
Meniscus tears are very common. Each knee has two menisci which serve as cushions. They can tear due to degeneration, or they can tear due to trauma or a sports injury. The treatment of a meniscus tear will depend on the type of tear you have, whether or not you also have osteoarthritis and the nature of your complaints.
Many people do not understand why many meniscus tears do not require surgery. Having a firm understanding of what the meniscus does and why some tears do not require surgery should go a long way in assisting you in your surgical decision-making.
Meniscus tears are a very common source of pain in the knee. They are also commonly seen on MRIs obtained for other reasons – and are not necessarily the cause of your pain. Many people come in on a daily basis and ask if surgery for their meniscus tear is always necessary. In this post, we will explore
- what a meniscus is,
- what are meniscus tears,
- why meniscus tears are so common
Meniscus Tears
What is a meniscus? It is a cartilage disk that’s found in the knee.

There are actually two of them. We have one on the inner side of the knee which we call the medial meniscus and one on the outer side of the knee which we call the lateral meniscus. These two disks function as shock absorbers or cushions to minimize the stress on another type of cartilage that we have in the knee which we call the articular cartilage. The articular cartilage is the cartilage that actually coats the ends of the bones. If the two menisci are not present or they’re torn, then the articular cartilage sees an increase in stress and can trigger the onset of osteoarthritis. Meniscus tears are by no means the only cause of osteoarthritis. However, they certainly are a significant contributor.
Why do meniscus tears occur?
Now I see many patients every week who present with knee pain and many of them are suffering from meniscus tears. Why/How do we get meniscus tears? Why do these little meniscal disks tear so easily once we reach our fourth, fifth decades and beyond? Our meniscal tissue is non-regenerative. It’s similar to our brain or our heart tissues. If we have a heart attack or a stroke, we do not regenerate those areas of our heart or our brain. It simply scars in. Yet if we cut our skin, our skin heals. Our skin tissue is regenerative, same with some muscle and a lot of other tissues in our body.
The meniscus tissue in our knee has very few mechanisms for repairing itself. Therefore, every step that you’ve taken, every twist that you’ve done, every time you’ve knelt down or squatted down, you’ve put a force across that meniscus and eventually it wears out and the meniscus tears. (This is why most tears are referred to as being “degenerative”. A lot of times people will note that they simply knelt down to pick up something up and when they went to stand up they felt something rip inside their knee and noted the onset of pain.
Why does a meniscus tear hurt?
The typical patient with a meniscus tear doesn’t have much in the way of pain with walking straight ahead. Sometimes they do. It depends on the size of the tear but usually, they’ll tolerate walking in a single direction very well. Patients with meniscus tears will occasionally complain of pain going downstairs. They’ll have pain getting up from a seated position. They’ll have pain with turning, pivoting and twisting and some patients, if the meniscus tear is large will complain that the knee is buckling or giving way or feels unstable. Many of you will also find you need to sleep with a pillow between your legs at night.
A meniscus tear hurts because they sometimes irritate the lining of the knee joint called the synovium. Tears can also hurt if there is a loose piece which is getting caught in the joint.
Types of meniscus tears?
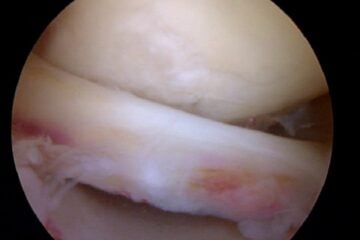
What are the different types of meniscal tears? The majority of tears are degenerative meniscal tears. When you look at the cartilage disc, the edges are simply frayed. The tissue has been destroyed from years and years of use. Nothing you did wrong. The tissue simply wore out. It’s like the front of a pair of blue jeans that you’ve worn for decades and the material just simply wore out.

Then there are those who have suffered more acute meniscus tears and these tears can have different shapes and different patterns. The shape and pattern will determine how symptomatic or how bothersome the meniscus tear will be. If a loose flap of tissue is created and that flap is moving around within the knee – that’s when you’re going to have given way and you’re going to have pain with many activities. You’re not going to tolerate flap tears well and those patients with flap tears (or unstable tears) will usually (not always) go on to require an arthroscopy or a scope to try to either repair or remove that torn piece.
We Treat Patients, NOT MRI findings…
Many patients with meniscus tear pain will improve within a few weeks of onset… in many cases, there is no need to rush into surgery.
- If your pain is starting to improve and
- if the pain does not interfere with your quality of life
- If compression sleeves work to control the pain
- If your range of motion is well maintained and
- You can participate in your normal daily activities —
Then why would one consider meniscus surgery a necessity? Not all “tears” require surgery. Again, we as physicians need to treat the patient, and not the disease.
