
Complex degenerative meniscus tears are quite common. The majority of us will develop them in our lifetime. The research has been clear over the years. The vast majority of these complex tears do not require surgery. This podcast will explore the function of the meniscus and the consequences of surgery on complex tears of the meniscus.
The meniscus has a very important function in our knee. We have a medial and a lateral meniscus. Both of the menisci play a role in how weight-bearing forces are distributed across the knee. When you step on your knee you put 5-7 times your body weight across your knee as a mechanical load. Any changes to the meniscus will increase the load that the articular cartilage or cushioning in your knee is subject to. That increase in stress will cause the articular cartilage to degenerate and osteoarthritis will occur.
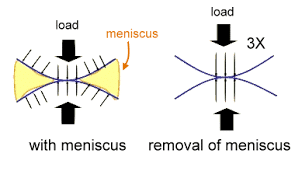 The picture above shows how your weight is distributed across the knee when it is functioning well. If the meniscus has been removed, even if a small piece has been removed, then the stress on the articular cartilage increase 3-fold. That can cause osteoarthritis, which may go on to require a knee replacement.
The picture above shows how your weight is distributed across the knee when it is functioning well. If the meniscus has been removed, even if a small piece has been removed, then the stress on the articular cartilage increase 3-fold. That can cause osteoarthritis, which may go on to require a knee replacement.
Your risk of developing osteoarthritis increases when a meniscus tear occurs. That risk is likely dependent on the type of meniscus tear you have. Degenerative or complex meniscus tears are associated with a lower risk of arthritis development than root or buckets handle tears.
In this podcast, I discuss the what a meniscus is, why it is important, and the result of a study on your risk for requiring a knee replacement if you have a part of your meniscus removed.
Meniscus surgery does not guarantee that you will require a knee replacement. However, as we will discuss it certainly increases the risk of arthritis development significantly. In addition, the discussion in this podcast pertains to a complex or degenerative meniscus tear. Radial or root tears, as well as bucket handle tears are looked at differently. Root and Bucket Handle mensicus tears may benefit from a repair where the meniscus tear is actually sutured back together. In those situations, a meniscus repair may serve you better than a non-surgically managed root or bucket handle tear.
The vast majority of tears in adults are complex degenerative meniscus tears. So this podcast will pertain to most tears that occur after we reach the age of 40.
Click on the orange circle in the picture to listen to the audio.
Do you have questions regarding an Orthopedic injury or longevity?
Do you want to talk to an expert who can listen to you for 45-60 minutes and explain the options in detail?
Dr. Howard Luks offers remote guidance sessions to review your X-ray or MRI images and explain your options.
Dr. Luks has also received hundreds of requests for educational sessions on the topics discussed in his book, Longevity Simplified.








John Czerwinski
Hello, Dr. Luks,
Thank you for the wonderful information you continue to provide.
I am a fit and active 53-year-old with a left knee issue. Nearly six weeks ago, I did back squats for the first time in months with a moderate weight, and then lunges the following day. I did *not* feel any sort of “pop” of a sensation that my knee was giving away. However, that night, my knee swelled up, was red, warm to the touch, and very painful. The pain continued for several weeks, but has now subsided to the point where I only take an anti-inflammatory med at night, since that’s when pain is the worst. I’m still walking with a slight limp, and am using a compression sleeve. Two weeks ago, I visited a PT and then a clinic that specializes in knee injuries for an ultrasound and X-rays. Both the PT and the Dr. at the clinic diagnosed me with a mild MCL strain, and a medial meniscus tear. Per the ultrasound: evidence of horizontal tear in the posterior horn of the medial meniscus; perimeniscal fluid; degenerative changes; mild extrusion. All other findings were normal on the subject (L) knee. Per the X-rays: L knee Kellgren-Lawrence OA Grade of 1; R knee grade of 1+. (I had a prior surgery on my R knee due to a bucket handle medial meniscus tear in 2004.) The clinic suggested PRP injections, and PT, which I begin this week. My goal is to avoid surgery if possible. After reading several of your articles, I believe I still need to give my knee more time, as the pain has significantly reduced, is not popping or locking, etc. My main questions for you are: 1) Whereas I see your point about avoiding surgery for complex degenerative medial meniscus tears vs tears caused by trauma, I can’t say for sure which category I fall into. Is it possible that my tear was caused by a both? 2) Since I’m essentially pain-free, would PRP injections provide any other benefit, such as with healing? 3) How long would you suggest I wait for my knee to improve before getting an MRI and then considering surgery as a last resort? Of course, any other suggestions that would be beneficial are greatly appreciated.
Thank you again for all the helpful content on your site and in your videos,
J
Rob Preston
Thanks for the great information. I’m a 50 year old marathon runner who loves to run. In March I had a MRI and the results were: tear posterior horn medial meniscus, bony edema and tendinosis at semimembranosus attachment and in medial head gastrocnumius tendon. I don’t understand most of that other than the meniscus (The doctor didn’t go over any of it with me). I’ve been doing a lot of bike riding and pool running. About every 2 or 3 days, I try to run and I can usually get 2 miles into it before I feel a dull pain. Then the dull pain comes later in the day. I’ve read your article about running with a meniscus tear and how it’s probably not making it worse. Do you think I’m better off just doing the bike until the pain goes away or should I continue to try the run every few days. It’s getting very frustrating and I just don’t want to make it worse. And I can’t find an orthopedic doctor who is a runner ( I wish I was closer to NY). – Thanks
Well… the risk of developing osteoarthritis (OA) does increase when you tear the meniscus itself. Having surgery to remove the torn piece does not alter that risk. It may in fact increase the risk of OA. If you have bone edema then the bone is upset due to the increase in pressure or force it is subject to because of the tear. Running is often well tolerated in knees with these degenerative tears in the posterior horn. But it may take up to one year for the knee joint to settle down. Since I have not seen your images, Xrays, etc I cannot say what the best course of action is. In this format I cannot recommend treatments or activities either… advice is a tricky thing on the internet.
Rob N. Preston
Thank You!
Rob
Hi Dr Luks,
In June 2017 I was diagnosed with a posterior horn medial meniscus tear in the left knee. I was 45 at the time and the tear came about while running and turning on uneven ground.
I was referred to a surgeon who said he’d address the tear and I’d be back running in 2 months. I awoke from the operation to be told he removed 60% of the posterior horn part of the meniscus as it was getting stuck in the joint. 2 years on and I’ve never been able to run a few metres due to intense pain.
He scheduled a microfracture surgery last month only to discover it’s too far gone with large legions of exposed bone and recommends a knee replacement. I’m devastated this gas occured and I believe I was misled into surgery. Are there any options to avoid this?
I’ve been advised to have pentosan treatment to reduce bone Edema and this will allow me to be reasonably active. What are your thoughts.
HI Rob.. I’m sorry that you’re no longer running :-( Also sorry to say that I have no experience with Pentosan for the treatment of bone marrow edema.