
Root tears of the medial meniscus are being recognized on an MRI with increasing frequency. Most of you who have a root tear do not recall an injury to your knee. That is a degenerative meniscus root tear. A handful of you had a significant sports-related injury or ACL tear and find that you also have a root tear. How we treat these meniscus root tears will depend a lot on your age, how your tear occurred, the location of your root tear, and whether or not anything else is injured.
A root tear of the medial meniscus is a unique tear. Repairing a root tear of the medial meniscus requires a very different approach than a traditional meniscal repair. Root tears that occur after trauma and an ACL tear will require a meniscus root repair. This is in contrast to the more common degenerative root tear. Some degenerative root tears will benefit from a repair, and some may not. We can help guide you through that decision making. This article will discuss what root tears of the meniscus are and the thought process behind how we treat them.
The meniscus is a c-shaped cartilage cushion in the knee joint. It functions as a shock absorber and a stabilizer. Tears of the meniscus are prevalent. Root tears are not very common, but they are increasingly being recognized as a cause of severe arthritis. Your doctor must be well versed in root tears since they behave much differently than a typical meniscus tear.
What is the “Root” of the Meniscus?
The meniscus is attached or anchored to the tibia by two “roots.” There is a root attachment in the front of the meniscus and a root attachment in the back (posterior) of the meniscus. In most injuries, it is the posterior root attachment that is torn. Problems arise with root tears because if the root of the meniscus is torn, then the entire meniscus becomes non-functional. In other words, the meniscus needs to be well anchored to the tibia to function as a shock absorber.
How Did I Tear The Root of the Meniscus?
Many meniscus root tears occur as a result of trauma. Some root tears occur at the same time you tore your ACL. Other common causes of root tears might be a fall, slip on ice, or related to a sports injury. As we age, it is easier to tear the root of the meniscus, especially the medial meniscus root. Therefore you may tear the root by merely kneeling or squatting down. The average age of patients with root tears in my practice is between 25 and 65. The younger patients tend to have lateral root tears in association with ACL tears. The older patients tend to have medial root tears in association with early arthritic changes. Root tears that occur in association or with coexisting osteoarthritis are the most common form of root tear seen by orthopedic surgeons. Most of you will note that you knelt, bent your knee or twisted, felt a pop, and then noted increasingly more severe pain in the knee.
