like getting my leg over a picnic bench seat hurts.
I decided to go to a highly recommended, alternative orthopedic Dr whose original training was orthopedic surgeon (however he doesn’t practice as a surgeon anymore) . He suggested several treatment options one of them being ozone injections. He thought this was the best option and I agreed to give it a try since I know someone else who recovered a knee injury from these. It was almost a miracle at first. For 3 days I had no pain! It did feel a little achy but no sharp pains like I had been having. Gradually the pain did come back, however drastically reduced. Maybe 40-50% of what it was. I called after a week and a half because the pain was still great enough to really bother me, but still nowhere what it was before. I went in for another injection. It did take down the pain again although not as much as the first time. Now 2 weeks after the second injection the pain is inching back up (maybe 30-40% of what it originally was) and at times has very sharp pain. It is still drastically improved compared to when I first went in to see him. But with the pain starting to increase I’m wondering if I go for another injection and stay this course of treatment for awhile more or go to a surgeon? The Dr did say it can still take up to a year to heal. I also know that this Dr is willing to admit when alternative treatment isn’t working and send his patients to a surgeon. I would love to avoid surgery if possible, but I’m afraid of waiting too long before seeing surgeon. This injury is affecting my life. I feel I can’t have my normal activity level, I can’t squat, or kneel comfortably, walking hills and stairs will cause pain. I’m 36 and have 2 kids, I need to be active for. I’d love to know your opinions on ozone injections and my case specifically. I know that surgery can take a while to recover from too, and it still may not ever be the same. I am just frustrated by the pain and the pain affecting my life. Your advice/opinion is greatly appreciated. Thank you!
Anne
Anne… I have heard of ozone therapy for arthritis… but not necessarily for meniscus tears. There are a few studies right now which may lend some scientific proof to many of the claims from the alternative medicine community. If the science proves its usefulness I will begin to investigate using it in my own practice… but let’s get back to you.
You sound like you are having mechanical pain… pain from a loose piece of meniscal or cartilage tissue. Mechanical problems usually require mechanical solutions. I find it very unlikely that more injections will offer long lasting benefit given the mechanical source of your pain (as opposed to arthritis, where the pain is due to loss of cartilage).
The recovery from an arthroscopy for meniscal tears without the presence of arthritis is generally very rapid…. but that’s a discussion you need to have with your surgeon.
If you read your own post… I think the answer is fairly clear. You have a meniscus tear which has bothered you enough to affect your quality of life for a very long time. You have tried many different alternatives to obtain relief. You remain dissatisfied with your quality of life…
Please understand that this is not medical advice… and my disclaimer applies.
Good luck with your decision making.
HJL
Healthcare – Social Media – Orthopedic Surgery
Anne
Thank you for your quick response. It is great to be able to have resources like this available online. With the immediate pain relief I got from the first ozone injection I was very hopeful at first, but since the pain is creeping back, I think you are right and I guess I need to look into surgery as an option.
Thanks again for the info.
Anne
Once again Anne… you are most welcome. Please come back and let us know how you are doing. You can also check out this section which help a little more. https://www.howardluksmd.com/education/common-injuries/meniscus-tears/
HJL
Healthcare- Social Media – Orthopedic Surgery
amber
HI doctor,
I’m a 27 year old female. Two years ago i had a high impact fall in which i broke my patella. I had ORIF the next day. Since the accident i have always had swelling, pain in the medial side of my knee and a sensation of the knee givingway and have never been able to walk up or down stairs since. 4 months ago i underwent hardware removal and chondroplasty for grade 3 chondromalacia of the patella. A few weeks ago I had my first ever MRI done due to continued pain and inability to conquer those stairs which my surgeon said at 6 weeks with good PT i would be able to. The MRI revealed grade 4 cartilage degeneration of the medial femoral condyle and medial tibial plateau with “bone on bone”, bone marrow edema in the medial tibial plateau and the medial femoral condyle anteromedially, the medial meniscus shows alteration of signal intensity at its posterior root suggestive of a degree of maceration. There is no meniscal tear evident. The body of the meniscus is extruded with truncation of the free margin. There is edema within the proximal 2/3 of the infrapatellar tendon. grade 4 retropatellar cartilage degeneration are present involving the medial facet. There is minor edema of the hoffa’s fat pad. And also a small bakers cyst. My question is for a young person who has never had knee problems in the past, is not athletic or overweight could an undiagnosed soft tissue injury to the meniscus or the articular cartilage cause as many issues which are present now?
Thanks for your time
cheers4 amber
Amber… Thanks for reaching out… I love that people are utilizing social media to improve their knowledge and learning about their health.
I’m very sorry to hear of these findings. As you know this represents severe osteoarthritis or post-traumatic arthritis and leaves you with limited options. Is it possible that you suffered an injury to the medial compartment as a result of your trauma, sure. Is it possible that this would have occurred regardless of whether or not the injury was recognized, yes. The problem is simply that once you reach this stage, it is impossible to say for sure what the sequence of events was. The more important question is what do you do about it… Now, very important… this is NOT medical advice and my disclaimer applies… but things to discuss with your surgeon, or another surgeon… unloader braces, visco-supplementation, osteotomies, stem cells (with or without a micro-fracture first)….. it is unlikely that an arthroscopy and micro-fracture alone will help you. Time to do your homework :-)
Good luck.
Derrick
Dr. Luks, thank you so much for being so honest, and generous with your time and energy. God bless you! I have watched your video multiple times, and also read all of the posts.
I am 44-years old, and a lifelong physical fitness enthusiast, particularly strength training. For the past 6-months, I have experienced medial right knee pain during lunges. I attributed this to pes anserine tendonitis, and have plowed on. Of note is the fact that my right VMO is “overdeveloped” both in relation to the VL, as well as the left VMO. Meanwhile, my right glute is slightly smaller than my left glute. Both glutes are disproportionately large and strong in relation to my hamstrings and quads. I can barbell hip thrust 430-lbs for reps, but only squat 270. During lunges and squats, my right leg does seem to slightly cave in, just a bit, as though looking for a better angle to use that dominant VMO.
In the last 6-weeks, I have upped my frequency on squats quite a bit. These are full squats, (hamstrings contact calves) both front and back varieties. This week, after no particular trauma, my medial right knee was very sore. There was a small linear horizontal bruise directly parallel with the bottom of the patella on the medial knee. I began to have pain going up steps, and arising from a seated position, enough that I have stopped squatting, which in itself is causing me great anxiety. (If it sounds like I’m an addict, guilty, your honor :)
When I self administer the McMurray test, I do have pain, no real click but definitely “crunchiness”, although sometimes I do feel a click, or a need to “pop” the knee to align something. I have been icing, and resting, and am feeling a bit better. Walking is fine. Strangely when I go up stairs, if I cue a relaxing of the knee, it doesn’t hurt. I know this is vague, and I really don’t understand the process of what I’m doing either. Also when I arise from a seated position, I have learned to dorsiflex my ankles and push only through the heels, which causes less pain.
My question is if it would be reasonably safe to resume squatting, pain allowing, or am I likely causing further damage to a possibly torn meniscus. Maybe I can tweak my form to a more hamstring dominant squat?
I have no insurance benefits, and am trying to save up money to go to a good sports clinic, but as we have learned in the previous posts, there is a huge profit motive that often trumps sound medical advice in these matters. So I want to gather as much information as possible before I head into the lion’s den. I don’t mind self-paying as long as my care is precise, and results driven. But I digress.
I have been able to self-rehab a torn quad, torn biceps tendon/subscap, tremendous lumbar back spasms, and patellar tendinosis that hurt for almost 2-years. But this one scares me b/c of the non-regenerative possibilities. I don’t want to end up hobbled and in pain. Staying strong and mobile is my goal!
Again, thanks for all that you do. I understand that you can’t provide specific medical advice: any general information or insight would be greatly appreciated. All the best, and keep up the good, necessary work.
Derrick
Derrick… Thanks for the kind words. The magic of social media and healthcare.
