
Considering knee replacement surgery is a tough decision to make. Prior to taking the leap, many will try all reasonable alternatives to knee surgery before scheduling. Knee replacement surgery is a very commonly performed procedure that involves the resurfacing of the bones of the knee with metal and plastic pieces or components. While there is a wealth of information and advertisements recommending which knee replacement to have, and where to have it done, there is very little published about knee replacement surgery alternatives.
The most common condition leading to a knee replacement is Osteoarthritis. Osteoarthritis affects nearly everyone over the age of 60, yet it can also affect those of us in our 30’s or 40’s if we have a genetic predisposition or if we had a previous injury.
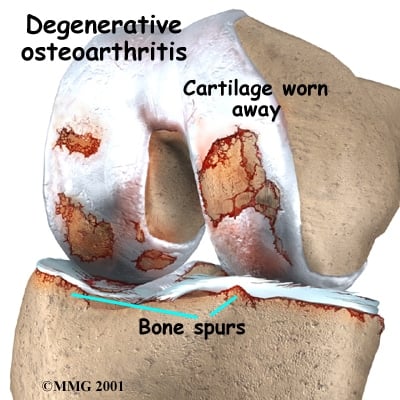
Osteoarthritis, by definition means that the cartilage cushion on the ends of your bones is wearing away. While there is no cure for osteoarthritis, the are many alternatives to surgery available to treat the pain associated with osteoarthritis and thus postpone the need for a knee replacement.
Why postpone a knee replacement? Well, a knee replacement is a big procedure involving numerous risks and a significant recovery period. Some of the risks associated with a knee replacement include:
- Infections
- stiffness
- blood clots, heart attacks and death
- loosening of the pieces or components
- instability of loose feeling in the knee
- injuries to blood vessels or nerves
- risks of anesthesia
Now, if your pain doesn’t improve with physical therapy, a knee compression sleeve, and certain supplements, then, in the right setting and after the failure of non-surgical treatments a knee replacement might prove to be your best option. But you may have a few years left with your knee, and since a knee replacement only lasts so long, the longer you have your own knee, the better the chances are that you will only need one knee replacement in your lifetime.
Related post: Should I have a knee replacement?
Knee replacement surgery alternatives:
There are many well proven alternatives to knee replacement surgery. Some are simple, some are more complex or invasive.
There is a body of literature that supports the use of various supplements and vitamins to potentially slow the progress of arthritis and diminish the inflammation. Some of those which have been studied include
- Chondroitin Sulfate
- Vitamin D : Not useful alone
- Curcumin
- Omega fatty acids
- minimizing sugar intake can decrease total body inflammation
The anti-inflammatories also have a role if you are able to take them.
- Ibuprofen
- Naprosyn
- Celebrex
- Meloxicam and others.
These medications can interfere with other medications like Plavix and Coumadin, and they can cause ulcers and kidney disease so be sure to check with your family doctor first.
Braces or Compression Sleeves: Compression sleeves can be effective in treating the pain associated with arthritis too. Simple neoprene sleeves will significantly improve the pain in many patients. It probably works through a biofeedback neurological mechanism, so if it’s tight enough to stay on, it is the proper size. Do not get a brace that is too tight. In this post I review the compression sleeves I see most often. Other braces that need to be ordered through your doctor can “unload” or take the pressure off side of your knee and transfer the stress to the other side of the knee. Since arthritis tends to begin on one side of the knee these braces can be very effective too.
Physical activity and physical therapy can be effective as an alternative to knee replacement surgery. In general, arthritic joints like to move. Activities such as rowing, walking, swimming or riding a bike are better tolerated. The stronger the leg muscles are, the less discomfort you tend to have. For those who have access to a pool… pool based exercises can be very beneficial for arthritis sufferers. Arthritic knees actually like to move… they become very stiff and painful from inactivity. Do I need to remind of that severe pain and stiffness is in the morning? ;-(
Ice can help alleviate the pain after a day of activity. Compression ice wraps can be used 15 minutes on, 15 minutes off to minimize the risk of frostbite.
Warm compresses to stimulate bloodflow to the knee can help, particularly towards the end of the day, or even early in the morning to help loosen up the joint before the day begins. Warm compresses can be used a few times a day.
Weight loss: For every pound you weigh, you put four to seven times that amount of weight across the knee on each step. So if you weigh 300 pounds, your knee is subject to 1200 lbs of force with each and every step. Therefore, even a small amount of weight loss can lead to significant improvement in pain.
A cane… yes, a cane. Get over it :-) ! They work. Use the cane in the opposite hand. o if your right knee hurts, use the cane in your left hand.
Injections as an alternative to knee replacement surgery.
If you have tried oral medications, braces, and exercise – and yet you are still suffering, there are a number of injections available to significantly ease the pain you are suffering from.
There are many different types of medications or substances available for injection.
The workhorse of the injections is cortisone. This is a steroid and can not be injected too often, but it can make a warm, swollen, painful arthritic joint very comfortable in a very short period of time. There are risks associated with steroids, especially in diabetics where it will cause a rise in your blood sugars. While steroids are useful for acutely painful arthritic knees and people who are truly miserable, there are other injections you should consider either instead of, or after the steroid cools down your knee a bit.
Gel injections… or Viscosupplementaion involves the injection of Hyaluronic Acid (HA) into the knee joint. HA is a substance found in abundance in normal knees, and for some reason arthritic knees stop producing as much. These injections involve putting the Hyaluronic Acid back into your knee over a period of 3-5 weeks. This is generally a very well tolerated injection and can result in relief of your pain for anywhere from 4-12 months. No, it will not work on everyone… but most people respond very well. Many companies manufacture HA and the name brands include Synvisc, Orthovisc, Supartz and Eufflexa.