Patients with root tears of the medial meniscus often complain of giving way or instability. They are fearful that the knee will buckle or give-out. The onset of pain is often abrupt, and the pain is usually on the inner side of the knee, or in the back of the knee.
How Do You Fix A Root Tear of the meniscus?
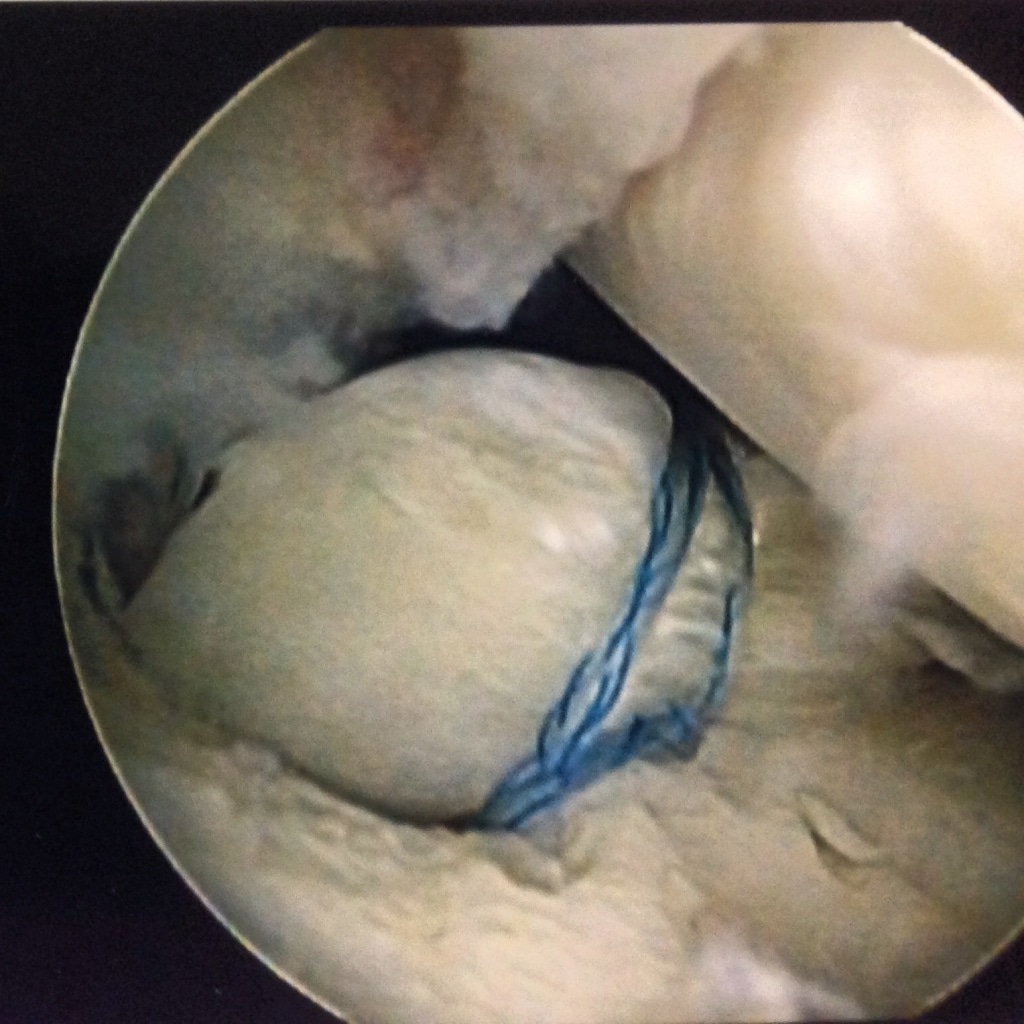 To fix the root of the meniscus, we need to pull the root against the tibia in the same place where the root was before your injury. The procedure is mostly arthroscopic. It is a technically challenging procedure, so please be sure that your physician has performed many of these. After we put a suture around the root of the meniscus, we drill a hole from the front of your tibia into the root area. We then bring the stitches out through the hole and tie them over the front of the tibia. Therefore we are pulling the root down into the tibia, and the stitching will hold it in place until it heals. In the picture above, you can see how the stitch is through the root of the meniscus, and the meniscus is being pulled down into a small hole I created to encourage healing.
To fix the root of the meniscus, we need to pull the root against the tibia in the same place where the root was before your injury. The procedure is mostly arthroscopic. It is a technically challenging procedure, so please be sure that your physician has performed many of these. After we put a suture around the root of the meniscus, we drill a hole from the front of your tibia into the root area. We then bring the stitches out through the hole and tie them over the front of the tibia. Therefore we are pulling the root down into the tibia, and the stitching will hold it in place until it heals. In the picture above, you can see how the stitch is through the root of the meniscus, and the meniscus is being pulled down into a small hole I created to encourage healing.
Do All Meniscus Root Tears Need Surgery?
The body of evidence about the treatment of root tears of the meniscus is growing. There is a generalized agreement that most medial root tears that occur in the setting of moderate or severe osteoarthritis should not be fixed. In these cases, the meniscus is usually degenerative or wearing out. Studies have shown that if these tears are fixed, they will commonly tear again in a very short time frame. If the arthritis is severe, then fixing the root tear may not alleviate your pain.
Root tears that occur in a severely arthritic knee should be treated with relative rest. Some of you may require a walker or crutches for limited weight-bearing. Many will benefit from the use of a compression sleeve, and after a month, a course of physical therapy.
