
A partial ACL tear is an incomplete tear or injury to the anterior cruciate ligament (ACL). Partial ACL injuries might be treated differently than a complete tear of the ACL. Recovery from a partial ACL tear might be faster than the recovery from a full tear, but it is also a much more complicated decision-making and treatment process. There is a number of variables and considerations that require careful attention in determining how we might treat a partial ACL tear. The goal of the treatment is to minimize the risk of having instability or giving-way episodes.
Why do Partial ACL injuries occur?
Most ACL tears occur from non-contact injuries. When you turn, pivot or twist and you feel a pop or tear inside the knee, then there is a chance you injured your ACL. That injury could be a “partial tear” or a “complete tear” of the ACL. Injuries to the ACL or Anterior Cruciate Ligament are becoming more and more common. The ACL is composed of two pieces, or bundles — so it is possible to suffer only a partial ACL tear, as opposed to a complete ACL rupture.
What is the Anterior Cruciate Ligament (ACL)?
 The anterior cruciate ligament (ACL) is one of the more vital and more easily injured ligaments within our knee. Ligaments are very tough, fibrous tissue structures. Ligaments hold our bones together and allow us to bend, twist, pivot and rapidly accelerate and decelerate and yet maintain the stability of our joints. The ligaments of our knee hold it together. Most ACL ligament injuries in the knee are non-contact in nature.
The anterior cruciate ligament (ACL) is one of the more vital and more easily injured ligaments within our knee. Ligaments are very tough, fibrous tissue structures. Ligaments hold our bones together and allow us to bend, twist, pivot and rapidly accelerate and decelerate and yet maintain the stability of our joints. The ligaments of our knee hold it together. Most ACL ligament injuries in the knee are non-contact in nature.

If you have sustained an injury to your knee during a pivoting, or twisting incident, you felt a pop and then noted the inability to walk — as well as significant swelling within your knee — there is a significant chance that you have injured your anterior cruciate ligament.
The anterior cruciate ligament or ACL is the most commonly injured of the four major ligaments that exist within our knee. The ACL is a large ligament composed of two “bundles”. Therefore injuries can lead to a partial (one bundle) ACL tear or a complete ACL tear (both bundles). A good examination by your doctor can often tell the difference between a partial ACL tear and a complete tear. Often times, you will be referred for an MRI to confirm the diagnosis.
Complete ACL Tears:
A complete ACL tear involves the complete disruption of all of the ligament tissue that connected both the femur and tibia. You may simply possess discomfort, pain, and swelling – – – or you may perceive that the knee is unstable and feels like your knee wants to buckle or give way. We have covered the treatment of complete ACL tears elsewhere within this website, and whether or not ACL surgery is necessary as well. I recently placed two ACL Surgery blog posts on this site. The first will help you determine if ACL Surgery is necessary and what questions you should ask your surgeon. And a follow-through post of steps you should take before surgery and after surgery to minimize the risks of complications and improve your overall results following an ACL reconstruction.
Partial ACL Tears
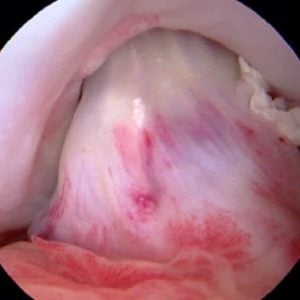
A partial ACL tear involves an injury to only a portion of the ACL. The normal ligament has an Anteromedial bundle and a Posterolateral bundle. A partial injury means that only one of the two bundles was torn. Therefore, the second bundle is intact. Many patients who sustain a partial ACL tear will be able to return to their prior level of activity without complaints of buckling, instability or giving way. It may, however, take many months to recover from the injury and to complete the extensive rehabilitation necessary.
Unfortunately, a fair number of you with a partial ACL tear will not be able to return to sports because your knee feels unstable or loose. Therein lies the issue with partial ACL tears … some people with a partial tear will not complain of instability of their knee with sports, but some might.

