
Severe pain on the inner or medial side of the knee can be disabling. Many people with terrible pain on the inner or medial side of the knee do not recall any injury. There’s often a similar story or history given by our patients with regard to the onset of severe knee pain.
One day you felt a click or pop in your knee. A few days later you can barely walk. You are usually between 45 and 75 years of age. After kneeling, or squatting to pick something up, you felt a pop inside your knee. You have some pain in the knee, but immediately after the pop, it wasn’t terrible pain. The next day the pain is worse, and the strain on the inner part of your knee continues to worsen to the point that you can not walk. Now your knee starts to swell. Why has the pain on the inside of your knee further exacerbated over the last few days?
Although not described as a terrible triad in the scientific literature, over my 20 years of experience I have heard this story often enough to know what the list of diagnoses will be in this situation. After speaking with you for a few minutes and a brief exam, the diagnosis is often clear. The triad of issues that arise in this situation is a common cause of severe medial knee pain or pain on the inner side of your knee in people between 45-75 years of age.
Your knee MRI will often show a:
- Root tear (Radial tear) of the medial meniscus
- mild or moderate knee arthritis
- bone marrow edema, or an insufficiency fracture in the inner part of the knee.
Those three findings on your MRI are related to one another… in other words, these 3 findings are associated with one another. These three findings are what I refer to as the Terrible Triad of (medial) knee pain. It is an under-recognized set of issues and it is often poorly understood by patients I see for second opinions.
The Terrible Triad: Part I – Meniscus Root Tear
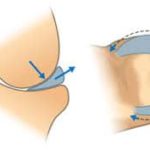 The meniscus plays a crucial role as a cushion inside the knee. It distributes the stresses of walking very efficiently. The root is where the meniscus attaches or is anchored to the bone. The meniscal root attachment degenerates (or wears out) in our knee just like many other tissues in our body. That’s why it will pop and tear while only squatting down or twisting while walking. The trauma or energy needed to tear the root of the medial meniscus in an adult is small. That was the straw that broke the camel’s back. This post goes into more detail about root tears of the medial meniscus. These root tears initiate the process that will then cause the other two components of this terrible triad to worsen.
The meniscus plays a crucial role as a cushion inside the knee. It distributes the stresses of walking very efficiently. The root is where the meniscus attaches or is anchored to the bone. The meniscal root attachment degenerates (or wears out) in our knee just like many other tissues in our body. That’s why it will pop and tear while only squatting down or twisting while walking. The trauma or energy needed to tear the root of the medial meniscus in an adult is small. That was the straw that broke the camel’s back. This post goes into more detail about root tears of the medial meniscus. These root tears initiate the process that will then cause the other two components of this terrible triad to worsen.
The Terrible Triad: Part II- Osteoarthritis of the knee
 The degeneration of the meniscus root causes it to “tear.” When the tear occurs, the function of the meniscus is lost. That loss of cushioning function causes an increase in stress on the bone. The meniscus usually distributes the force of weight-bearing evenly across our knee joint surface. If the root tears and the function of the meniscus are lost, then the force of weight-bearing will concentrate is small areas on the joint surface. That will overstress the cartilage and lead to arthritis. In the terrible triad, many of you will also have at least mild osteoarthritis. Osteoarthritis of the knee implies that you have lost some of the articular cartilage which covers the ends of the bones in the knee. That cartilage also cushions the knee.
The degeneration of the meniscus root causes it to “tear.” When the tear occurs, the function of the meniscus is lost. That loss of cushioning function causes an increase in stress on the bone. The meniscus usually distributes the force of weight-bearing evenly across our knee joint surface. If the root tears and the function of the meniscus are lost, then the force of weight-bearing will concentrate is small areas on the joint surface. That will overstress the cartilage and lead to arthritis. In the terrible triad, many of you will also have at least mild osteoarthritis. Osteoarthritis of the knee implies that you have lost some of the articular cartilage which covers the ends of the bones in the knee. That cartilage also cushions the knee.