Medial root tears with minimal osteoarthritis should likely be fixed or repaired. A successful repair will eliminate the sense of the knee giving way or feeling unstable. More importantly, fixing a medial meniscus root tear might slow the progression of osteoarthritis. But the critical issue here is that the severity of arthritis in the knee should be mild/moderate.
Root tears and ACL tears often occur together
Meniscus root tears often occur when you tear your ACL. If you have a traumatic root tear due to a severe injury, there is agreement amongst sports surgeons and orthopedic surgeons that these tears should be repaired at the same time that the ligament is reconstructed.
Do root repairs heal well?
Some studies show that a high percentage of these root repairs are successful, and there are studies that show that the success rate might be far lower. Many factors will often determine the success rate. First is whether or not you have anything else wrong with your joint… such as osteoarthritis. Other reasons for failure include lack of biological healing, resuming activities too quickly leading to a new tear, and over-tightening the repair, which could lead to a new tear somewhere else.
Bottom Line:
Do you have questions regarding an Orthopedic injury or longevity?
Do you want to talk to an expert who can listen to you for 45-60 minutes and explain the options in detail?
Dr. Howard Luks offers remote guidance sessions to review your X-ray or MRI images and explain your options.
Dr. Luks has also received hundreds of requests for educational sessions on the topics discussed in his book, Longevity Simplified.
If you have a root tear as a result of a traumatic injury, be sure you see a Sports Medicine Trained Orthopedic Surgeon with experience repairing meniscus root tears. Some tears might be considered for repair, and others may not. IF you have osteoarthritis, and it is moderately severe, then having surgery for your root tear might not be advisable.
Hopefully, this has improved your understanding of meniscus root tears of the medial meniscus. Here is a review of root tears that might be worth reviewing.






Amber Berry
Hi Dr Luks,
I am 54 years old. While I was exercising I hurt my knee. The MRI revealed a root meniscus tear. The surgeon stated I do not have arthritis and I am a candidate for a repair. The recovery requires 6 weeks non weight bearing. Based on the research that is available to you- is it worth it? Will it prevent a knee replacement in the future? Thank you
If the tear isn’t degenerative and appears to be repairable, the sports medicine community would consider repairing these in the non-arthritic knee. Yes.. NWB is 6 weeks and not bening beyond 90 degrees for 4 weeks is advised. Yes.. there is literature to support that the risk of OA is lower after a successful repair– the risk isn’t zero, but it is lower than if it isn’t repaired.
Amber Berry
Dear Dr Luks,
Thank you so much for your help. I ready as appreciate it. Have a good day.
John
Dr. Luks,
56 y.o., very active runner, etc. Landed hard at bottom of stairs with pain and swelling. Dx medial meniscus posterior root tear with extrusion (mild OA also). Dull AND sharp pain for ~5 weeks, but worked hard at formal P/T. Now pain free, and while I’m not running, I’m working hard on heavy bag (including kicks), which I can live with. Am I fooling myself, or can I continue non-surgically indefinitely?
Doc rec surgery to repair, but I would like to continue as is since I feel great. What do you think?
Really tough call… When we determine who to repair we look at the person, the quality of the meniscus, the articular cartilage and the bone. Some root tears shouldn’t be repaired, because they will not heal. if the tissue is robust, and the OA truly is mild then a repair MIGHT be the right thing to do. Complete root tears can lead to severe OA… but failed repairs are common if we do not assess these cases very stringently and stick to strict criteria.
So.. I cannot tell you if you should or shouldn’t have the surgery. But I would consider a few different opinions.
John
It’s very kind of you to respond, doctor. I will seek a second opinion. We have some good doctors in my area of the South.
Tiffany
My husband is 53 yo who runs approximately 15 miles a week and does some cross training and weight lifting as well. He injured his knee about a month ago. Still having pain when walking some distance. He is healthy, not overweight and has never had knee problems before. No arthritis that he knows of. The pain he is currently having is mostly on the medial side of his knee.