If you do in fact have a meniscal tear and you continue with (painful) deep squats it is possible to tear the meniscus more. I would continue your cardio, squats that are not as deep (as long as they don’t hurt) and see how things go over the next 4-6 weeks. If you have any significant residual discomfort at that point then I would see someone. If you develop buckling, instability or giving way I would see someone sooner rather than later.
Good Luck.
Derrick
Thank you, Dr. Luks for your response. I will take your advice. I am a bit confused about pain as it relates to the meniscus, since I was under the impression that there are no nerves in the meniscus. If I don’t experience further pain, is it reasonable to infer that I am not aggravating any possible injury? (Disclaimer, got it, ha ha..)
I re-read my post, and it must sound crazy to a normal person why I would want to keep going. But I do. I am hoping that A.) I don’t have a torn meniscus, and only a nasty case of tendinitis, or B) I have small tear in the red zone that will heal on its own. I have NO buckling, and NO locking.
To further discuss the failings of our health care system, I have a friend who has had a torn meniscus for 8-years; the last 3 have graduated to locking knee, loose, palpable cartilage floating, the absolute worst case scenario, and still, STILL! the doctors are delaying, playing games, giving cortisone shots, etc.
Just by watching your video, and reading your page, I know that he MUST get surgery, and told him so. I just refuse to believe that this is the best we can do. Thanks again, Dr. Luks!
Brad Gilbert
Hello, I have been diagnosed with having both of my meniscus torn in my left knee, plus an ACL tear. I was told to get surgery on both (or, if one at a time, the meniscus before the ACL) , but do not have insurance at this time. Are there any rehab options for me?
Brad… Many patients with ACL tears will do *well* without an ACL reconstruction. The goal is to prevent the knee from buckling or giving way. Each time that happens you risk injuring the other structures within the knee. Exercises and bracing can be effective in some individuals. Other alternatives, depending on your fiscal situation are services like http://www.faircaremd.com where you can negotiate with a provider or institution for a desired service.
Good Luck
Howard Luks
Kate
I forgot to add I have a Baker’s cyst in the R knee. That was the only aberrant finding on the MRI. Thank you!
Kate
Hello! I have a question. I like to walk a lot and 3 months ago I was walking and all of a sudden my R knee had severe pain. I finished the walk and felt like something was really wrong in my knee. It became very obvious that I wasn’t going to be able to walk for quite awhile. So I started biking and doing some swim running and those things were OK. My pain still continued though so I went to the doctor and she said I have all of the symptoms of a medial meniscus tear (joint line tenderness, severe pain in those divets just beneath my kneecap and mild-moderate swelling with activity). So I had an MRI that said my knee is normal other than a Baker’s cyst. This was about a month ago…. Since my knee was “normal” I thought I could start walking again since I had taken 12 weeks completely off walking and had been diligent with exercises from a knee pain book and had a couple appts with my PT…. so I did a few walks and then all of a sudden my pain returned with a vengeance (pain that feels like a nail being driven through my knee with moderate “puffiness” to the knee)…. I’m 29, have been active all of my life. When I was about 22 I was very into rollerblading that involved jumping down flights of stairs (frequently landing on my knees). Other than that there was not an “injury”.
I made an appt with a orthopedic surgeon for in 2 weeks. What do you think I should anticipate? How can I have a normal MRI yet all of the symptoms of a medial meniscus problem. Do you think diagnostic arthroscopy is a good idea? I just can’t believe I’d have a normal MRI because I’ve had injuries before and this is BY FAR the most painful…..
Thank you very much!!
Kate… believe it or not this is not an atypical situation. We see people all the time who present with classic symptoms for this or that only to obtain an MRI and find little if anything. That said, the MRI may have missed something, the radiologist may have missed something, or the pain generator simply is not revealing itself on the MRI. Not all painful problems within a knee will reveal themselves on some MRI scans.
I would be sure that you have copy of the MRI on a disc for your surgeon to review. I would consider a second opinion or second reading on the MRI if you surgeon is unsure of the status of the menisci on the MRI, etc. Diagnostic arthroscopies are occasionally indicated if you have persistent, quality of life limiting discomfort, despite adequate periods of rest, medications, anti-inflammatories, activity modification, etc. Personally, I will usually inject the knee to confirm that the knee joint is the source of the pain. If the injection temporarily alleviates your pain, but the pain returns then it increases the likelihood that your issue is coming from inside the joint (and not the surrounding tendons, etc) .
Good Luck
Kelly
Oh I just realized my phone autocorrected Luks to Luis; sorry about that!
Kelly
Thank you for your time and opinion! I’ll try to schedule an appointment soon, it might be a while though he’s always so booked. Thanks again!
Kelly
Hi Dr. Luis,
I’m sorry to be yet another person bombarding you with their knee problems so I’ll try to make this brief: my main purpose of writing this is to determine if I should talk to my orthopedic surgeon about my knees. I am sixteen and a level 10 competitive gymnast. About eight months ago, I noticed that my knees would accumulate a lot of fluid above the kneecap after any running or jumping activity. Since then, I don’t notice the swelling as much but I have a slight pain and a lot of cracking. Sometimes when I am walking it feels as though I shouldn’t bend my knee; it doesn’t lock but it feels as though it might. My pain level is low yet my tolerance is high; I have an orthopedic surgeon because I sustained damage to my cartilage in my elbows that required surgical removal of loose bodies. Since then, I’ve been very worried about any aches and pains that come with the sport, but I don’t want to waste his/my time at the office if there’s no problem. What is your opinion on this? Sorry, the briefness I was hoping for didn’t really work out… Thank you for your time and for the helpful article!! And I know, your disclaimer applies :)
Kelly … Thanks for stopping by. I’m glad I can act as a resource for people taking an active role in their own health! No apologies necessary.
While I applaud your desire to limit health care costs and your desire not to waste your time or your doctor’s time, when someone has mechanical symptoms — catching, locking, popping, the feeling of giving way or instability — it is time to be seen. As you know all too well. Gymnasts, tri-athletes, etc live a life of significant pain. Most of the aches and pains are simply because you are over-exceeding what your body is capable of handling. That said, most push on- — it is a calling , and most committed athletes, despite knowing what they are doing to their body need to continue.
While many aches and pain can be *ignored* or managed with *benign neglect* when someone (especially at your age) has mechanical complaints it’s time for and exam, X-rays and perhaps an MRI to be sure that you are not suffering from an articular cartilage defect https://www.howardluksmd.com/education/common-injuries/cartilage-defects/ or a meniscus tear https://www.howardluksmd.com/education/common-injuries/meniscus-tears/
Good Luck and let me know what your Orthopod says.
HJL
Gurmeet Singh
Hello I am Gurmeet Singh from India, Somebody twisted my knee 7 months back, didnt take much initiative but after a month got it checkd by doc. He suggested MRI, which showed Partial ACL tEAR, i Took rest, nd advised me to take rest. My knee was gettig weaker, Doctor suggested me to do some exercises, i did. My knee improved, but still when i used to go on heel, nd tried to kick round with other leg, i felt a bit unstability. Now after these months, i can do cartwheel, i can even jump a bit,, but there is a sudden shockto the knee, it give a click sound then i feel a bit pain qhile stretching the leg, after 5 minutes of rest, its fine. Now i again got my MRI done, which states,,”complex tear of posterior hornof lateral mebiscus with meniscal cyst, and partial ACL tear… Suggest me what ia right….
Gurmeet, Thanks for stopping by.
THe ACL, along with the other ligaments in the knee are responsible for maintaining stability. The ACL is the most commonly injured ligament. Many people who injure their ACL (even a complete rupture) do have any any problems with stability. However, the are patients who are very sensitive to even slight tears of the ACL. The ACL has two bundles. If one of the bundles is torn you may experience instability symptoms or giving way. It sounds like you are having instability episodes. One of the reasons we recommend surgery for patients with instability is because every time the knee buckles or gives way you risk injuring the other structures like the menisci. While I can not offer absolute treatment advice from thousands of miles away my suspicion is that you have an unstable knee which has now resulted in a medial meniscus tear. In the US many of us can perform partial reconstructions if only one bundle of the ACL is torn. I’m sure there are Sports Docs in India who can perform the same procedure. I would seek out a well qualified academic orthopedist who can perform ACL augmentations as well as complete reconstructions and allow them to examine you and talk to you and figure out the best way to proceed. Feel free to check out my section on ACL Injuries : http://goo.gl/L3N3p . And here is another blog I wrote about ACL Injuries and the need for ACL reconstructions.