The Terrible Triad: Part III- Insufficiency fracture
It follows that if you tear the root of the meniscus the stress in the knee increases. You already have arthritis, so the cartilage cushion was thin and less protective. All of this causes an increase in the pressure within the bones in the knee. In many of you that will lead to a stress fracture or an insufficiency fracture. Those insufficiency fractures of the knee cause a ton of inflammation which shows up on an MRI as bone marrow edema. It takes at least 1-3 days or more for the stress fracture to occur following a root tear. That’s why the pain worsens over the next few days after you felt the pop.
The bone marrow edema caused by the insufficiency fracture causes severe pain. The meniscus is not the most likely cause of pain in this situation. Bone is a confined space, and it can not expand. If you have inflammation and swelling in the bone, then the pressure in the bone will increase. That’s why an infected tooth hurts so much, that infection is in a tight space, so the pressure rises, and it is the pressure that hurts so much.
The terrible triad hurts a lot. That usually leads to a visit to your doctor or an Orthopedic Surgeon. An MRI reveals the findings I mentioned earlier.
Treatment of The Terrible Triad of Medial Knee Pain
Most of you who have all three of the findings I mentioned above will usually have very severe pain. For some of you, your Doctor will focus only on the meniscus and recommend surgery to remove the torn meniscus.
That is not recommended as the best way to proceed if you have a degenerative root tear in the presence of osteoarthritis and bone marrow edema. If your doctor recommends surgery to “clean out” the knee, the research shows that the operation often fails to alleviate your pain, and increases your risk of needing a knee replacement.
Why does your knee hurt so much! It is often the bone marrow edema or inflammation in the bone from the stress reaction or insufficiency fracture which is causing your pain. Usually, time and limiting weight-bearing can improve that pain. It may take 1-3 months for the pain to subside. A subchondroplasty for bone marrow edema may help some people feel better. Determining who might benefit is often a challenge. And infections or complications from a subchondroplasty can be hard to manage.
Do you have questions regarding an Orthopedic injury or longevity?
Do you want to talk to an expert who can listen to you for 45-60 minutes and explain the options in detail?
Dr. Howard Luks offers remote guidance sessions to review your X-ray or MRI images and explain your options.
Dr. Luks has also received hundreds of requests for educational sessions on the topics discussed in his book, Longevity Simplified.
Meniscus root repairs for severe medial knee pain
In a knee with mild arthritis and persistent pain due to a root tear of the medial meniscus, a repair of the meniscus root should be considered. Make sure that your Orthopedic Surgeon knows how to perform meniscus root repairs. They are not easy to perform, and some surgeons only remove these torn pieces. During a root repair, the meniscus is sutured back to its attachment in the bone.

Focusing on meniscus preservation and restoration of more normal force distribution will offer you the best chance of long term success. If the arthritis is moderate to severe and your pain persists despite rest and limited weight-bearing, then a knee replacement might prove to be your better option.
The bottom line is that treatment recommendations need to be individualized to improve your chance of success and minimize the risk of worsening arthritis or the risk of having unnecessary surgery.







Jordie
Hi Doc!
I’m early in this with no diagnostic testing yet.
No acute trauma. Severe medial pain when leg is straight , hanging down, in bed, Walking on and off, or turning, a dull very painful ache. Sometimes it is so very very intense and burns. If I bend knee back…very painful or bend down.
When bending down or sitting on floor Indian style, horrible pain getting up because something is subluxating ???? And it’s a very hard LOUD pop As it goes back.
I can make it happen but it’s soooo painful. Medial side of knee throbs.
Would love your thoughts….
I walk daily, active all my life, and have osteoporosis, but I keep moving.
Age 62
Thank you…headed to Doc because ice, heat, wrapped no help.