His MRI states:
“Medial Meniscus: Body of the medial meniscus is mildly extruded. Large radial tear of the junction of the posterior horn and root (series 6, image 20). There is also free edge tearing of the posterior horn.Lateral Meniscus: No significant abnormality.Patellofemoral Extensor Mechanism and Hoffa’s fat: No significant abnormality.Joint Effusion and Baker’s Cyst: Trace joint effusion is present with a small popliteal fossa cyst.Cartilage: Mild chondral thinning and partial-thickness chondral loss within the trochlear cartilage centrally. Mild chondral thinning within the medial femoral condyle.Bone Marrow: There is a subchondral insufficiency fracture within the medial femoral condyle with moderate bone marrow edema.Muscles: No significant abnormality.Subcutaneous soft tissues: Soft tissue edema greatest along the medial aspect of the knee.Additional Findings: None.IMPRESSION:1. Subchondral insufficiency fracture within the medial femoral condyle with moderate bone marrow edema.2. Tearing of the posterior horn of the medial meniscus. The body is mildly extruded.3. Trace joint effusion and small popliteal fossa cyst.4. Soft tissue edema greatest along the medial knee”
We met with a knee surgeon and he has recommended a partial meniscectomy with subchondroplasty. I am hesitant, but my husband wants to move forward since the doctor told him he would be feeling better and back on his feet relatively soon and led him to believe he would be able to continue running. Running is very important to my husband. I am reading different things about his injury, some say repair, some say no surgery, etc. This particular surgeon said repair in his case is not an option because where the meniscus is torn will not heal. My question for you is, is a partial meniscectomy and subchondroplasty a good idea in this case or should he consider not having surgery right now and rest for a while longer and see how it feels, or should we seek out another surgeon to look at a repair if that is possible. Surgery has been scheduled for October 15th any advice you have would be most appreciated.
Thank you!
I would be very leary about moving forward with a partial menisectomy. There are many of us who actively pursue repairing these… or suturing them. The stress fracture will heal without the need for a subchondroplasty. If those get infected it can be a nightmare. His main concern should be the integrity of the meniscus and thus the risk for arthritis. Right now his risk of developing OA is very high. Removing the torn part will not alter the risk of developing OA. Now, the meniscus may ultimately prove that it is not repairable… but you need to find a sports doc whose primary goal is to repair or suture the meniscus back together.
Tiffany
Thank you for the quick reply! We may be hard pressed to find a surgeon in our area that will do a repair, but we will keep looking. If we go with a conservative approach (no surgery or subchondroplasty) should he be non weight bearing or use crutches as much as he can? How long does a subchondral fracture take to heal on average?
M Allison
Thank you Dr. Luks for all this information. I’m 67, overweight and losing, working out slowing and increasing to become more fit. Lots of quad work and some squats. Had some pain in right knee but assumed osteoarthritis. Kept going with stairs and bike and elliptical. On Easter, popped my knee going upstairs. Can’t put weight on it. MRI: Findings suggestive of a meniscal tear at the root attachment of the posterior horn medial meniscus. Mild medial subluxation of the body of the medial meniscus, and mild free edge fraying of the body medial meniscus. Free edge tear involving the body of the lateral meniscus. Complex meniscal tear involving the anterior aspect of the posterior horn lateral meniscus near its root attachment. Scoping scheduled in a week with surgeon who recently scoped other knee. Options?
A scope may or may not be a good idea… Hopefully, your surgeon plans on actually repairing (suturing) the root!
M Allison
Sorry Dr. Luks. I thought ‘scope’ was short for arthroscopic repair and not just look. He plans to probably repair the meniscus and remove all the feathers. Thank you for your response.
Susan
What a wealth of info you have relayed. I thank you for that. I had medial meniscus root repair January 31st. I am 68 years old, very active with, according to my orthopedic surgeon, no arthritis. I was non weight hearing for 6 weeks following surgery and have been going to my twice a week. My concern is the pain and swelling behind my knee and on the medial side of my knee. Am I hoping for too much too soon? How long is normal recovery for a root repair? Thanks for your response.