Good Luck
HJL
Healthcare – Social Media – Orthopedic Surgery
Eddie
Hi Doctor,
The reason that I am emailing you is because I have a lateral miniscus tear in my right knee. The doctor said that surgery was definitely a viable option. I have had this problem with my knee for about a year already because I have not made up my mind about the surgery. Based on my MRI my doctor told me that there is a ball of liquid ( he called it a cyst) which is damaging my lateral miniscus. He explained the surgery procedures to me. He told me that they go in my knee and remove the cyst and then remove that damaged miniscus. My fears are that I actually go through with the surgery and come out worse than I was before. I am also afraid that the surgery will bring me more health problems in the future with my knee. Also the part that worries me too is the part where they remove part of the miniscus that is damaged. My doctor said that a damaged miniscus is not doing its function. Before this miniscus tear I had a very active lifestyle. I would like to get back to that lifestyle. I hope that one day I can actually run a marathon. My questions is : 1) Is surgery the only option for me or are there other non-surgical options out there that are effective?; and 2) Have any of your patients had the same experience with thier knee? And if so what was thier experience and how did they treat it? And what was their success? Thank you for your time Doctor.
Eddie
Eddie… If you have tried therapy and other treatment options and you feel that your quality of life is limited to the point where you are unhappy then surgery might be an option. The para-meniscal cysts we see with lateral meniscus tears are not dangerous and do not need to be treated unless they are bothering you.
Good Luck
HJL
Healthcare – Social Media – Orthopedic Surgery
John
Hi there,
I have lost about 70% of my medial meniscus, and I have constant pain and swelling after meniscectomy. Are you familiar with Actifit (http://www.orteq.com) implant? Could Actifit be my treatment?
Thanks in advance.
John,
The current options available to make up for the lost meniscus are meniscal transplantation or the placement of a meniscal scaffold. When they were performing the trials a number of centers placed the scaffolds, but I’m not sure if the FDA has released it for general use as yet.
You need to have a sit down with your orthopedist or someone who has performed many transplant procedures. They will help guide you in determining if you are a candidate, and if so, which option best suits your situation.
Good Luck
Nicola
Thank you to everyone who has contributed to this blog. I have read some of the Q and A
My problem is that I don’t know how I injured my right knee. I do not recall any sudden popping, but in 1 week the pain and swelling just got worse to the point of not being able to stand without feeling my knee would give way on me.
I completed my very 1st 5K run the beginning of June….the pain started about July 19th when I was swimming in my dads pool.
I have had an x-ray and UltraSound which shows a torn LCL and MCL. The Dr was unable to do a full examination due to the pain when he tried to move my knee up/down and left/right. I have to go back next week to see if the swelling has gone down enough for him to try examining the knee again. In the meantime I am taking pain killers&NSAID. Should I ask him about surgery? I am 49 and active. I stand all day at work. Only lasted 4 hours yesterday then came home to R.I.CE.
Nicola… an Ultrasound around the knee is not particularly useful. It doesn’t show the menisci very well in most people.
Unlikely your tore your LCL, or MCL for that matter simply swimming in a pool.
I wouldn’t consider surgery until you have a definitive diagnosis, diagnostic suspicion or plan. Did you have an Ultrasound because you cannot have an MRI??? I would start with pursuing an MRI and a good history and exam… then determine what the next step should be.
Good Luck….
HJL
Healthcare – Social Media – Orthopedic Surgery
Nicola
I will ask for an MRI but suspect it will take a while to get an appointment, they had to squeeze me in for the UltraSound. I live in Canada. When I have a definitive diagnosis I should then ask what my options are. The recovery period for surgery would be too long for me to be off work I assume.
Isn’t it better to just wait it out and see if it gets better on it’s own, using just medication and the
R.I.C.E approach. Would physio or massage be better? We are already short-staffed at work so I really don’t want to spend time off. I have been fitted with a brace for support and am using crutches. I am not able to put any weight on it without it hurting. Going up and down stairs is awful.
Thank you for your speedy reply. I will come back and visit again when I get the final answer from my family Dr. Should I be asking for a referral to an Ortho Specialist??
Lilly
I have just undergone reconstructive ACL surgery (hamstring graft) and was told there was macerated meniscus not able to be repaired. I’m a 17-year old soccer player who wonders now whether I can continue to play following the standard rehab protocol. I would appreciate your opinion and your advice, Doctor. Thank you
Lilly, I’m sorry I can help you out much. Losing a part of your meniscus and sustaining an ACL tear both put you at risk for developing problems later in life. The presence of a tear, which was not able to be repaired should not alter your rehabilitation following your ACL reconstruction. Whether or not sports participation put you at higher risk for developing degenerative changes is being debated. Most sports docs would not hold you back… but that is a discussion for you to have with your Orthopedist.
HJL
Healthcare – Social Media – Orthopedic Surgery
Becky
Thanks Doc,
According to MRI the doc that looked at it said it appears to be a major MCL sprain, they did not see any tears in meniscus, the MCL they said appears intact, the bones and everything else seem good. I have been refferred to physical therapy… I scheduled an appointment at a facility with an orthopedic doc/surgeon(who came highly recommended from numerous co-workers, and they also do on site PT. He is requesting to also have a look at the MRI
I can’t get in to the therapist till August 1st.
Still not sure how long I will be out of work. :(
I am wondering how long in a sprain of the MCL does it usually take to start feeling better?
I have been continuing RICE, along with OTC pain relievers. how ever the range of motion is still not getting any better, ( still cannot bend my knee to go upstairs or pick my foot up to step over my dog) nor is the pain,, and the severe bruising feeling on the inside of my knee.
I am realizing just how impatient I am with this.
Is it possible the MRI may not have picked up on something or is the MCL sprain really this bad.
Being an athlete I have had many sprains, (ankles, wrists, and even my neck) and none have felt like this. The other day i was laying on my stomach, turned over sat up, and my knee popped. Normal for an MCL sprain?
Sorry for so many questions.
Like I said I am impatient with my active lifestyle and job.
Thanks again
Becky
Becky
Doc,
I am a 26y/o female. I am a firefighter/ paramedic (meaning lots of stairs, carrying ppl, pivoting, kneeling etc) I am also a marathon runner and doing kickboxing and jiu jitsu.
On Wednesday I was doing some jiu jitsu when one of the guys tried doing a move on me, i flipped and at some point during that flip that i had this sudden onset of severe (10/10) pain in my left knee. I was unable to move the knee for a good minute, and the pain went down into my shin, and up into my thigh, it was mostly on the inside of my knee. I went home, iced it, took a naproxen, (there was minor swelling and one small bruise on the inside of the left knee) and went back for another hour of kick boxing, I noticed it was extremely tight, painful, unable to bend and would send shooting pain down my shin. the following day I went and saw medical attention. I could not bear weight on it, do stairs, bend or straighten it other than a few minimal degrees. It felt unstable and if the dog would jump up at me it would feel like it was about to give out. It all happened so fast I am not sure if there was a pop or crack or anything at the time of the injury all i know is the pain was extreme and instant and happened pretty fast.
At the appointment it was extremely painful when forced straight it was painful to the touch on the inside of the knee. and all that “fun” bending the doctor does almost got him kicked it hurt so bad. When walking and if i’m trying to step over something i can not pick my foot up (like but kicks) more than a couple inches off the floor,(that seems to be not improving at all) it is extremely painful and shoots down my shin still if i try. it feels more stuck. Picking my foot up the other way(knee highs is still painful I need to lift my leg some to help assist it is a little better, same as if i’m sitting in a chair and am sliding my foot towards the chair, it feels stuck but is able to do if i pick up my knee from under neath the thigh where the thigh and knee meet. and help guide it in. Yesterday my pain started feeling worse again,(more so especially around the knee cap) and it is more painful to touch on the inside of the knee. Lateral movement from the knee down is still very painful, and also shoots down the shin and feels very difficult to force and still feels slightly unstable but not as bad. flexing my foot up and down also produces some pain as well.
