
 A recent article in the New England Journal of Medicine has attracted a lot of attention… and it should. The article focused on a group of patients with meniscus tears and osteoarthritis. The goal of the study was to determine whether or not surgery was necessary when compared to a group of patients who only had physical therapy. Although it was not the best study possible, the results are encouraging…. depending on your perspective :-) Physical therapy is equally effective at treating patients with both meniscus tears and osteoarthritis as surgery is. Imagine that!
A recent article in the New England Journal of Medicine has attracted a lot of attention… and it should. The article focused on a group of patients with meniscus tears and osteoarthritis. The goal of the study was to determine whether or not surgery was necessary when compared to a group of patients who only had physical therapy. Although it was not the best study possible, the results are encouraging…. depending on your perspective :-) Physical therapy is equally effective at treating patients with both meniscus tears and osteoarthritis as surgery is. Imagine that!
The issues, however, run deeper than those studied by the authors. Those issues include:
- Why were the MRIs performed in the first place?
- Why is it easier to get permission for an MRI and surgery than it is to get permission for physical therapy?
- Kudos to Dr Jen Gunter for her thoughts on this!
- Why do many patients expect an MRI for every joint ache or pain?
- Why do providers agree to order that MRI?
- Are we treating MRI findings— or are we treating patients?
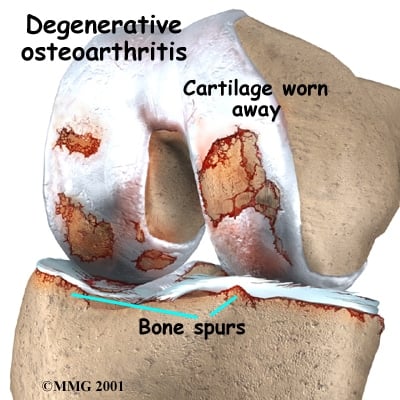
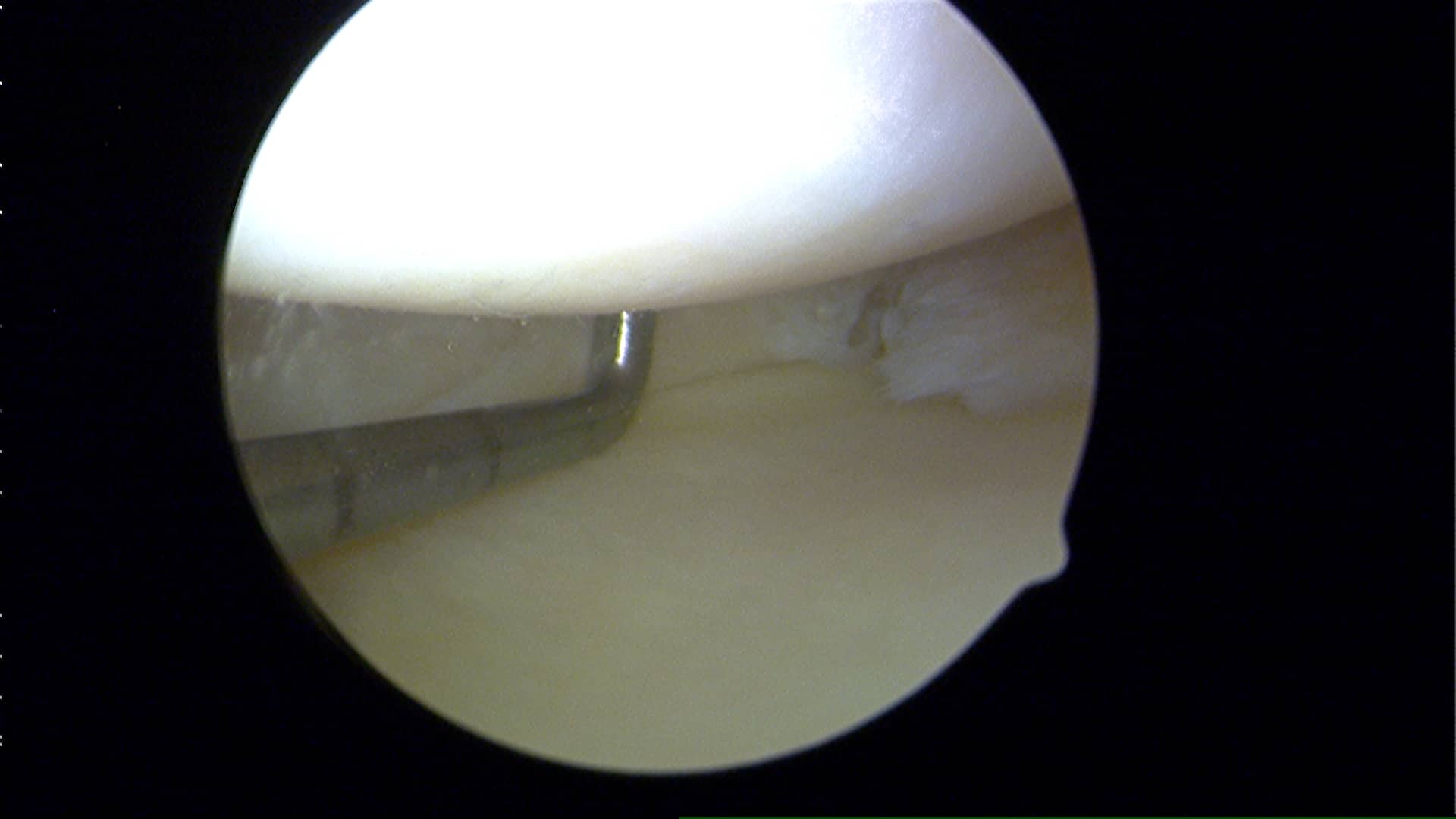 A meniscus is a cushioning disc found within our knee. We actually have two menisci. Osteoarthritis involves the loss of “articular” cartilage from the ends of our bones. As that cartilage erodes away our bones become exposed, and when the bones on opposing sides of the joint rub together… it hurts — occasionally it hurts A LOT.
A meniscus is a cushioning disc found within our knee. We actually have two menisci. Osteoarthritis involves the loss of “articular” cartilage from the ends of our bones. As that cartilage erodes away our bones become exposed, and when the bones on opposing sides of the joint rub together… it hurts — occasionally it hurts A LOT.
What most people in their 40s and up do not realize is that many of you have meniscus tears, and perhaps even a rotator cuff tear and yet you have no pain. Which meniscus tears hurt and why is an area we’re still studying. There are many different types of meniscus tears. Most tears are degenerative because our parts wear out… and surgery for degenerative tears without loose flaps is very rarely necessary.