These recoveries are always longer than we expect…. some swelling is normal. Some pain behind the knee might be normal too. My root repairs take 3-4 months minimum to feel that they are happy after the surgery and are able to return to some sports and activities of daily living. Intense running sports, tennis, etc I usually delay a return to until nearly 6 months after surgery to minimize the risk of reinjury.
Henry
Dr. Luks, what do you think about partial (not complete) chronic/degenrative root tears of the posterior lateral meniscus in younger patients who don’t have any signs of arthritic changes in the knee? A few surgeons have told me that partial root tears cannot be repaired (only complete root tears can be), and that a patient’s options would either be partial meniscectomy or leaving it alone. In general, do you know if this is true, or is it possible to repair a partially-torn posterior lateral meniscus root?
Thanks
Most all of the literature in this area is written about complete root tears. There are no scientific studies on the management of partial root injuries. If it is a partial tear, it might not be the source of your knee pain?
Henry
Dr. Luks,
Thanks for the info; that’s what I figured (in terms of there being no studies that have been conducted on the treatment of partial root tears). The partial root tear actually occurred almost 3 years ago. I probably tore it from running every day. It seems like it has “healed” to the point that the only noticeable symptom is snapping when I twist my foot into the ground (thus twisting the knee as well), along with a loud pop that sometimes occurs when I repeatedly flex and extend the knee (the pop usually occurs just before the knee is fully extended). It doesn’t really hurt, but it does feel like an “adjustment,” almost like popping your knuckles.
I still run 4 days/week (7-9 miles each time). I usually don’t feel any pain at all during the runs, but there may or may not be mild pain (almost like an icy-hot around knee but nothing sharp) feeling later that day. During some weeks, I will be able to do my runs and not experience any pain afterwards, and I will start to think that it is healed. During other weeks, the pain is more noticeable but never severe. It seems to be more likely to get sore afterwards if I ran hills or uneven surfaces. Also, it’s hard to explain, but it sometimes feels more like something small is tugging/pulling at the back of knee, rather than actual pain.
In fact, I would say the pain itself is easily tolerable. I am just afraid of tearing the root even further (a radiologist said he would estimate that the tear was a pretty small portion of the root) or of developing arthritis if I keep running.
The surgeons I have talked to seem to think it is an unusual root tear case (Dr. LaPrade took a look at my x-rays, and his PA told me that it wasn’t a textbook root tear and there was no extrusion). The radiology report also said there was no arthritis and no other issues. It makes me wonder how I got the injury in the first place (never had any other meniscus tears, all ligaments are fine).
Do you think it is a bad idea to keep running without getting surgery? I am 29 and would like to continue to be able to run 4 days/week, so if surgery would be the best alternative to pursue for long-term success, I’ll definitely consider it. So far, one surgeon wanted to do partial meniscectomy immediately then recommended a wait-and-see approach when he looked at a follow-up x-ray a few months later and said it looked “a little better.” Another surgeon said he wouldn’t recommend surgery since the tear is small, unless it gets to the point where it bothers me on a severe level. Of course, even though the pain is mild enough to push through it, I just don’t want to make things worse.
Sheryl Neal
Dr. Luks,
I am a very physically active 57 year old female. I was diagnosed with breast cancer in May 2016 and have undergone chemotherapy, radiation and a lumpectomy in 2016. I have been going through Herceptin Infusions since January 2017. I have developed Osteopenia. I have continued to exercise in whatever form possible throughout my treatment. I had a small right knee meniscus tear that I had repaired in March 2016. In September of this year I felt a pop while walking into a grocery store. I have been diagnosed with a left knee medial meniscus root avulsion with surgery scheduled in 2 weeks. My surgeon wants to do an aspirin regimen for 2 weeks post surgery and my oncologist wants me to take a blood thinner due to a previous DVT during my chemotherapy. Any suggestions?