I am awaiting the results of the MRI (hopefully will come in tomorrow as I am missing a lot of work this week between my 2 jobs) Doc is sure its a meniscus tear just waiting to see how bad.
In your opinion with my career and extremely active lifestyle, how much rest and rehab do u think i will need. how much pain should be gone before I return to work etc.. how serious does this sound? surgery bad? As far as my running will I always feel pain when running? what about my fighting? I have a marathon in just over 2 months. would it still be wise to run that? Will a meniscus tear affect my career at all? if so how much?
I thank you in advance for your advice and input. take care :)
Becky… please understand that I can not provide specific diagnostic, nor treatment advice via the internet. That said , your injury sounds far more complex than just a meniscus tear. I can count the number of patients on one hand who have described their symptoms a 10/10 and they have *only* had a meniscal tear.
Some meniscus tears will lead to the inability to straighten the knee and cause the knee to feel unstable. That is a unique tear we call a “bucket handle tear'”. In that situation the torn piece flips into the joint and prevents it from fully straightening.
The most common reason people with knee injuries complain of such severe pain on the inner side that radiates down the leg are injuries to the medial collateral ligament or MCL. By far, these are some of the most painful injuries that people can suffer. We do not know why they hurt more than ACL and other injuries, but they do. If you have torn or injured your MCL and the injury is severe enough that would also cause the knee to feel unstable … and it will significantly limit your motion because of pain.
Other possibilities, and certainly not an exhaustive list include injuries to the patella or quadriceps tendon, fractures within the knee and tears or injuries of the Anterior Cruciate Ligament (ACL).
I would be very surprised if you only have a meniscal tear… and if you do, and you do NOT have a bucket handle tear, then it is not the reason why you can’t straighten the knee. IF you DO have a bucket handle tear, they need to be fixed… that is sutured back in place.
Good luck… feel free to stop back after you have had a better exam and you know your MRI findings.
Remember… my disclaimer needs to apply.
Howard Luks
Dee
Hello Doc Luks, I so appreciate what you are doing for all of us. My problem is I have had an MRI after continually complaining of pain behind my left knee and being told that it was caused by arthritis leaking and pressing on a nerve. Finally ordered MRI, but being told I did not have a Bakers Cyst. After MRI was then told, I would need Arthroscopic surgery. Since I will soon be 69 and have osteoarthritis in both knees, my question is, if I don’t get this surgery in August and wait until the beginning of the year or maybe not get the surgery at all, would it cause a severe amount of damage in the mean time? And does this sound like a repair or removal? Also, would he be able to remove the cyst at the same time or would the cyst be left to hopefully go away after the irritating tear has been dealt with? I have to say that most of the pain is from the cyst and so far I have been able to limit the pain with ice. I don’t have any popping noises, no buckling and I am able to walk without pain. Also, I am flying to see grandkids soon and wondered if a compression stocking would help while flying? And I am going for a second Sept 14th, the earliest I could get an appointment.
Thanks so much for your time!!!
MRI report:1)Tear central body and posterior horn medial meniscus. Small horizontal tear extends to the meniscus free edge which is truncated associated with a small, 4-5 mm, centrally displaced meniscal flap fragment. Age of the tear is indeterminate. Meniscus os slightly peripherally displaced related to the central abnormality and mild medial compartment degeneration. Meniscal root attachment of posterior horn and anterior horn medial meniscus are intact.
2)Interstitial signal central fibers ACL consistent with myxoid degeneration. No acute or high grade ACL injury. Mild buckling of PCL is nonspecific. Correlate with clinical ACL stability, PCL is otherwise intact and unremarkable.
3)Intact lateral meniscus and collateral supporting structures including ligaments of posterolateral corner.
4)Fusiform thickening distal quadriceps tendon with magnetic artifact superficial tendon fibers. Changes appear postoperative, but could be post-traumatic. Correlate clinically. No acute or high grad quadriceps tendon tear or retraction. Patellar tendon is intact and unremarkable.
5)*Minimal effusion with 1 x 4 cm Baker’s cyst dissecting about and below the joint line.
6)Mild medial compartment chondrosis. 2mm chondral thinning and fraying opposing articular surfaces over approximately 50% of the articular cartilage. No high grade chondral defect or loose body.
7)The remainder of the marrow, articular cartilage and surrounding musculotendinous soft tissue are with normal limits.
Dee… The decision to have an arthroscopy for a meniscus tear is predominantly a quality of life decision. I can not speak for your surgeon, nor offer medical advice in this venue… HOWEVER… if I hear ” I don’t have any popping noises, no buckling and I am able to walk without pain.” And if I also hear that someone is primarily affected by the swelling in the back of the knee (Bakers Cyst) then I would concentrate on treating the cyst… and perhaps I would not concentrate on the meniscus. Many patients are walking around with meniscal tears and do not even know it. I would discuss alternatives to treat the cyst… injections, medications, aspiration (taking the fluid out), etc prior to considering an arthroscopy. I would also discuss the downsides of an arthroscopy in a mature women with underlying osteoarthritis… rapidly progressive arthritis, post menisectomy osteonecrosis, persistent pain (AND persistent cyst).
Good luck with your second… take your time… there is no rush.
Angela
Dr Luks,
I am glad that I found your page. I had meniscus surgery in 2007, due to exercising. 4 days ago I was running after my Aunts dogs (they got out of the house) later that night my knee started locking up on me and had dull, sharp pains in the back of the knee. Since that night, when I walk up and down the stairs I can not put any weight on that leg, and my knee pops every step I take. I can walk around the house, but eventually I have to stop because my knee starts hurting bad. When I hold my 7 month old son it starts locking up on me and hurting pretty bad. What would you suggest in this type of issue? Would you consider waiting for a certain wait time to see if it heals on its own or would you suggest going to a insta care and getting an xray done on the knee to make sure it has not been re torn?
Thank you!
You need to take locking and giving way symptoms seriously. I would not want to hear that your knee locked and you fell — either alone or while holding your son!! When you have these *mechanical* symptoms or complaints such as locking and popping you should be seen, obtain X-rays, examined, and perhaps referred for an MRI sooner rather than later. Patients without these mechanical symptoms can wait 10-14 days to see if their symptoms subside.
I hope this helps… please remember…. this is not medical advice… just general guidelines and my disclaimer needs to apply.
Howard
Tim
Hello Dr. Howard,
I recently after playing soccer felt this pain toward the medial area of my left knee. For about 2-5 days my left knee was swollen and I applied RICE. The incident occurred on 6/31/2011 and since then my mobility has improved though I do have this pain medially in my knee when I twist my knee in certain angles and plus I get this click sound whenever I get up from the sitting position.
The surgeon looked at the Axial T2 w GRE , coronal 1.5T magnet MRI images.
Findings:
There is a vertical radial tear in the posterior horn of the medical meniscus, with mild central displacement. Small complex tears are also seen in the body of the medial meniscus. The cruciate and collateral ligaments are intact. There is no occult fracture. A tiny bone contusion is present in the medical corner of the medial tibial plateau. Moderate to marked cartilage loss with small focus of exposed bone and underlying bone marrow edema are seen, consistent with Chondromalacia. Similar Chondromalacia is also seen in the medial articular facet and apex of the patella. There is small joint effusion, without loose bodies or baker’s cyst. The quadriceps and patellar tendons are normal.
Impression:
1. MRI of the left knee without contrast showing tears in the posterior horn and body of the medial meniscus.
2. Areas of moderate to marked Chondromalacia in the medial femoral condyle and patella.
As of right now I have full motion in my left leg and can flex and abduct my leg without any resistance. The only pain i feel is when I try to twist the leg medially. My range of motion has improved a lot for the past 2 and half weeks after the incident. I do get sore if I walk more than 3 miles. I also wearing a brace to reduce the stress on my knee.
However my concern is that should I go for arthroscopic knee surgery to shave off the vertical tear and add micro-fracture of the medical femoral condyle? The surgeon has recommended surgery and I feel a bit hesitant to go for immediate surgery and find some alternative instead.
I am trying to find out what is the best course of action.