Consider this article which demonstrated that a sham surgery (incisions made, but nothing done) was no better than treating a meniscus tear when the patient had a degenerative meniscus tear. There are also plenty of studies which show that a degenerative tear can be treated with physical therapy.
How are meniscus tears treated?
If you have knee pain, and you’re found to have a degenerative meniscus tear — I typically advise patients to simply just wait. A lot of times your symptoms will go away. If you sustain an injury and you have an unstable tear, a tear we call a horizontal cleavage tear, a radial tear or a flap tear — those are the tears tend to remain bothersome. If after four, five, six weeks, you still have the same degree of discomfort and quality of life issues, then you might be a good candidate for surgery, which we call an arthroscopy.
Physical therapy can help those of you whose knees feel unstable or weak, and it can help those of you with significant swelling to gain back your motion, stability and strength. Therapy can be beneficial before surgery (pre-habilitation), instead of surgery, or after surgery.
Many patients feel that a compression sleeve makes them feel better and improves their sense of stability – see some of our patients’ favorite knee compression sleeves here.
Do all meniscus tears require an arthroscopy?
What exactly is an arthroscopy?
Basically, an arthroscopy involves bringing you into the operating room, inducing a light sleep, injecting local anesthesia and then placing a fiber-optic camera into your knee through a ¼ inch incision. We then inspect the entire joint, find the tear and determine if it will be removed or stitched back into place. Most procedures take 15-45 minutes and you are able to go home the same day. Whether or not you can return to sports soon will depend on which procedure you had — repair versus removal. More on the recovery from meniscus surgery here.
So if you have a meniscus tear, it’s not all doom and gloom. Many tears do not require meniscus surgery. Some of them do. Some meniscus tears are repairable. Sometimes the torn portion of the meniscus is simply removed.

We try to repair – or suture- meniscus tears whenever possible — but only certain tears are in fact repairable. One caveat: If you have a meniscal tear and you’re experiencing instability or giving way, be very careful with your activities. You don’t want to find yourself on the stairway carrying a load of objects and your knee gives way. If you have instability symptoms, make sure that you have a hand available to hold onto something at all times while you are in your recuperative phase or awaiting surgery or simply waiting to see if the symptoms are going to recover on their own.
Hope you enjoyed this post. For more information there is a more in depth section on meniscus tears here.
And by no means is meniscus surgery or emergency surgery. Take your time, rest and consider a second opinion.
After your meniscus surgery, what should you expect as your recovery from an arthroscopy for a meniscus tear?
Due to the overwhelming popularity of this post, I want to make sure that the many and varied needs that each of you have is met during your visit here. With that in mind, you may benefit in reviewing these related posts on this site:










Dear dr,
MRI report of one if my relative is suggesting below findings, Pls suggest the treatment option available for same and is it necessary to go for surgeries:
Finding:
Findings are suggestive of anterior cruciate
ligament tear with mild joint effusion and complex tear of lateral meniscus
Depends on what your relative is feeling, experiencing and what their exam is like… I do not treat isolated MRI findings… I treat patients :-) And each patient will respond differently.
Hello Doctor,
I had ACL tear surgery in April,2012 . Now again last month I got knee twisted and doctor advised me to go for MRI.
MRI report shows
1.Meniscal tissue in the region of the intercondylar eminence- possible bucket handle tear with significantly attenuated meniscal tissue in the body of the medial meniscus. Mildly attenuated anterior horn of the medial meniscus.
The Surgeon who operated me earlier advised me to undergo arthroscopic for cleaning of the damaged portion, I have consulted another orthopedic, he suggested to try physiotherapy then come to a decision.
What should I do ?
Surgery or it can be cured by Physio and exercises?
Check with your initial surgeon … he may removed a portion of your meniscus during your ACL surgery. If he did… then your second opinion sounds like a good option. If your first surgery did not involve the meniscus — you will likely find that bucket handle tears tend to remain bothersome and can damage the inside of your joint. Therefore many of us prefer to operate on bucket handle tears sooner rather than later.
Thanks Dr. for your reply. I will concern him but isn’t it risky to for surgery a second time ? Will this surgery be as big as ACL Repair one which I had earlier? Surgeon told me like this will be a minor one and I can walk from next day?
Hello Doctor,
Yes he did removed a portion of damaged meniscus at that time when I undergone ACL reconstruction surgery, but he is saying still it need to be operated as that damaged portion can hurt joints in future resulting in arthritis problems. So kindly suggest on this, he will be removing damaged portion of meniscus. Should I go ahead on this?