Thanks,
Sheryl
You need to discuss this at length with your surgeon. I can not comment on this. A prior DVT increases the risk of a future DVT.
Suzanne
Hello, Dr. Luks.
Is a “meniscocapsular separation” the same thing as a root tear? I’m finding little information online about this condition.
I just turned 40 years of age this August. I am female and live in Texas, with a fairly active lifestyle, or at least…it used to be. On April 19th of this year, I bent awkwardly – think bad form on a lunge – and I heard the dreaded pop/snap and knew/felt something was wrong. I was able to walk for about 72 hours after the incident, but, not thereafter.
My MRI Impressions, dated 05/11/17 read:
1. Meniscocapsular tear of the medial meniscus about the posterior horn.
2. Low-grade strain within the medial head gastrocnemius muscle.
3. Very low-grade cartilage within the lateral facet of the patella.
4. Small knee joint effusion.
5. Enchondroma measuring 5.6 mm within the femoral diaphysis.
Everything else, according to the MRI findings, seems intact, normal or relatively preserved. (Though I confess, there’s a nagging dull ache on the top left of my knee cap – is that related to the lateral facet of the patella in the findings? And a dull ache on the back of my knee, as well. I think I’m also possibly developing a Baker’s Cyst at this point).
Despite the pain lessening, which is good, my injury was almost six months ago, and I’m still not recovered. I’ve used mostly crutches in this period of time. Indeed, it took a while for my leg to be able to extend fully/have my foot touch the floor. I saw two separate orthopedists who both opted for conservative treatment. I have done physical therapy which got me back to full flexion. My pain has decreased. I am now able to stand, but I still present with quite a limp when I walk. So, my distances are short. I still cannot climb stairs without assistance and I can still feel that the …inner-mechanics of my knee, if you will…. are “off”. My ortho doctor told me he’ll see me again in November and maybe we’ll see “if surgery is worth the risk”.
I’m quite frustrated if not a bit scared.
Dr. Luks, is a “meniscocapsular separation” the same thing as a “root tear”? And would you advise surgical repair on this or shall I keep going the conservative route and see how I keep progressing? My quality of life has definitely been impinged. I just don’t know if this will ‘heal’ on its own or if I should try surgery to restore the function and kinematics of my knee joint. Also…what’s the proverbial shelf-life of my MRI? I wonder if a new one was taken today, it would show different results.
I truly hope to hear from you.
Thank you in advance for your time and your informative website.
Sincerely,
-Suzanne
So, a menisco-capsular (you might also read about RAMP lesions) separation is not a root tear. An M-C separation is a very peripheral tear of the meniscus. They are rare in 40 somethings… usually adolescents have these. Assuming the radiology read is accurate these are usually very repairable tears. Did your doc agree with the radiologist? I would gather a few opinions on the type of tear… either way, both MC-separations and root tears, in a young active person without arthritic changes are generally amenable to repair.
Good luck
Suzanne
Thank you so much for your reply, Dr. Luks!!
I feel honored….
I am not acquainted with RAMP lesions so…. onward goes my personal research! I had the feeling my injury was a rare case. (My age and my not presenting with any ligament tears being the chief reasons).
My doctor, whom I seem to be visiting every other month or so since April, did agree with the radiologist, at least, with regards to the M-C separation. But, beyond suggesting conservative therapy, nothing else has been mentioned except: “When you return, we’ll decide if surgery is worth the risk”. [guLp]. Sounds….ominous.
I don’t know if six-months is an expected time frame to still be dealing with all of this?… It’s the not being able to walk very well; tenderness/a lump behind my knee; and the slight tenderness at the soft area to the left of my left kneecap that are still lingering. (Obviously, it’s the lack of functionality that I have that’s driving me crazy). I’m very afraid of surgery creating other problems; but, with your reply and my lack of wanting to stay where I’m at, I will move forward.
Many thanks again, Dr. Luks. I wish I could see/thank you in person.
Cheers,
-Suzanne
Allen
Thank you, Dr. Luks, for the great, clear and detailed information on this site and kudos to you for taking time from your busy practice to answer questions.