Thanks
Tim
Tim, Unfortunately you fit into a category of patients that can be difficult to manage… because you have arthritic changes (exposed bone and very thin cartilage) and a meniscus tear. Many orthopedists prefer to be very *conservative with this patient population and only treat the meniscal tear if it remains symptomatic and you clearly understand that your symptoms may persist (because of the arthritis) or they could even worsen (if the arthritis progresses). Without examining you, talking to you and seeing your studies I can not guide your treatment or make specific recommendations — legal issues also prevent this. However, you should clearly understand that these conditions together can be difficult to achieve “success”, if success means returning to the soccer field, basketball court, etc. Plus, with an appropriately performed microfracture you may be off your leg for 6 weeks depending on size, location of the lesion.
Hope this helps… pls understand this is not medical advice… just some thoughts to discuss with your surgeon — and my site disclaimer needs to apply.
Howard
Josh
I hope i’m not too late in responding to this video but i’m 15 and i tore my medial meniscus on my left knee. I’ve been to an orthopedic surgeon who said that based on the time (6-7 weeks) since the injury happened he’s happy with my progress and doesn’t want to operate on my knee, but since then it’s been about 3-4 weeks and I really cant honestly say i’ve improved , if anything my knee feels worse and more painful, but i’ve noticed i have more flexibility when pulling my ankle back as if to stretch my quadriceps? So i guess what i’m asking is do you have any idea how long i’d be looking at for a recovery based on the amount of time since the injury? Or is going in for a scope the option i should consider? i just want to play football again.
I hope you get back to me,
Cheers.
Never too late Josh… I’m so excited to see a 15 year old online and doing their research! Kudos my young man.
Generally speaking, many academic sports docs are more apt to recommend surgery for a bothersome meniscus tear in a 15 year old, because your tears can usually be sewn together as a repair, as opposed to snipping the torn piece out. The longer you run or live with a painful meniscus tear, the lower the likelihood that a successful repair is possible… not impossible, but it does affect the success rate, if the tissue has degenerated.
If your meniscus was going to heal spontaneously, and many do… it usually would have done so by now. I would revisit your surgeon, or consider a second opinion if you still have questions. The typical recovery from a true repair where the meniscus is sewn together is usually 3-4 months before you can return to sports… but every doc has their own criteria for return to sports.
Good Luck… I hope this helped.
Please understand the limitations of my being able to offer medical advice on a website, and across state or international boundaries. This can not be taken as medical advice and my site disclaimer needs to apply.
Sharon
I have an obligque longitudinal tear in the medial mensicus, extending to the femur, involving the posterior horn and the body of the meniscus. Would this require surgery in your opinion? It is a result of a fall 11 months ago, with regular, very painful (swelling also) flare ups every few weeks.
Bob
I recently discovered this site and greatly appreciate your generosity with these resources and with your expertise, Dr. Luks.
On the question of surgery for meniscal tears…. As patients assess their condition’s affect on quality of life and the risks/benefits of surgery, I wonder if there’s a factor they may easily overlook — namely, the affect of the condition on their *future* quality of life and the shifting risk/benefit ratio as they age. For example, let’s say a patient is 50 years old and their meniscal tear “flares up” for a a couple of weeks once or twice a year, enough so that it’s very painful to go down stairs or stand from a seated position, but not enough to warrant surgery. Might that condition have a greater affect on their quality of life when they are 65 (especially if it deteriorates), while the risk of surgery — including prolonged recovery time — would be greater?
The conservative, nonsurgical approach makes the most sense to me, but I wonder about older people regretting *not* having surgery when they could weather it more easily. I do not have clinical expertise, so perhaps I am off track. But it seems to me that sometimes people forget to look forward into what their life and physical condition may *become* as they age. Thoughts?
Bob, thanks for stopping by and thanks for the comments/questions. Once a tear occurs and arthritic process may set in. Many people who surgery to remove the torn portion develop progressive degenerative arthritis. At surgery, if more of the meniscus is removed than is actually torn, there is an increased likelihood of developing osteoarthritis — eventually necessitating a knee replacement. So, the short answer to your question is that symptoms may come and go, or may never come back. In this scenario, I would not consider surgery because of what I may or may not feel in the future. If the surgery offered a clear protective or preserving function then perhaps that concept has some merit. Unfortunately, that is not the reality of meniscus surgery.
Bob
Great info. I’ve learned a lot. Thanks again!
My pleasure.
Cristin
Dear Dr. Luks,
Thank you for putting up this site and being available to answer questions.
I tore my ACL playing soccer in 2007 at age 27. I had it repaired with my hamstring. I then tore my meniscus in 2008 playing soccer. I was told that the tear was more than half way through the actual meniscus. I also had that repaired. I played soccer once or twice since then after I was given the go ahead to do so by my doctor. I haven’t played in over a year and last night I decided to give it a try. Again my Dr. gave me the go ahead. While playing I hear a loud pop and experienced a lot of pain. I am almost certain I tore my meniscus again. Currently I am experiencing pain walking and cannot fully straighten my leg. I have very minimal swelling.
Is it possible the pain will subside and I will be able to straighten my leg with rest and ice?
Should I wait to go to the Dr.? I do not have insurance right now so I really do not want to seek medical attention if I don’t have to.
I am hoping that I can live with this until I get a job and insurance.
Any advice or input you have regarding how to proceed is very much appreciated!
Cristin
Thanks Cristin…. unfortunately, a pop and swelling could mean anything from a strain, to a meniscus tear, to an ACL injury. It is a non-specific event, which normally would require a trip back to your orthopedist. If your lost of extension persists, that can be an issue if it is not due to swelling but due to a locked piece of meniscus etc. If you are not feeling better right now, I would consider calling your orthopedist and informing them of your insurance status. Many of us will work with uninsured patients to be sure they have access to quality care.
Good Luck… and please remember, this is not medical advice and my disclaimer needs to apply
Howard
steven
Thank you for your advice Doctor Howard. I’m so glad I found this website
you are most welcome…
steven
Hello Doctors, I need your opinions on what I should do. I fell on my knee 4 weeks ago and I heard it’s called bending trauma. I had an mri done. Today they told me a have a small lateral tear of the meniscus and a pcl tear as well. The doctor I was speaking too was pushing for arthroscopic surgery to remove the torn area while stating that the pcl will not be a problem once I do rehab. My pain has been subsiding over the past 4 weeks and every week my knee seems to feel better. I can jog but that’s about it. Considering I couldn’t walk the day after it happened that might be good progress. The doctor did say my knee could recover with just rehab but that it could give me problems somewhere down the line and he said with arthroscopic surgery I am almost guaranteed a full recovery. I’m 17 and play soccer and I feel I can go pro no joke. What do you think I should do and what do you think of what the doctor said and how long will the recovery take? Thanks
Steven… Time to strongly consider a second opinion…. Step back and take a look at the what happening… 1- You have a “small tear” … (whatever that means), 2- your symptoms are improving every week… 3- You’ve gone from not walking to running … 4-You are considering a career as a professional athlete 5- THERE ARE NO GUARANTEES with surgery. 6-Many tears in young patients can heal on their own (I have no idea what type of tear you have so I do not know if your type of tear can heal) 7- Once you have a part of your meniscus removed arthritis usually-but not always sets in. 8-Many patients with isolated PCL tears do not need surgery, but some do. Again, no guarantees.
Judging by the facts it seems like you should not be in a rush to have surgery. I would, however, suggest a second opinion.
Good Luck.
Please understand that my site disclaimer applies and this was not meant as treatment advice.
Trisha Torrey
Hi Shawna,
You’ve asked, “are patients allowed to ask doc’s for the types of aids that they think might better help them to deal with the pain they’re feeling-such as meds, or cortisone shots, or support devices, etc…or, is that inappropriate, particularly, as in my case, we don’t have an actual confirmed diagnosis yet? or, perhaps, offensive on some level, b/c it suggests i’m telling them how to do their job? even though that is not at all how i intend it.”
Here’s an idea to keep in the back of your mind: Start shifting the preposition. Medical care should NOT be done TO you or FOR you – it should be done WITH you. That means that yes, you become a partner, and yes, your questions / suggestions / decisions should be addressed and considered.