Would an X-ray be ok first before MRI? $$$$$ money is a factor
Jordie
NORFOLK, Va
Hi Jordy …
At 62 there’s always a chance that this is a combination of a bit of arthritic change and what might turn out to be a medial meniscus tear. The posterior horn (back) of the medial meniscus is often what tears in a knee that’s starting to show some age-related wear and tear. Obviously you will need to see a doctor to find out exactly what’s wrong… but this is not an uncommon story for us to hear.
tracy
Hi Dr. Luks! I have found your information to be very helpful and was hoping to get your opinion on the findings presented to me. So I’m on the younger end of the average age range (43yr old female) for this possible triad of injuries to happen. I used to be very active in different sports, workouts, etc but activity level declined alot over last 6 years after having my twins. I’ve been trying to get back into some of my activities this past year, (lose weight, get more fit, etc), and while playing volleyball 3 1/2 weeks ago, I came down wrong and felt a pop in the back of my knee and was in a lot of pain when I tried to put weight on my leg. Went home and did ice, ibuprofen and elevation. Next morning could barely put any weight on the leg (still shooting pain on back side of knee), so went and got checked out at an ortho walk-in clinic. They did x-ray which came back fine
(X-ray results: 4 views of the right knee show normal alignment. There is no fracture. There is no signficant degenerative arthrities.)
Was told to keep doing ice, ibuprofen and give it a couple weeks. Although pain greatly subsided, I was still getting frequent jolts of pain where knee would “stick”, or just hurt – on stairs, twisting, etc. Pain is either on lower inside of knee, or back of knee (knee pit). Seemed to be getting a bit stiffer/achier feeling so I went in for MRI after couple weeks.
MRI confirmed MMRT with some moderate chrondromalcia in patellofemoral compartment. Since i’m not in my teens or 20’s doctor said the tear probably not repairable, but that we should do menisectomy. He also said he’s not experienced in root tears, and that only 1 of the 16 doctors at this practice actually have done any root tear repairs (a young doctor who’s only been in practice since 2016).
After everything I’ve read, I’m wondering if menisectomy really best option. It may provide short-term relief, but I want to get back to a higher level of activity and don’t want to jeopardize making my knee worse over next 3-5 years. I need to find a surgeon familiar with root tear repair to see if repair even feasible in my situation (I have tentative appt with the young doc next week as I didn’t want to agree to menisectomy yet), and if he doesn’t think he can repair, do I do the menisectomy or just nothing then (conservative treatment)? Since there is some arthritis in one of the knee compartments I wasn’t sure if that was enough of reason for surgery repair to not be a success, as I’m not really sure of the severity level of the arthritis currently present.
–MRI results:——————-
There are findings compatible with a meniscal root tear of the medial meniscus with minimal medial subluxation of the meniscus. There is evidence of moderate chondromalacia at the patellofemoral compartment.
FINDINGS: This examination shows increased signal in the posterior horn of the medial meniscus interrupting the meniscal root on coronal series 5 number 7 compatible with meniscal root tear. The body and anterior horn are intact. There is minimal medial subluxation of the meniscus.
The lateral meniscus images normally. The anterior and posterior cruciate ligaments, and medial and lateral collateral ligaments image normally. The extensor mechanism is intact.
There is a large joint effusion. A small popliteal cyst is seen. There is some focal bursal fluid at the semimembranosus-medial collateral bursa.
There is moderate chondromalacia with near full-thickness cartilage loss seen over the median ridge and medial patellar facet including some underlying bone marrow reaction in the patella.
No other chondromalacia is detected. No loose body is seen.
———————————
thank you very much for your time!
-Tracy
HI Tracy…
If the pain does not improve with time/ PT, etc… and if there is no significant arthritis then the meniscus should be repaired and not removed.
Renee
I had surgery for 2 meniscus tears on August 17th. It was awesome for the first two weeks. I tripped and fell directly on top of the knee that had the surgery. Now I cannot walk without a limp and severe pain. I have had a cortisone shot and 4 weeks of physical therapy. The swelling will not go down and the pain will not ease up. I have a snap on the inside of the knee that is constant and sharp pain. I was given a different antiinflammotory shot today and told to give it 4 weeks. I was told an MRI would be a waste because it is so swollen and so soon after surgery.
Sounds like a new MRI might be a good idea. Swelling in the knee might actually highlight the important structures better.
ya
Dr. Howard J. Luke, can’t thank you enough for sharing such excellent professional information and opinions which one must pay lots of money for in our time. You make me feel there’s still hope in humanity.