My wife, age 70,until recently active and in good health, experienced sharp pain in her right knee during her “body pump” exercise class three weeks ago. MRI shows “high-grade complete or near complete tear of the posterior root attachment of the medial meniscus with marrow edema at the posterior root attachment and medical extrusion of the medial meniscal body.” She also has a “focal radial tear in the free edge of the anterior body of the lateral meniscus and suspected undersurface tear in the body of the lateral menuscis.” She has grade 4 chondromalacia of the lateral weightbearing tibial plateau” and “at least 50% thinning of the median ridge and lateral patellar facet articular cartilage as well as the medial weightbearing lateral tibial plateau without full-thickness defects.” The MRI report says all of her ligaments and tendons look OK.
She’s in pain all the time and can barely hobble around. Your blog leads us to think she’s not a good candidate for root repair surgery. Is knee replacement surgery our only option or are there are other options we should look into?
This post might be worth reading too…
Denise
I am a 47 athletic female that is 9 weeks out from a medial meniscus root repair. I was 7 weeks non weight bearing and 2 weeks partial with brace locked and crutches. I have only been one week starting to walk without my brace and still using crutches. Have been religiously performing my exercises and seeing PT 2 to 3 times a week and was feeling strong. Since the brace came off completely my leg is bent and unable to straighten. When walking also stays bent. Have tremendous pain constantly and knee pops and locks. I work hard to straighten sitting for hours on the floor but after an hour in the chair I’m back at square one. I am only able to bend to 90 degrees as well. I see my Ortho next week and will discuss all this but would be interested in your thoughts. Thank you
There’s little I can say from my end. Hopefully your doc addresses your concerns.
Terri Colagross
So much good info here. Thanks. Question for you. After descending 16 flights of stairs 2 days in a row with no initial problem I began to have knee pain 2 days later. It did not resolve so saw my MD. X-RAY showed fluid, no fx, minimal arthritis. Crutches briefly, NSAIDS, rest, brace and ice helped. However, after stopping NSAIDS pain came back. Gave it time and then MD ordered MRI. Showed radial tear at the medial meniscus root with loss of hoop strength. Mod medial tibiofemoral joint arthritis with mild stress marrow edema signal changes and mod joint effusion. My MD is referring me to an ortho doc. My question is X-ray says minimal arthritis. MRI says moderate. Read by 2 different docs. I would love to have this repaired if possible. I am 60 years old. Healthy and active till this! So now I wait for referral and then appointment. What should I be doing so I don’t make things worse? NSAIDS? Rest? I work in a hospital 12 hours a day. Wearing the brace seems to help but pretty tired and painful knee by the end of the day. Thanks for your consideration.
This is a very common “triad”… a root tear in the presence of moderate degenerative changes (the MRI is more sensitive than x-ray) and edema due to stress in the bone from the loss of the meniscus function. Most people with this triad will recover after a few months… most will not need surgery. Surgery to repair root tears in the presence of moderate arthritis fails often enough that we are not very aggressive at surgically managing these tears.
Renee
Is platelet rich plasma a viable non surgical option
Or is this junk science? MRI States focal complex tear of posterior
Horn medial meniscus near the root. Mild medial patellofemoral compartment osteo arthritis. Have tried physical therapy and steroid injection.
There is no evidence that PRP is effective at healing root tears of the mensicus.
Sheila
Hi Doctor Lux, I am a very fit woman in my late 5O’s In great shape and was diagnosed with a complex tearing of the posterior horn of the medial meniscus with tear extensions to both superior and inferior surfaces. I was not impressed with the doctor today and choice 6 weeks of physical therapy before I decide to have surgery. I am impressed with you and your opinion:) I work out 5 times a week and was doing a forward lunge with a 40 pound bar when my Knee popped 5 weeks ago. Of course I have not worked out since and am doing rice, muscle stim, low level laser and minimal stretching until further notice. I am also going to try acupuncture.