If you sustain an injury and your knee hurts… you stand a really good chance of feeling better if you allow the body to heal itself. On occasion we need some assistance and that might mean a visit to your primary care doctor. Hopefully your provider can offer you some tips to set you on the path to recovery… but very rarely should an MRI be ordered (or asked for) soon after the initial injury. MRI’s should be used to confirm diagnoses… not to make a diagnosis. They are most useful if you have failed non-surgical treatment and we are considering surgery. Even in the realm of professional athlete injury management the issue of over-utilization of MRIs has gained a lot of attention .
Given the insight gleaned from this paper, your primary care doctor should likely start you in physical therapy if they suspect that you have suffered a meniscus tear, and your X-rays show evidence of arthritis. But our primary care docs are getting squeezed… they need to see too many people each and every day just to be able to keep their doors open. That leads to rushed visits, easy scripts for MRIs and premature referrals to specialists. That opens the door for a specialist to then recommend an operation based on the MRI findings… and not necessarily because they are treating you as a patient. Many variables need to be considered whenever surgery is being thought of as the primary treatment modality. Your MRI finding is but one small consideration in that “shared decision making process“.
The big picture… many patients will have meniscus tears that will marginally affect their quality of life, if at all. Not all weekend injuries require an MRI … time heals most injuries alone. Surgery is not necessary for all meniscus tears. Doctors need to commit to be willing to spend as much time talking about the non-surgical treatments for meniscus tears as they do trying to explain what the surgery entails. While surgery might ultimately prove to be the proper course of treatment to pursue for certain meniscus tear… it should only follow a course of failed non-surgical treatments for your meniscus tear and osteoarthritis.
Do you have questions regarding an Orthopedic injury or longevity?
Do you want to talk to an expert who can listen to you for 45-60 minutes and explain the options in detail?
Dr. Howard Luks offers remote guidance sessions to review your X-ray or MRI images and explain your options.
Dr. Luks has also received hundreds of requests for educational sessions on the topics discussed in his book, Longevity Simplified.