Platlet rich plasma, or PRP, which involves the injection of a portion of your own blood into your knee has been scientifically proven to reduce the pain from osteoarthritis for up to one year or more. In the end… PRP and stem cell injections may prove to be the best alternative to knee replacement surgery… but the jury is still out. One important caveat… Most insurance plans do not cover PRP injections. It truly is the wild west out there with regards to pricing and preparation. The research about PRP continues to the this day… we are still unsure of the exact reason why it works and the best way to prepare it… but the currently available methods seem to work well. I have called many offices in my area and found that the price for a PRP injection into a knee can vary from $1000-$5000 – so please shop around and do not be afraid to negotiate.
Please note… an arthroscopy, or scope should not be considered a viable alternative to a knee replacement. Having a surgeon go in and “clean things up” is not generally very effective.
Ultimately, you may go on to require a knee replacement. Keep in mind, it should be YOUR decision when that moment should arise. This is a quality of life procedure and only you can determine if you are ready, and if you have suffered enough. Luckily, there are knee replacement surgery alternatives that can work to improve your pain, improve your quality of life and potentially hold off a knee replacement for years.








I’ve had multiple (17) surgeries from a compound fx of tibia/fib years ago. Osteomyelitis as a bonus. I’m 52 active but suffering from knee pain now. MRI shows all kinds of damage. My surgeon said he wants to do arthroscopic procedure to look closer. Said I’d need replacement but no one would want to touch it because of the osteomyelitis. I don’t like pain meds but can’t get relief otherwise. What do I do? .
It’s true that osteo in the past, carries a much higher risk of infection in a future knee replacement. There are ways to minimize the risk of infection, but you need to see a revision joint surgeon who has experience in this area. This is not a knee replacement for your average orthopedist to be doing.
Good Luck
Hi I am 58 yrs old fit lady I have been told by my surgeon that I have no cartlige on the left side of my knee and very little on the left side, she says because of my job and the long hours I am standing on my legs I will now need a replacement knee. I have had three clean out and repairs done the last one I’m still recovering from, as I have to return to work soon as a chef could u please advise me as to which knee brace I should wear as mmy knee feels very unstable.
many of our patients like the Bauerfeind knee braces
Thank you for responding to so many individual requests regarding our diseased knees! Last year, at age 56, after about 10 days of extreme stress, my right knee became incredibly painful – to the point of my not being able to stand. My ortho doctor said the long, banana-shaped swelling on the side of my right knee was a cyst that would return if drained, therefore, surgery was indicated.[Am also knock-kneed, with right leg becoming a “kickstand”] An MRI was done (torn meniscus?); I had knee surgery. After the procedure, the physician said that I didn’t have a cyst after all (it wasn’t there when I woke up and, he “had never been more suprised in the operating room by what he found- compared to what he thought he would find”). When I asked what he DID find, he said, “a synovial response, just like the MRI indicated”). This answer did not satisfy me.I believe the nurse said a meniscus repair was done. After 3 rounds (6 visits each) of PT, I stopped. While my knee pain was practicallly gone, the accompanying arch-of-foot pain, buttocks pain, and calf cramps remained. I went to another Ortho doc when the knee pain returned as well. He eliminated the spine as cause of my other symptoms, and has begun a series of cortisone injections about every 8 weeks. He says I am not bone-on-bone yet, but I am concerned about how much longer cortisone should be continued (the injections work, until they DON’T). He says to expect TKR within 2-3 years – shots for that long? Also, he says, “I did 5 knee replacemnts yesterday, I know what I’m doing”. This concerns me, as this feels like assembly-line surgery to me. DO I NEED TO LOOK FOR A THIRD ORTHO SPECIALIST? Am currently overweight, history of TIAs, seizure disorder under control with minimum meds. Otherwise, only 2 years ago, I was very active, including aerobic- and Zumba-dancing three times weekly. Not anymore.
Arthritic knees typically do not like being operated on. They are very “cranky”. A knee replacement will be necessary when you think it is necessary. Many of our patients have noted significant improvement in their pain with certain knee compression sleeves. In addition, many take Tart Cherry Juice
which is proven to work in many with arthritic knee pain.
Good Luck
I have a question about Knee replacement vs microfracture repair. I injured my knee at age 57 , after physical therapy attempts fail to relieve pain, I was told I was going to have my knee scoped to fix a possible tear. I had this procedure at age 58. I woke up to being told I had a microfracture procedure. I was not even told about this prior to the surgery . I had never heard of it before and it was never discussed. My husband was told I would need a total knee replacement. My question is this what is the success rate of this microfracture procedure for patients in their late 50’s early 60’s . Is it better to do the replacement?
It’s not very effective at our age… especially if the loss of cartilage is extensive. Whether a knee replacement is needed is more of a quality of life decision. It can’t be done for at least 3 months after your surgery or last injection anyway… higher risk of infection.
Hi Dr. Luke
I had a total knee replacement 2 years ago with little improvement. I have a lot of numbness at the lateral side of the knee that radiates down the leg
My surgeon is recommending arthroscopic in that knee replacement. Is this normally done and what risks are involved.
thank you for your I formative column.
Numbness on the outer side of the knee after a knee replacement is normal. Numbness on the outer side of the lower leg could be an issue with the peroneal nerve … or the low back. Unlikely that an arthroscopy will help address numbness. Pain — perhaps, but without examining you I can not comment further on treatments in this forum.