What I’m getting at is simply the fact that we should not look at your ACL tear as being “partial” or “complete”, we look at your KNEE as being “functional” or “non-functional” or “stable” vs. “unstable”.
If you have a functional and stable partial tear of your ACL, that means that you have torn a certain portion of your ACL fibers, however, you are still able to participate in sports without the feeling of the knee giving way or being unstable. If you possess a nonfunctional partial tear of your ACL, that means that you have torn enough of your ACL fibers that your knee no longer feels stable. That means that you are at risk of further injury if you return to your prior level of sports participation. Every time your knee buckles or gives way you run the risk of tearing other structures within the knee, such as the medial or lateral meniscus. If you sustain tears of either the medial or lateral meniscus, which are the shock absorbers within the knee, then you are at risk of developing osteoarthritis. You, therefore, want to eliminate or minimize the risk of buckling, instability or giving way and therefore a patient who presents with a partial ACL tear, who complains of instability, will likely present as an appropriate candidate to consider an ACL reconstruction or possibly an ACL augmentation.
ACL Repair and Treatment Options – If Partial ACL tear surgery is necessary
The difference between an ACL reconstruction and an ACL augmentation is fairly simple. During the process of an ACL reconstruction, we will reconstruct or replace the entire ruptured ligament. Anatomically, the ACL is composed of two separate bundles and a complete reconstruction will compensate for both of those bundles. In an ACL augmentation, you have only sustained a partial tear. That means that a portion of your ACL remains intact and should be normal. Many competent sports medicine orthopedic surgeons are capable of reconstructing only the torn portion of the ligament, leaving the normal portion alone. There are many advantages to an ACL partial tear augmentation over a full ACL reconstruction. While the discomfort and the nature of the surgery are virtually identical – – – it is far more likely that someone who undergoes an augmentation will have a much more natural feeling knee when all is said and done. The reason for that is because the normal ACL has certain nerves within it. Those nerve fibers give the brain certain feedback as to the position of the knee joint. It turns out that those nerve fibers are quite important. If we preserve the intact portion of your ACL, then we are preserving those nerve fibers and hopefully preserving the integrity of your knee in the long run.
In some published series, up to 50% of athletes can be expected to return to sports with a partial ACL tear which is treated without surgery. Before returning to sports, an athlete should complete a formal rehabilitation program. A thorough evaluation by your doctor, physical therapist or athletic trainer should also be performed to make sure that your knee is properly rehabilitated and ready to return to the field.













Hello i am a 15 year old male, i had an ACL operation and it was successful. After 3 and a half months i tore my acl again should i do the operation? i play in a professional soccer team.
How did you re-tear it? Did you go back to sports after only 3 months ?? What graft was used?
If you felt like you needed the first ACL reconstruction, why would that change after a second tear? It is unlikely that a teenager could return to professional level sports without a functioning ACL.
Good Luck
Howard Luks
Hi Dr. Luks,
I am 25 years old from Jakarta, Indonesia. I am so glad that I found your article in this website. Well, first I’ll tell my diagnosis story on my Right Knee injury. I currently living in Guangzhou, China. I am a very active person in martial arts, fitness & other sports. 5 months ago I injured my ACL & some part in the Meniscus because of the jiujitsu training. At first, I checked with the 2 Chinese orthopedics back when I got my injury, at first the doctor didn’t give any further physical exam, & ask the MRI for further diagnosis – yet, both of the doctor didn’t do the physical exam on my knee – suggesting to wear leg brace (not knee brace – if you know what I mean). All they do is based on the MRI results, which I believed what they diagnosed that, I had complete torn on my ACL & suggested to do the surgery. Well, in that time they didn’t suggest to do it directly, because I still had my swelling in the knee. After 3 weeks I had a chance to go back to Jakarta, & then I immediately went to my trusted orthopedic, and yes he did the physical exam with the McMurray test, & diagnosed me with a partially torn after the exam (found the stiffness in the muscle on that time). More, he gave me the injections of “calcitonin” like 3 times a week without any charges (he’s a social doctor too FYI), yet he saw my MRI result, but what he commented on the result is that he couldn’t just believe what MRI report told, he needs to do the physical exam more. Right now, i am able to walk normally, bending, and putting the heel into my butt, however then I checked again with another Indonesian doctor and he diagnosed that its a complete torn & need surgery, without doing any physical exam too (as like the Chinese). Well, i still got lots of chances to saw my trusted orthopedic more often & he still did more physical tests during the i always visited him. He suggested to always wear the knee brace until it naturally healed & restored (it might not be 100% restored he said, but its better than the surgery) – the process might take 6-9 months he said.
But still I’ve complaints – I still have pain sometimes when I tried to even jogging, walk on the stairs, & felt unstable sometimes (not everytime). I still wear my knee brace & try to come back to train again in jiujitsu, but again some twisting movement or more active movements I didn’t do it, but since I can feel the pain during I actively move/run – I rest to train jiujitsu, let it be restored completely, and waiting.
So, right now I am still confuse whether I need the surgery or not.
What is your thoughts for me, if you were me? Hoping that you can suggest some more details information too.
Thank you.
JANSEN-
Hi Jansen… what was the reading or impression on the MRI?
Hi Dr. Luks,
The MRI reading was a translation like this;
“Result of right knee MRI plain scan
1. The ACL was completely torn. The PCL, MCL & LCL were partially torn. Anterior angle of meniscus was torn.
2. Internal condyle, lateral condyle of right femur & lateral tibial plateau were focal bone marrow edema.
3. The right knee was hydrops articuli.”
These are all I got – but what the physical exam result was completely different.
However, I am still confuse now.