
Why does the outside of my knee hurt ? Lateral knee pain is pain on the outside of your knee. The location of your knee pain can give you a clue about what might be bothering you. Lateral knee pain is a common location for overuse running injuries. Lateral knee pain is also common after an injury in turning or twisting sports. Outer knee pain could also occur without any injury at all. Pain on the outer side of the knee might be accompanied by swelling, clicking or popping. Depending on the location of your pain, the cause of your pain, and the associated symptoms we are usually able to determine what the cause of your pain is and what treatment will be necessary.
Most Common Causes of Lateral Knee Pain:
- lateral meniscus tear
- popliteus tendinitis or instability.
- ITB syndrome
- proximal Tib-fib Joint injuries
- lateral hamstring injury
- lateral collateral ligament injury
Lateral Meniscus Tears:
 The lateral meniscus is one of the two cartilage discs in our knee. The lateral meniscus serves as a cushion or shock absorber. Meniscus tears can occur due to sports injuries or wear and tear. Medial meniscus tears, or tears of the meniscus on the inner side of her knee is more common than lateral tears. Tears of the lateral meniscus can cause pain on the outer side of the knee. Depending on the type of tear you have it could cause snapping, popping, or even locking. On occasion the entire meniscus will flip over into the middle of the knee due to a unique type of tear called a bucket-handle tear. With bucket-handle tears, in addition to having pain on the outer side of the knee, you will likely notice that the knee is difficult to fully straighten. Many tears of the lateral meniscus can be safely observed and do not require surgery. Some of these tears might even heal themselves. On occasion people have unstable “radial tears” of the lateral meniscus which might respond well to a repair where the ends of the tear are sewn back together. Most people with lateral meniscus tears will experience improvement in their pain and function with time and a structured physical therapy program. On occasion surgery will be necessary. But this should be clear, this is a quality of life decision. Surgery on the lateral or outer side of the knee for a meniscus tear is not well tolerated by the knee. Many people are told that lateral meniscus surgery can prevent arthritis from occuring. That’s not true. Perhaps if the torn edges are sewn together we might prevent arthritis from progressing, but if the torn pieces are removed then the lateral compartment often becomes arthritic fairly rapidly. Lateral meniscus surgery, other than a suture repair should be avoided if possible to minimize the risk of developing rapidly progressive arthritis.
The lateral meniscus is one of the two cartilage discs in our knee. The lateral meniscus serves as a cushion or shock absorber. Meniscus tears can occur due to sports injuries or wear and tear. Medial meniscus tears, or tears of the meniscus on the inner side of her knee is more common than lateral tears. Tears of the lateral meniscus can cause pain on the outer side of the knee. Depending on the type of tear you have it could cause snapping, popping, or even locking. On occasion the entire meniscus will flip over into the middle of the knee due to a unique type of tear called a bucket-handle tear. With bucket-handle tears, in addition to having pain on the outer side of the knee, you will likely notice that the knee is difficult to fully straighten. Many tears of the lateral meniscus can be safely observed and do not require surgery. Some of these tears might even heal themselves. On occasion people have unstable “radial tears” of the lateral meniscus which might respond well to a repair where the ends of the tear are sewn back together. Most people with lateral meniscus tears will experience improvement in their pain and function with time and a structured physical therapy program. On occasion surgery will be necessary. But this should be clear, this is a quality of life decision. Surgery on the lateral or outer side of the knee for a meniscus tear is not well tolerated by the knee. Many people are told that lateral meniscus surgery can prevent arthritis from occuring. That’s not true. Perhaps if the torn edges are sewn together we might prevent arthritis from progressing, but if the torn pieces are removed then the lateral compartment often becomes arthritic fairly rapidly. Lateral meniscus surgery, other than a suture repair should be avoided if possible to minimize the risk of developing rapidly progressive arthritis.
Popliteus Tendinitis
Popliteus tendinitis/tendinosis or instability is an under-diagnosed and over-looked diagnosis. Many MRI reports will not focus on the the popliteus, but they should. Many athletes with popliteus issues can be spared unnecessary surgery if the diagnosis is accurately made. The popliteus tendon is located on the outer side of the knee. It is a very small muscle and small tendon however it plays an important role in maintaining stability of the knee. The popliteus can be injured due to trauma or sports injury. More commonly, it will bother you as a result of chronic repetitive stress. Pain due to popliteus tendinitis is on the outer side of the knee and tends to be worse with twisting and turning maneuvers. It does not usually cause snapping or popping, and swelling is not common. Popliteus Tendinitis usually creates a very distinct small area on the outer side of the knee which will be tender to touch. An MRI will often see evidence of inflammation around the popliteus tendon or degeneration of the tendon itself (tendinosis). Often the pain will subside with a change in certain activities and perhaps with anti-inflammatories. Physical therapy can be helpful as well. On occasion we utilize an ultrasound machine to inject the area around the tendon with an anti-inflammatory. Surgery for Popliteus Tendinitis is rarely necessary.