Questions? Why don’t you come in and discuss your options. :-)








Shawna
If I bend my knees too far, they lock with excruciating pain until someone straightens it . POP… then the pain eases to an ache. That is the always problem, now I can’t straighten my left knee because it’s like it is going too far and I’m in constant pain if it’s semi bent for too long or standing too long. There seems to be no happy medium. I have as of late tied a bandana tightly around my knee under the cap and it seems to have ‘secured’ it somehow. I’m not dragging my leg behind me for a change. I hope that can help someone in a similar case, but would more so like to know what the cause is, and what can be done!
Darlene Jill
I had surgery for meniscus tear (no arthritis). So glad I did.
So glad to hear you are doing well. Knee pain due to meniscal tears without arthritis often will improve significantly after an arthroscopy.
Anita Millard
Thanks again. Nice to get a confirmation of what I was thinking!
Anita Millard
Thank you so much for your honest reply. I asked my stem cell doctor for proof that the injections work and he referred me to Regenexx study of their approximately 2000 patients which showed 45-75% mprovements in 1-3 years in mobility and pain. I wish it had been an independant study.
Regnenexx doesn’t perform randomized control trials. The placebo effect is strong. So 50% or more can believe they are better when injected with only saline.
Anita Millard
I enjoyed your article also. I have severe OA in both my knees. I have seen two orthopedic doctors. The one does stem cell therapy using the patients own stem cells. He has told me I mainly have one compartment affected by OA but since the other two compartments have some cartilage among other things I qualify for stem cell therapy. The other Doctor recommends total joint replacements as he says I have bone on bone disease with medial bone spurs on both knees. I tore my meniscus in the last week so he gave me a cortisone shot. I saw my xrays and I do have some space between my femur and tibia in the two compartments but not the medial aspects due to the bone spurs. I would love to have the stem cell therapy but my concern is it won’t work. Would I have to have a repeat of the therapy? It costs $5,000 per knee which would be out of pocket for me. So what do you think?
The future of stem cells is very bright in orthopedic conditions. Unfortunately the science just doesn’t support their use right now. The stem cells/PRP injections for most patients becomes an expensive bridge to an eventual knee replacement. The placebo effect of nearly any treatment means that up to 50% of patients will respond favorably to the injection of anything (saline)- as long as they think it is going to work. It is a difficult decision to make. Ask your stem cell doctor to show you evidence of their methods and how well it has worked.
Dara
Hi Doctor, I am usually very active and unfortunately injury prone. I ran through the pain in a half marathon in April 2016, medial left knee. Ran light miles in May. Stopped running in June because it wasn’t getting better. Biked all summer with an occasional tester run. Finally went to Doctor in September, he said he thought arthritis but nothing on X-Ray and/or maybe a slight tear to miniscus. Is there any real point of the MRI? Will the knee heal enough to exercise without pain? If I start running again will I just make it worse? Thanks for your time.
For runners with persistent medial pain, a stress reaction or fracture is also a possibility. After a few months of persistent symptoms it’s likely time to see if an MRI helps shed light on your issue.
Lori
Dr. Luks,
My husband has an inside left knee meniscus tear with arthritis and on small bone spur on the other side. Significant arthritis behind the kneecap.
Surgeon read MRI and the X-ray (showed arthritis).
He’s 5’9″, 400 lbs, 51 and his BMI is too high to risk knee replacement surgery. Offered every six months for a year or two cortisone shots.
He injuried it helping someone move it didn’t tear but just was like not stable (11/2015) and it healed around March 2016.
July 4, went to sit down and heard the pop in the knee and X-ray were clean except the arthritis. MRI done two weeks ago…showed the tear and the bone spur and arthritis and very little cushioning on right side of left knee.
Surgeon said no arthroscopic surgery because that will not solve issue because of the right side little cushioning. Because of that recommends knee replacement but will not do it because of BMI and success rate is 75% by year five. Suggested Bariatric surgery and then he would see.
Nothing was offered as PT or brace or not so drastic. He’s working on his weight.
Found this article and a brace (web style) on Better Braces.com.
Would the brace and getting hydro PT help?
And we know the weight loss will to
Opinion?
PT, pool therapy could work well. It might be difficult to fit him with a brace. Weight loss and appropriate lifestyle changes ( no sugar, pool based walking, etc) are critical.