Good Day Doctor Luks
I am Aloke from Malaysia. I was doing some study about lateral meniscus tear and stemcell therapy, and thus found you on the web.
I had a football injury and was found to have lateral meniscus tear in MRI. Then I had gone through arthroscopy surgery in January 2010.
But now for last 1 year I have got a pain full knee specially while climbing stairs and running. In the recent MRI it was found that there is “Horizontal tear of body of lateral meniscus with adjacent parameniscal cyst”.
I have been consulting a Dr Saw Khay Yong in Kuala Lumpur and he advised me to go through another arthroscopy and stem cell therapy (culturing from Bone marrow).
The surgery is due next month.
I am bit afraid to go through another surgery, because i come to know from some study on internet that this will create some more hole/void in my knee with a possibility of arthritis in future.
Can stem cell therapy resolve my issue? any other alternative we can adopt?
I Request your kind advise on this issue.
** I have sent you a request in Twistle. I can send you my MRI images if you advise.
Best Regards
Aloke Kumar Saha
Locked Bag No. 1, 98009, Lutong, Miri, Sarawak, Malaysia
HP: +60 11 158 63 081
Softphone: +60 85 45 4568
Email: [email protected]
Good Morning Aloke…
Sorry.. I use Twistle for patient communication only.
You should talk to your surgeon about the possibility of trying the stem cells before considering surgery. You could also ask if he would consider a repair (many of us will try to repair certain horizontal cleavage tears), expecially since the stem cells “should” increase the chance of healing. The most recent study on stem cells and mensicus tears shows that the meniscus can partially grow back — that’s a very interesting area of study.
Dear Dr. Luks,
I am a 33 year old male and injured my right knee while salsa dancing on New Year’s. I had no major pain – just felt like I had twisted something. I walked several blocks home from the party I was at and have improved vastly over the last 3 weeks using the RICE method with a reduction in swelling, increased mobility, I can walk slowly but normally and can do stairs. I saw a D.O. who examined me and did not feel it was more than a sprain or at worst a possible meniscal tear. I had left ACL and meniscus surgery 2 years ago this month, and saw my surgeon for my recent knee injury to ensure it was nothing beyond a sprain. He examined me and felt that no ligaments were torn but wanted to rule out a meniscal tear. I just got my MRI results which indicate peripheral vertical tears in the posterior one thing of the posterior horn on both the medial and lateral mesicii, a complete tear of the ACL torn in the mid substance and a grade 2 MCL sprain. This injury has been a completely different experience than when I previously tore my ACL and my surgeon did not detect any possible ligament tears during a physical exam. In your opinion, how should I proceed? Could this be a bad read on the MRI or could it be possible that despite my limited symptoms I have suffered this much damage which would clearly require surgery?
Thank you!!!
It could be an over-read.. or it could also be a poor physical exam. Maybe your knee was swollen and difficult to examine ??? Tearing an ACL graft doesn’t usually produce the same symptoms as tearing your native ACL. There are no nerve fibers, and if an allograft was used, there is very little blood supply. So there tends to be less pain and less bleeding. With new peripheral tears, it is likely that your knee buckled… but I can’t say 100%. Did they mention a bone bruise on the end of the lateral femoral condyle or the posterior lateral tibial plateau? That would confirm that your knee gave way.
Good Luck.. time for another exam.
Howard Luks
Dear Dr. Luks,
A million thanks! Yes, my knee was swollen at the time of exam, but the exams were involved both times (testing range of motion, ability to bend, squat, bear weight, etc.) This injury occurred to my right knee – not the one previously operated upon – so this is my native ACL. The injury experience was entirely different than when I tore my ACL previously – no major pain at all, and I was able to walk home. Last time I could not get up off of the ground. The MRI report does state:
“Complete tear of the ACL. Grade 2 MCL complex sprain. There is edema in the popliteus muscle belly and muscle-tendon junction as well. Bone marrow contusions are seen in the posterior medial and lateral proximal tibia as well as the mid lateral femoral condyle extending anteriorly. Intact extensor mechanism.”
With that said… I don’t feel instability in the knee as I did with my left knee when I tore it – so something isn’t adding up for me.
Thank you!!!
Elliot… those bone bruises unfortunately give it away. They imply that the knee buckled when your ACL tore. The edema in the posterolateral corner goes along with that theory as well. Having seen many many patients with ACL tears, so are more traumatic, thus more painful — some tear with less force, cause less bleeding and inflammation and tend not to bother people as much. Good news on the lack of instability feeling!
Good Luck
Howard Luks