An effective and fulfilling patient-doctor relationship is 50-50. Your doctor brings 50% in the form of education and experience. YOU bring 50% in the knowledge of your body, what’s working, what isn’t and your very personal knowledge of your beliefs and wishes.
So, knowing that, let’s answer your question:
There are a few things that need to happen here: One, that you need a diagnosis, and two, that you need relief. The questions about suggesting treatments are to provide relief – and yes, that’s important. But sometimes relief can get in the way of the diagnosis, too. If the pain is no longer there, then it’s tough to describe how it affects you, and tougher for the doctor to figure out what is causing it.
And – as you have already identified yourself – you also don’t want to step over that 50-50 line by “telling the doctor what to do.” SO – here’s my suggestion:
Ask questions. “Is there a way to relieve my pain without getting in the way of pursuing the right diagnosis?” “I’ve read about different meds, cortisone shots, and other ways of relieving pain. Would any of them work for my pain?”
By asking questions, you are still acknowledging the doctor’s expertise, but you are learning more yourself about your knee pain, too.
A shameless plug – and the reason Dr. Luks invited my reply to you – you’ll find much much more about these kinds of empowered patient approaches here: http://patients.about.com/
Welcome to the world of empowered patients, Shawna. You’ll find it to be far more satisfying than your experience so far. Please let us know how you do.
Trisha Torrey
Every Patient’s Advocate
http://patients.about.com/
shawna
thk u, ms. torrey, for your answer-going forward, i will apply your suggestions to make a better connection with my provider(s) to see if i can receive what i feel are my needs for relief/care…i also want to thank you for sharing information (links) that lead to more information about your advocacy program/mission.
i never imagined, when i stumbled on dr. luks site (trying in my own way to do research/seek on my knee), that it would lead to such inspiring people as yourself and dave, who are armed with helpful resources & motivating personal stories-not to mention, dr. luks himself, who has spent (it feels) more time, in actual conversation with me, than my own doctor(s).
i have a call into my ins. co. to see if i can make a change to my provider, and will let you all know how i do.
**dr. luks, the other day, dave wondered if you might know of any peer forums for ortho patients-if it happens, that you do, i would welcome checking them out.
also, and this one you may not be able to answer, as you explained certain limitations apply (which i respect), but IF you are, i would like to know what you think-are numbness/tightness (in ft), same side as problem knee, be an issue to visit the er, or just wait it out until an office visit can be made? i ask b/c if i am leaving my current provider, it may take a while b/4 i can get into another, and i don’t know if these new issues are important or normal.
thk u.
-shawna
shawna
dr. luks and dave-i had no idea that there could be such a community of people interested in helping people like me, and others, find the tools necessary to stand up to doctors, who we tend to elevate (or revere), or large ins. co’s, who we know are only (coldly) driven by greed, but who seem unmovable.
so, i appreciate you all so much…and, my son does too i can say, b/c he has seen me smile quite a bit today, in spite of the pain i feel.
i will most definitely be sharing, with all who will listen, my e-patient experience on this site. i’ve heard it said that “pain is a great motivator”, well, it must be true, b/c i had actually never blogged b/4 this, but i’m glad i finally did, b/c i feel very motivated now.
with warm regards.
-shawna
shawna
dr. luks and ms. torrey, i am actually moved beyond words. it is hard for me to express my gratitude.
to actually have my concerns addressed in this forum, and not by my provider(s), is unreal to me. and shows my complete naivete, i honestly assumed doctor’s were in some way, driven by some ethical code to provide the best care available for their patients.
i will work hard on my own behalf to apply what i’ve learned here-trying to stay hopeful that there are, in fact, more doctors out there like you dr. luks.
i have a little one whose life is also being greatly impacted by this (b/c my husband and i are separated), and my son relies completely on me for his care, but of late, i have not been able to provide it the way i am supposed to, which saddens me. so now that i am a little more informed (and encouraged :-D), i will gather my records, as you suggested ms. torrey, and move forward (with my fingers crossed) to a new provider. i will let you know how it goes.
oh, before i close, i would like to ask—just so i’ll know going forward, are patients allowed to ask doc’s for the types of aids that they think might better help them to deal with the pain they’re feeling-such as meds, or cortisone shots, or support devices, etc…or, is that inappropriate, particularly, as in my case, we don’t have an actual confirmed diagnosis yet? or, perhaps, offensive on some level, b/c it suggests i’m telling them how to do their job? even though that is not at all how i intend it.
again, with MUCH appreciation!!
-shawna
And another empowered patient is born :-) People always ask me why I am so active online… and your case illustrates the answer I always fall back to. I want patients everywhere to be provided with useful information without commercial bias. I want patients to feel that they have a say in their own health care! You deserve to be treated like a person and not a disease… you do not deserve to be treated by an orthopedist only looking for MRI findings to justify another surgery. You deserve answers that you are satisfied with … and you will keep looking until you are satisfied. Now friend our FB pages and tell all your friends. Today was the day you became an e-patient (electronic, empowered, engaged) :-) I’m glad we could help!!
Now with regards to your last question… I can’t offer specific medical advice through this forum. Too many laws that forbid this form of interaction. You’re not my patient, and even if you were, we still couldn’t do it without a long consent form filled out in the office :-( HIPAA
Again… I hope you find the physician you are looking for… we are out there. Enjoy your weekend.
e-Patient Dave
Trisha & Howard, thanks for handling this so admirably.
Shawna, everything they said is true, including the economic pressures on the practices where you’re trying to get care. I would only add that many people working in those practices DID go into medicine to do what you and I expect, and it’s no coincidence that health insurance companies have been reporting record profits while many doctors report being squeezed, and many patients experience what you’ve experienced.
The bottom line is indeed that if you KNOW you’re not getting good care, do whatever you can to GET good care – Including having clear words with your insurance company, saying that they did NOT solve your problem. They may come back at you with “But the MRI said no problem found,” and you may need to push back, knowing that you (and your son) are not being served by this malfunction of the system.
Trisha runs a good advocate program at http://www.advoconnection.com, though obviously she wasn’t advertising it here. You might want to see if one of her affiliates is accessible to you. (She’ll correct me if I’m wrong.)
Howard, do you know of any peer forums for orthopedic patients like Shawna?
—
p.s. Shawna, consider this post, by a patient who learned to use what she calls her “mother of a patient” voice.
Similarly, in the book about my cancer, a note about my research nurse is titled, “Would you do it for your child? Then do it for yourself.” And you can apply that when talking to your insurance company, too.
Dave, We all appreciate and respect your presence on my site in this set of threaded comments. Shawna… you may not know it … but you have the most internationally visible e-patient addressing the concerns you raised. You have also been able to share with one the fiercest patient advocates online as well. Patients are becoming far more active members of the health care team. Ultimately the system should be built up around you, the patient. Patient Centric Medicine. Perhaps we’re starting to head that way now… perhaps not. But you have learned a great lesson today…. and hopefully you will share that lesson with others… and that’s how patients will ultimately lead to the change that need to take place to address the issues you raised. You are not alone in this. Plenty of patients on Twitter, Facebook and disease specific sites talking about these very same issues. Sometimes it appears that we’re stuck in an echo chamber … so it is so reinvigorating for us to know that our efforts are paying off.
shawna
again, thk u doctor luks…your responding renews my hope a bit b/c i have not been able to get any of my doc’s to listen to me. they are very dismissive, and the “normal” MRI report finding has not helped.
once i experienced the callousness of the OS, who ordered the MRI, i decided i would not be returning after i’d had my MRI, and instead, opted to return to my GP provider (a physician’s asst.), hoping she would be more concerned than he appeared to be, and willing to send me to another OS, given my symptoms haven’t changed. however, i did not find that to be the case. she explained, considering the “normal” MRI finding, she didn’t feel there was any other cause known to her (that hadn’t already been considered by the MRI) that might be responsible for the pain i’m in. nor, was she willing to take a very pro-active approach of trying find out either, i felt.