Jean Rajotte
Hi Dr. Luks. It is a very valuable initiative to share your time and expertise to explain the pros and cons of meniscus surgery. I am a 58 years old Canadian male who had partial meniscectomy 15 years ago on my right knee after a hockey injury. Although this knee has always been more fragile or weak during training, il remains pain free. The problem is that I now experience severe pain and instability in my other knee when I make torsion moves or I am descending stairs. Just a light pain when I climb stairs. In line with your recommandations, my doctor does not anticipate the same outcome of meniscectomy on my left knee as OA is likely to be a factor now. The main question is: Can an imagery exam provides a good assessment of the OA on the joint to make a decision or should I undergo an arthroscopy to view the condition of the cartilage? Accessory question: If the surgery does not work, what are the chances that the meniscectomy procedure worsen the symptoms and the evolution of the OA?
Thanks again for your valuable opinions.
Yes… A well performed MRI will show the status of the articular cartilage and whether or not any arthritis is present.
Iaman Alkhalaf
Dr. Luks,
Thank you so much for spending the time to help people and provide insight. I am a 22 years old active male recently diagnosed with meniscus tear as a result of knee twisting whild doing Taekwondo in my right knee. The orthopedic surgeon suggested examining my MRI and then decide to have a surgery or not. I looked at the study linked in Dr.Jen Gunter article and it seems like the study examined the effectiveness of PT for patients above 45 years old. Do you believe that the same conclusion of the study can be applied to younger patients ? How can we draw the line between going for PT and the the necessity of having a surgery ?
Best regards,
Usually no harm in trying PT first.
Thomas Hall
Aloha Dr. Luks,
I am 66 and have remained in good shape as a surfer etc. in Hawaii for the last 40 years. I have recently experienced a torn meniscus. My surgeon has given me advise to not have surgery because of my meniscus showing older damage and scaring (and the fact that I have arthritis present). It has been 3 months now and my knee has gotten a bit better BUT it occasionally gives out because of pain and a feeling that something is catching between the joint. The severe pain only lasts 5 or 10 minutes and then I am only dealing with the tenderness and am able to walk again. My question is: I can’t tell what is causing the episodes. I haven’t been able to completely bend my knee over the last 3 months (without pain, popping and crackling) and I am concerned that the meniscus is catching in between my joint and causing the problem. Would it be beneficial to have the floating parts removed or is the arthritis a factor (as my doctor mentioned) that superceeds any surgery efforts?
Thanks for your help.Tom
Great question … your surgeon is correct. Tread lightly when arthritis is present, especially if it is moderate or severe. If it is mild to moderate in severity and your instability persists then it is ok to consider an arthroscopy as long as you clearly understand that it may not work. IF the arthritis is severe and the knee is bone on bone, then an arthroscopy will not help you.
Good Luck
Allison Green
MRI shows a medial posterior meniscus tear, I am 80, one doctor says go as long as can before a total knee repair as orthoscopic would make it worse, another doctor ( fellowship train, and young) says a 15 minute orthoscopic surgery would keep the tear from getting worse. It catches and I walk stiff leg at times .There is pain. what is right? Primary doctor says PT. Time and travel is a problem. WHAT SAY YOU/
At 80… most arthroscopic surgeries do not end well. If there is significant arthritic change, then an arthroscopy has a chance of not working well. plus, the risk of stress fractures after surgery increase due to osteoporosis too. Difficult decisions, without examining you I can not offer specific advice
kripsal
Dr Luks,
i am 19 years old and have had a lateral meniscus tear for about 3 years. i am ok with light sports like running or gym exercizes but when i try to play football again. i get massive inflammation which leaves me in pain and unable to walk without a limp for about a week after playing. from reading many articles im am not sure what to do as i have read getting the meniscus repaired leads to early arthritis but not doing so can also do the same. would really appreciate your opinion on the matter. Thanks
Hi ! I would love to help you with your questions. You can find me on Curely where I can answer questions by text or email … Join me there. http://www.curely.co/
joyce swartz
twisted my knee as I fell. ortho doc said treating meniscus makes oa worse. true?
It is possible …
Darlene Jill
I had surgery for it. Fixed it. Off of crutches in two days. Worth it.
Jane
I am 11 weeks out from meniscal repair. I have severe OA in both knees. My insurance has just approved Supartz (3 injection in each knee). I have had 16 PT sessions and there is conflict about how I should exercise,the PA says no walking unless I have to,the PT says to walk 2-3 miles a day. How do I know what to do without worsening the OA in the knees?