Lynne Marks
Sure appreciate your article and your responses to the comments. Also appreciate your philosophy about educating patients so that they can actively participate in decisions about their health care… wish more medical providers felt same way :>) Thank you!
THank you so much Lynne !!
John K.
The pain described in the beginning of this article almost exactly described what I have experienced. The only exception being instead of a initial click or pop in the knee it was more of a feeling of a bad cramp in the back of the knee that would not go away. After this the next day the knee pain was worse, swelling followed and the pain moved to the inside of the knee. I have dealt with it in the hopes that it would eventually heal itself but it has been difficult. Just curious how often you have heard the initial pain described as a cramp like feeling.
Thanks for the information, greatly appreciated.
HI John…
I have heard patients describe the initial event in many different ways. A good exam and perhaps an Xray and MRI will tell you if the root of the meniscus is torn, and if there is bone marrow edema (inflammation) present.
Good luck !
Amruta Mahamuni
Great blog.Thanks for sharing this information with us.
Sue
Aloha Dr. Luks,
I am 67 and have run for over 30 years. Three years ago a surgeon said I needed a knee replacement. I didn’t have it and now have a new problem. I had an X-ray, then an MRI of my left knee. I went back to the surgeon who told me I had a bruised bone? The MRI showed some subchondral degenerative signal in the distal femur. Also small partial-thickness cartilage fissure, Tear of the free margin of the mid body of the medial meniscus. Indistinct tear versus meniscal contusion at the junction of the mid body and posterior horn of the medial meniscus. The surgeon said I didn’t have a tear? Why would the MRI findings say other? Thank you in advance for your very informative website, and all your help!!
Sincerely,
Sue Hahn
HI Sue…
THose degenerative tears are rarely a problem and often do not respond well to surgery. There is also a fairly high risk of becoming worse after meniscus surgery in a degenerative knee. Sometimes if docs use the term bruised bone they mean bone marrow edema. I also elaborate on it further on this post. That may or may NOT be the source of your pain… I can only tell after a good examination.
Ron Beemer
Good Morning Dr. Luks,
Thanks for your excellent articles. Surgeon wants to do surgery to repair/remove partial meniscus. Previous meniscus repair in USMC. Pain has worsened over past 6 months. Biggest complaint is sleeping or lack thereof. From reading your articles my concern is the marrow edema. Any recommendations? Do you recommend a second opinion? X-Ray shows moderate osteoarthritis, MRI comments below. About 25-30 pounds overweight. Thank You.
Findings: Osteophyte formation and cartilage loss are identified in
the medial compartment. There are several large defects in the
articular cartilage of the medial femoral condyle with marrow edema in
the medial tibial plateau. Abnormal signal within the posterior horn
of the medial meniscus extends to the inferior articular surface on
series 3 images 9-10. It also extends into the meniscal body. The
lateral meniscus is unremarkable.
Definitely seek a second opinion… you have a highly degenerative knee. A straightforward arthroscopy is not usually successful in the long term in these instances.
It would depend on your exam … but you might be correct. Bone marrow edema is often the cause of pain, and an arthroscopy will not address that since it is due to the arthritic changes.
Good Luck
Marvin Silverman
How bad are stairs in a home with these knee conditions (age 68)? I am thinking of buying a stair lift, as advertised on tv, to ride up the stairs. I am concerned that the moderate osteoarthritis and meniscus tear will be exacerbated by the stairs. Thanks!!
Without examining someone or assessing their abilities I can not tell you if that purchase is worthwhile or not.
Kyra Ullman
Thanks for your posts, I’m hoping they can shed light on my increasingly hopeless knee and/or hip injury…
Diane Farnkoff
I do not want a knee replacement yet!! I’m too young., I’m 59yrs.
Completely understood !
Diane Farnkoff
This was so helpful, my knee pain is so severe. Your symptom checker convinced me to see my Dr., I have OA. & Had spinal, & cervical fusions. Metal plates & screws.
I’m glad that you found it helpful