the most i got out of her was, she conceded to have my case reviewed by her supervising doctor, but she was very resistant even to helping me, in the meantime, to find ways to deal with pain i’m in, which i found equally frustrating, as not knowing what’s causing the pain. i assumed there could be no harm in providing me, at the least, with the things i know are available to doctor’s to help ease a patient’s discomfort, but i had every one of my requests shot down, as if i had no right to ask. when i asked to have a basic brace to help support me (on a temporary basis) b/c i am not able to walk w/o limping and using a cane, she told me they were only for ligament injuries; when i asked if she could provide medication (not the vicodin i had been given at first), but rather some other pain med that might work in tandem perhaps with the anti-inflammatory meds i already had, she refused-stating those were enough; when i even asked could i receive a cortisone shot(s) in my knee to help numb it (the way I had for my wrist previously), she stated they were only for a situation like my wrist tendonitis; and finally, when i asked if i were a candidate for PT, perhaps they could help relieve the pain, she said, only as a last option-that she needed to be “conservative” in her approach. (unbelievable)
so, saying ALL that to say (my apologies for the length), i appreciate your suggestions that MRI’s are not the only diagnostic tool available, and that another pair of eyes might yield a different result-it gives me something to take to my next appt at the GP’s, with the senior doctor on staff-before i have to completely give up, and just resign myself to live with this pain. i only hope this time, i’m met with more than resistance, b/c you’re right, this definitely does affect the quality of my life.
i just don’t know what rights i have, if any, b/c i’m afraid i don’t belong to the best HMO, and i fear that is what is, in part, behind much of the low quality of care i’ve received so far. :-|
at any rate, i appreciate your taking time out to answer me.
-shawna
Trisha Torrey
Shawna – you are being stonewalled, and you have two choices: you can accept it, or you can do something about it.
Doctors and their associates work for reimbursements by your payer (insurance, Medicare, whoever your payer is). They get paid the same thing whether they spend 5 minutes with you – or 5 hours. Problem is, if they spend extra time with you (10 minutes or more) then they begin to lose money because they can’t fit as many patients in their day.
So your PA has been given these instructions by her bosses: “if a patient will require too much time, then either dismiss her, or frustrate her so much that she’ll choose to leave and find someone else to help. We can’t make money on those patients so we don’t want them around.” And your PA, wanting to keep her job, has done just that with you.
So that’s your choice. You can see yourself as a receiver of whatever care (or lack of care) they are willing to provide – or – you can proactively go find someone who will actually help you. Not all doctors (or PAs or NPs) will simply dismiss you as these folks have.
My advice: get copies of all your records, including those MRI files. Find another primary – one who will take you seriously and will work WITH you instead of AGAINST you. You’ll need to do this on your own, and be sure there is no relationship to the group you’ve just left. you may need to go to the other side of town. Take your records to your new primary. Ask your new primary to refer you to an orthopedist, perhaps a specific one you’ve already researched on your own – once again, someone who won’t be dismissive, but will partner with you.
If your car kept breaking down, you’d either find a new mechanic, or you’d buy a new car. You can’t buy a new body, so you’re left to pursue solutions for the one you’ve got. Don’t let those who aren’t interested in working with you continue to push you around.
Trisha Torrey
Every Patient’s Advocate
http://patients.about.com
Shawna, Trish is a wonderful resource and I hope that you give her advice serious consideration. As both Trish and I have mentioned. You are suffering, you are dissatisfied with the level of care that you received — and worse, you are starting to think that you are going to need to get used to living in a life of pain. You need to feel empowered, you need to understand that there are many more physicians like me out there. Physicians who will work as long as necessary to be sure you are informed and comfortable with the information and plan they have given you.
When enough empowered, engaged or e-patients start to walk out of offices where they feel that their issues were not adequately addressed — the medical community will wake up!
Keep us informed.
HJL
shawna
hi doctor,
i am a 45 yr old woman who fell 3 yrs ago; my rt knee never really felt “right” after that. have had a few incidence since falling of it swelling with lots of pain involved, but they would always subside. that is until recently, approx. 5 wks ago, my knee began swelling and aching so much i had to break down and go to er. i now have problems with it that i did not originally have after the original fall (3 yrs ago), such as popping, clicking and locking with great amounts of pain involved.
i was referred to an OS, who ordered an MRI, but i just found out that the results don’t show any significant problem.
is there any way that i can be in this much pain, but have no reason for it? (btw-no arthritis showed on x-ray taken at doc’s office either).
i am totally baffled.
thk u.
Two choices… at least. I’ve blogged and written about this before. Many outpatient MRIs (especially open 0.3T scans with large “slices”) are difficult to read or are possibly improperly read… so you can always consider obtaining a second opinion on your MRI interpretation. Second thought… I think you may wish to have a second orthopedic opinion too… someone who may not dismiss your issues because an MRI was normal. MRIs do not identify all abnormalities. Many diagnoses can be made be physical examination alone — and the MRI may not show something wrong. Example – snapping tendons. When you’re walking they move and snap, but when you’re lying still on an MRI table they are in their normal position. Find a surgeon willing to engage and work with you to attempt to identify the issue that is clearly affecting your quality of life.
Good Luck
Please understand that my site disclaimer needs to apply.
Amy Henriquez
Hello Doctor,
I have a meniscus tear and a tear in my ACL. this happend about 10 years ago and about every six months I have problems with my knee (pain etc) I can excersice without any problems, except jumping. Should I have a surgery? My doctor says I should by I am leaving a normal life and I am afraid of been worst after than now.
Please help me :) thank you very much for your time.
vince
Hi doc I had atherspoic on my lateral meniscus just had trimming and removing of the torn meniscus 16 days later when I. Squat down I have man just by the outer part of kneecap below were the incicison was made and swelling there is this normal
Barbara
Hello Dr. Luks,
I believe I tore my meniscus while running or playing tennis. I saw an Orthopedic Doctor and he said he is 99% sure that it is a meniscus tear and if so surgery is the way to go. I am having an MRI to confirm in 3 days. My question is, if I walk around on it prior to finding out for sure by the MRI… errands, cooking, etc… can I damage it further? I am a very active person and the thought of being a couch potato until I get this resolved is distressing. I appreciate any insight you can provide.
Thank you.
sabrina
Hello i had a soccer knee injury on december 2010.The doctor said i could have microtears in my knee.i went for physiotherapy for a month.And 3 months later now,i feel pain in my knee.I went to the hospital and the docter said i have meniscus tear.should i have surgery?(i am into competitve sports but im wondering if i could have physiotherapy all the way instead of surgery ?)
Not quite sure what a “micro-tear” is? Not a term we typically use in reference to a meniscus. Either way, if you have a meniscus tear, your decision to have surgery should be based on the effect the tear is having on your quality of life (assuming your physician believes the tear is the source of your pain). If there is little or no arthritis present, and the doctor feels you will do “well” after surgery then you can consider it. This is what I reference when I talk about the personality of an injury ( http://goo.gl/19y6k ). Not all tears behave the same in all patients. Not all patients are active or have discomfort. Therefore some might choose to have surgery and some may not. Time to have a sit down and heart to heart with your physician who can guide you utilizing Shared Decision Making principles.
Good Luck and pls not that my disclaimer needs to apply :-(
Julie
I had my meniscus tear surgically repaired on March 7, 2011. In the the last 3 weeks it feels just like it did before the surgeon fixed it. My question is Could I have tore it again?
Julie… It’s hard for me to comment on that. Too many variables… was there arthritis found, was tear addressed well, etc, etc… This is something to talk to your surgeon about.
Thanks for stopping by.
Gary L.
Dr. Luks,
First off, let me thank you for having this website so that people like me can get an opinion from a doctor who does not have a “direct interest” in my knee.
I am 61, 6 feet tall and 260 lbs. I go up and down a flight of stairs at least 15 times a day. Starting around March 1, 2011, I started to have knee pain for no reason when getting out of chairs. It progressed somewhat over time to where I am now. I had an MRI done and this is the result.