Your OA will worsen no matter what you do. That’s the natural history of it. Inactivity is very bad for your health.. and most arthritic knees actually like to move.
fabienzan
Thanks for your reply. Taking my example again. I have 2 small tears in the lateral meniscus and 1 of 1.2 cm on the posterior horn of the medial meniscus. All 3 were left in situ at surgery time, my surgeon mentioned that he might have to go back and do something about the medial meniscus tear if it propagate and become an issue. Why take this risky approach and not repair it or trim it at the time of surgery ? Is it better to keep a torn meniscus asymptomatic or with very little symptom or do a partial menisectomy ? I read that a meniscus tear can lead to Chondromalcia if left untreated ? Is a tear left in situ more protective of my join even if reasonably large like 1.2 cm than doing a partial menisectomy ?
My age again is 43.
fabienzan
In the case of an ACL tear and meniscus tear . During knee reconstruction how do you know which meniscus tears if there are more than one are degenerative and or acute ? Is that only based on the symptoms given by the patient ? What happens if the patient is not clear about the symptoms based on the fact that there is a lot going on in the knee after an acl tear.
Great question… At the time of surgery we are able to tell. We assess the quality of the meniscus itself (soft or firm: frayed or a clear tear), the location of the tear, the type of tear and can determine if it is repairable or not. A lot of attention recently has been focused on fixing tears we once believed would not heal — such as horizontal cleavage tears.
fabienzan
Thanks. Howard for your reply. How do you base your decision at surgery time ? For example before surgery I thought I didn’t have any symptoms as I was walking in straight line. Now I am for example crossing my legs and can feel some pain on the inside of the knee ( I assume this could be my medial meniscus tear). I am a bit paranoid about getting OA as I am only 43 and active. My surgeon also said that at my age a suture was probably not going to work as I am too old. Is it not worthwhile trying or is it doomed to fail anyway. My thought behind this is if it works then I have a fully functional medial meniscus instead .
What are the risks of leaving a large tear in situ ? Is it still better than doing a partial menisectomy ?
I am reading that the progronosis of getting OA after knee reconstruction and partial menisectomy is very high but if the meniscus is intact then it is not much better.
fabienzan
Dr Howard,
I have just seen my surgeon (1 month) post op after acl and meniscus tear injury.
He reconstructed my ACL (I am 43) and left untouched 2 small tears of the lateral meniscus and one 1.2 cm tear of the medial meniscus. My question is how would the lateral tear affect me (arthritis wise in the future . Are they likely to increase even so they appear to be really small ?)
Also how significant is a 1.2 cm medial meniscus tear left unrepaired ? My surgeon mentioned that I might need surgery to repair it in the future as it might get bigger.
At the moment I would say this tear is slightly symptomatic but not much. My physio said that as part of my rehab I will do some cycling which is likely to smooth the edge of the tear and make it none symptomatic. Is that correct ?
Also with a large medial meniscus tear is that likely to affect how my meniscus work and created OA in the near future ?
Some tears we know if left alone will heal or likely not bother you. Some tears we need to treat. That’s a judgement call at the time of surgery.
Good Luck
Sally
I am happy to read this article, I was just told that I have meniscus tears and arthritis on both knees and the first course of action was surgery.
I declined and asked that to be the last resort. This article makes me feel comfortable with that decision.
Thanks
Fabio
Nice article!! I see this things a lot in my chiropractic practice!!!
Thanks for stopping by Fabio. I have this discussion 20 times a week. Glad to see there’s evidence coming out in support of non-operative care for meniscus tears in the setting of concomitant osteoarthritis.
Veethika
Dr Luks
I have been watching some of your videos online about meniscus tears.
I was recently diagnosed with a meniscus tear (using MRI). I have RA and not osteoarthritis. I am 44 yrs old. My knee filled with fluid and my doctor extracted it twice over 2 weeks. The third time he recommended and MRI. I do not have pain in the knee but there is some fluid. I also take pain meds for RA so I am not sure if that suppresses the knee pain.
My report reads as -” Posterior horn medial meniscal tear, small joint effusion. There is a vertically oriented signal in the posterior horn of the medial meniscus communicating with the tibial and femoral articular surface. No displaced meniscal tissue is present. There is mild thinning of the articular cartilage of the medial compartment without focal chondral defect or osteochondral lesion. the medial collateral ligament is intact. The lateral meniscus is intact. Mild Marginal spurring of the lateral femoral condyle is present”
I am wearing a knee brace to avoid surgery immediately. I am avoiding any activity that will put stress on the knee. Will I be a candidate for arthroscopy?. It has been about a week with the brace. How long should I wait before deciding on a surgery or get the fluid extracted again? Is it any different if I have RA and not osteoarthritis?
Thanks for reading and your time.