ITB Syndrome Friction Syndrome
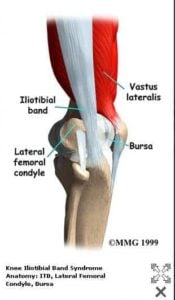
Iliotibial band syndrome or ITB syndrome usually occurs in runners. It is most common in long distance runners. ITB syndrome might also occur anyone who is training vigorously. On occasion we will see cyclists with ITB syndrome however, runners make up the majority of people we see who suffer from this. For the longest time referred to this as ITB friction syndrome. It was felt that the ilotibial band was rubbing against the bottom of the femur which led to a form of tendinitis. It is not actually of the tendon that is the issue in ITB syndrome. The pain in ITB syndrome is usually due to an inflamed bursa, or small fluid-filled sac, which sits just underneath or deep to the iliotibial band. This bursa becomes inflamed with repetitive activities. Many people also wrongly concluded ITB syndrome is common because the ITB is too tight. No research has actually found that the ITB is tight in patients who suffer from iliotibial band syndrome.
We are not quite certain why iliotibial band syndrome occurs. Many causes have been postulated. Some believe it may be due to improper shoe wear. It might be due to curvature of the road of the surface that you run on. One thing for sure, IT syndrome is more common in distance runners.
The bottom line is that ITB syndrome can be a mild annoyance for some, however it might be quite significant pain in others. For most of you it is a self-limiting process which will go away on its own over a few weeks. Unfortunately for some it becomes a long-term issue. Some people report that a roller is useful to help alleviate pain. Others report that shoewear modification and changing the directions of your run can be of benefit. Very little formal research has been focused in this area. If the pain is severe we have found that an ultrasound-guided injection into the bursa which lies just deep to the ITB can be useful. In severe cases which do not respond to treatment surgery might become an option, though this is very rare.
Proximal Tib-Fib Joint Injuries
Injuries to the proximal tib-fib joint are quite rare. When they do occur, they tend to occur in athletes involved in running sports with significant turning, pivoting, or twisting. An injury to the proximal tib-fib joint should be suspected if you heard a loud pop and felt pain on the outer side of your knee when you planted and twisted your leg to turn while running. In general you will find that area to be swollen and quite tender to touch. This is usually because the joint actually dislocated at the time of injury. Most of these proximal tib fib joint dislocations will spontaneously reduce and go back into normal position. On occasion the joint will remain dislocated. If you notice any deformity on the side of the knee then x-rays are indicated sooner rather than later. If the proximal tib-fib joint remains unstable and keeps dislocating then surgery is indicated to stabilize and repair the joint. During that surgery we usually place a screw through the fibula into the tibia. That will hold the joint reduced and allow it to heal. The screw will usually need to be removed prior to return to sports.
Lateral Collateral Ligament Injuries
 Injuries to the lateral collateral ligament not very common. These are typically very high energy injuries. The lateral collateral ligament is very rarely injured in isolation. That means that it is generally injured in combination with the ACL or the PCL. Unless you suffered a very significant injury or trauma it is not likely that she was suffered a lateral collateral ligament injury. If you have pain and instability in the knee feels like it is giving way he should see sports medicine professional sooner rather than later.
Injuries to the lateral collateral ligament not very common. These are typically very high energy injuries. The lateral collateral ligament is very rarely injured in isolation. That means that it is generally injured in combination with the ACL or the PCL. Unless you suffered a very significant injury or trauma it is not likely that she was suffered a lateral collateral ligament injury. If you have pain and instability in the knee feels like it is giving way he should see sports medicine professional sooner rather than later.
Do you have questions regarding an Orthopedic injury or longevity?
Do you want to talk to an expert who can listen to you for 45-60 minutes and explain the options in detail?
Dr. Howard Luks offers remote guidance sessions to review your X-ray or MRI images and explain your options.
Dr. Luks has also received hundreds of requests for educational sessions on the topics discussed in his book, Longevity Simplified.
Pain on the outer or lateral side of the knee joint is fairly common. As you can see from the list of injuries above there are a multitude of causes of pain. Many of these issues respond to nonsurgical management. Return to sports or activities is usually successful after your lateral knee pain has resolved.







Göran
A very impressive site. I’m pleased to find it as it have given me a better idea of what I might have, as well as being warmly human. If I might say so I suspect that you are what most doctors aspire too. It pleases me every time I find a site as yours.
Good on you
Göran
Arthur Nichols
I twisted my knee off of a step. I immediately got up and started walking around. There was some discomfort but not excruciating pain. I didn’t immediately keep off of it or take pain relievers. After a few days it got worse. Icing really helped, I could walk well and do things around the house. I was very careful how I moved and had no problem with bending or straightening out the knee. 2 weeks later it was on and off. I’d feel fine and then for a short time like 10 minutes I had toothache like pain in the knee. on the inside. Since early on the inner right side has been tender sometimes with slight pain radiates to front of knee. the one notable thing is that I have to sleep on my right side. When sleeping on the left the inside surface of the right knee is dully painful and I end up turning back to my right side. even putting a pillow between although this seems to be getting better. I can’t lift my right leg vertically with foot pointing right without pain or sensitivity although that seems to be getting better too! After standing the knee gets stiff and visa versa. I went to Doctor after 2 weeks had an xray everything in line nothing broken she said knee sprain. I would say majority of pain when present right inside of right knee. As we speak I bumped my foot from right to left against a stationary object and it didn’t hurt. Thanks for seeing this and all you do!.Funny pain goes from right side to left side without moving leg or knee?