FINDINGS: There is a small to moderate joint effusion. There is marked thinning of the patellar cartilage starting at the patellar region extending to medial facet. mild subchondral edema medial patellar facet associated with area maximum chondral thinning. No acute or unstable osteochondral lesion at the patella. There are subchondral cysts in the posterior tibia at the proximal tibiofibular articulation felt to be degenerative. Small subchondral cystic area – edema seen weight-bearing portion of lateral tibial plateau. Marrow signal otherwise normal. There is moderate medial and lateral join space narrowing with chondral thinning and irregularity both compartments. Irregular tear anterior horn and body of lateral meniscus. medial meniscus appears intact. with only questionable minimal free edge fraying. Cruciate and collateral ligaments appear intact. There is a 6 mm calcific density posterior joint, surrounded by joint fluid either a synovial cyst just posterior to the joint capsule or in the joint space possibly representing a loose body.
IMPRESSION: Triple compartment degenerative changes described. Joint effusoin and synovitis. Tear degeneration ante horn body of lateral meniscus. no definite medial meniscus tear. Calcific density surrounded by joint fluid, posteriorly, possibly loose body or calcific density in posterior synovial cyst.
I don’t like the idea of surgery AT ALL. I will do anything to prevent it. Is stair climbing and decending making my worse? Do I need surgery? Any advice will be greatly appreciated.
Gary
Gary… Thanks for stopping by and thanks for your comments. Please do not take this as personal medical advice… and my disclaimer needs to apply here.
The decision to have surgery for a mensicus tear is generally a “quality of life” decision. Many patients do very well and lead very active lifestyles without having their mensical tears treated surgically.
In addition, there are a number of other things to consider…. such as the realistic chance of obtaining pain relief. The success of an arthroscopy, which can NOT address or alleviate pain from severe degenerative (arthritic) changes, will depend upon whether or not other problems are present. Arthroscopy for just a meniscus tear is, in general, far more effective than arthroscopy for a mensicus tear in the presence of significant degenerative changes.
Do you need surgery? I don’t know? What do you think? What are your non-operative and operative options? What is the realistic chance you will experience relief following an arthroscopy with your MRI findings? Will you require a knee replacement in the future? These are all questions you need to explore with your treating physician.
pooja
my dad left leg right side knee is paining .he is 47 yrs old.acc 2 the MRI report .marked cartilage loss is seen in the medical femorotibial compartment. associated thickening and edema of the mcl is seen,with extrusion of the anterior horn of the medical meniscus and a complex torn of the posterior horn ,with horizontal and vertical components.
effusion is seen ,with mild synovial hypertrophy.possible loose bodies,noncalcified,are seen posterior of the pcl.
ITS PAINING A LOT.IS IT A VERY SERIOUS PRBLM .IS IT NECESSARY TO UNDERGO SURGERY. PLZ SUGGEST ME WHAT SHOULD HE DO.HE DOESNT WANTS TO UNDERGO SURGERY.PLZ RPLY ME AS SOON AS POSSIBLE PLZZZZZZZZZ.THE PAIN IS FROM 3 TO 4 MNTS
From where I sit… the problem sounds more arthritic than anything else… it is very very unlikely that meniscus surgery would be of benefit. If your father is that uncomfortable, have him talk to his doctor about a cortisone injection or injection of Hyaluronic Acid – Synvisc, Supartz, Hyalgan, Orthovisc etc…
Good Luck.
Howard Luks
Ihab
nice article Dr. Howard
i have a question here , If left untreated without surgery for a while let us say two months or like , can a meniscal tear cause further damage to the structure of the knee? .
i am waiting to return back to my country to check some other orthopedics.
regards
Nola B
I fell in the snow over a year ago and immediately felt pain. I had two MRI’s. The second MRI finally showed a complex medial tear of the knee. I have some weeks where my pain is down to zero (out of 10). But the pain seems to always come back twice as bad. It starts out with discomfort at night and then pain all day. I have had therapy and the pain is aggravated if I get on an elliptical machine. My knee pops all the time and does feel like it will give out. The doctor told me that I am a candidate for arthroscopy. I am unsure because since I have last been to the doctor (almost two weeks ago) my pain is back to zero. I am only 33 but overweight. I am worried if I go with the surgery it will make things worse. I would like your opinion.
Nola… I hope that my video helped you answer some of your questions??? It is not always an easy decision… and it is a *quality of life decision* that you should make after having a nice sit down with your surgeon. Many patients who experience pain on a *routine basis* will elect to have surgery… but many will not. That’s why you need to enter into a “shared decision making” (SDM) with your surgeon and go through your issues and come to a *team* decision as to whether or not surgery may or may not be in your best interest.
Judy Douglass
Good afternoon. Could I please ask your opinion. I have a torn meniscus and the MRI findings are as follows: “No evidence of fracture or dislocation. No suspicious focal bony lesion. No obvious soft tissue abnormality. Trace joint effusion. Quadriceps tendon and patellar tendon are intact. Anterior cruciate ligament and posterior cruciate ligament are intact. Medial collateral ligament and lateral collateral ligament are intact. Mild anterior extrusion of the anterior horn of the medial meniscus. Complex tear involving the posterior horn of the medial meniscus which extends into the body of the meniscus and to a lesser extent into the anterior horn. Underlying mucoid degeneration of the medial meniscus. The lateral meniscus is intact. No significant chondromalacia patella. No significant chondromalacia of the articular cartilage of the medial and lateral compartments. Impression: Complex medial meniscal tear.” My knee was hurting terribly and I scheduled surgery.
During the past week, my knee isn’t hurting very much and I am questioning whether I should have the surgery.
I would like your opinion. Thank you very much!!! Judy Douglass
In general, many patients with meniscal tears will experience relief after a period of rest, ice, activity limitation, etc. Degenerative tears tend to be less bothersome and require surgery less frequently than other tears — especially flap tears. Many, many patients with meniscal tears can be managed without surgery. This assumes they do not have instability or that the knee is stable and not giving way… and this assumes that the pain is improving and tolerable. Ultimately this becomes a quality of life decision.
Seems like you may have answered your own question. You can always call your surgeon and have another evaluation or seek a second opinion.
These are general recommendations and my disclaimer needs to apply .
Louis
Great Article Dr. Luks,
I have one additional question. If left untreated without surgery, can a meniscal tear cause further damage to the structure of the knee?
This is assuming that the knee does not lock and pain is minimal. I am a very active 20 something that is involved in contact sports similar to wrestling. I am still training and perform reasonably well. The only time my knee feels uncomfortable is when its in full flexion, heel touching my butt – my knee would pop but without pain. I am able to modify my activities/ movements that do not put me in that position too often…
Thanks,
Louis
Louis… in general, if someone is experiencing mechanical symptoms because of a tear, they could theoretically be injuring the articular cartilage on the ends of the bones. If a patient is not experiencing any mechanical symptoms (popping, catching, locking, giving way) than it is reasonable to assume that you are not causing any significant damage.
Of course my disclaimer needs to apply.
Louis
Thanks for the quick reply,
My knee does pop, but only in full flexion when my heels are touching my butt. (For example, when I sit in a kneeling position in Jiu-jitsu. I stopped sitting like that now.) In this case, do you think surgery is necessary to prevent further damage. I understand these are general recommendations, but I am curious.
It’s strange because I rarely experience any pain. Perhaps once when the actual injury occured, and once a few weeks back when my injury sort of flared up (it went away after a few days).
Alain
Good Afternoon Dr. Luks,
Thanks a lot for all these questions and greats answers.
I am writing from Paris, France.
2 months while playing a soccer game, I broke my knee. And later my MRI says:
– Bucket handle tear around 50% of my meniscus
– and 17 years ago I had an ACL tear while playing soccer too. but I did 6 month kine, and the results was good, I kept playing soccer at good level.
I am now 37 years old, hope to still do sports for long time, maybe not violent sports. The surgeon told me surgery is the only way. And I am really afraid of that and maybe also of the consequence in future for sport. He suggested suturing the meniscus and later construct the ACL.
Are they any others way to heal from that without surgery ?
If not, is ACL construction really necessary to do sport again ?
Thank you for your time and consideration.
Alain… a displaced bucket handle tear is usually repairable (where we stitch it, instead of remove it). These tears are best repaired early versus late to improve chance of healing and minimize trauma to the meniscus.
Good Luck
Howard Luks