Linda Yeager
Dr Dr Luks. I’m female 70, took a fall about six months ago and broke my shoulder. my knees were bruised. Slowly the pain in my right knee has been getting to be more and more of a problem. MRI shows a tear at the root on the inside of my knee. I have a slight narrowing of the space …one doc says mild osteo and another says moderate. I’m going to take your advice and find someone who has done this kind of surgery plenty! Do you know of anyone in the Eugene Oregon area? We are Track Town USA and lots of sport happens here so I’m guessing there might be someone! Thank you.
good luck to you…. hopefully you can find someone who can speak to the advantages / disadvantages of a medial meniscus root repair in your case.
Howard Luks
Elizabeth
Hello Doctor Luks,
I am 55 years old and scheduled for surgery next week. I have a tear of the posterior root of the medial meniscus with associated Meniscal extrusion and degenerative signal extending into the posterior horn and body. Degenerative signal within the anterior root of the lateral meniscus without a discrete tear. Mucoid degeneration of the anterior cruciate ligament and minimal early medial and patellofemoral compartment. I was carrying something heavy when I felt a pop and snap 8 weeks ago. I was on crutches for 3 weeks and felt a little better but once I started walking again the severe pain came back gradually. My Orthopedist is going in to clean it up and if needed perform the root repair based on what he sees. He does about one root repair a month. Is this enough experience? Could this heal if I continue to wait? I just want to get back to normal activity which includes walking 3-4 miles about every other day. I would appreciate your recommendation. Thank you
Root tears will not heal by themselves. However, root repairs, when there is also arthritis present in the knee joint dramatically diminishes the success rate of surgery. Unless a repair is going to be performed, there is no need to consider a “clean out”. Many of these tears are treated without surgery if arthritis is present- because the research shows that time and PT can frequently results in the same degree of improvement. So… if there is minimal or no arthritis a repair is possible and can be considered. If there is significant arthritic change then the repair will likely fail. It can be a tough call. IF your surgeon does one root repair a month, then they are doing more than many orthopedic surgeons.
Brian
Sounds like 90% of the Root tears, where as our ortho Dr suggest repair vs rehab, conflicts with your opinion, which convinces me to not have surgery….
My MRI: Complex Root tear involving the Posterior hrn of medial meniscus which extends to the Posterior Root attachment. 2mm peripheral extrusion of medial meniscus body. Oblique tear involving the inner free margin of Post horn.. bakers cycst , ruptured at one point, fluid… Full thickness articular cart loss involving Medial femoral condyle, large region of full thickness cart loss involving medial tibial platuea… alot of other stuff going on, just to much to transpose from Report…. basically, My knee hurts…..lol….
Good choice… that’s an arthritic knee.
MANGESH SHRIDHAR BHAGWAT
Dr. Luks,
I am Mangesh Bhagwat, India, Amravati, I am 48 year old, working as a Lawyer,
recently to lower down my weight which is 73 kg and to lower LIPID level, I started running for about 4-5 K.M and that i have done about for 10 days with cycling and trekking in jungle, but after some days it have started pain in Right knee, for which my Orthopedic Doctor suggested me MRI of 1.5 T power, which I have done before 1 Week, I have sown MRI to Orthopedic Surgeon at Nagpur, both are well qualified but both suggested me root surgery,
MRI report says that,
Early Changes of medial femorotibial osteoarthrosis
Radial tear of posterior horn of medial meniscus also involving its roots attachment with mild extrusion of the body segment into the medial gutter.
Pl. suggest, whether surgery is best option or conservative treatment. I dont’t want to go for surgery.
This is a very common picture or presentation in an early arthritic knee. We often see these degenerative root tears in the setting of osteoarthritis. Surgery is generally not recommended, or successful once there is extrusion associated with arthritic changes. We usually start treatment with physio, a compression sleeve, and we give the knee 6-8 weeks to see if it improves. It might be better to consider non-impact forms of exercise too — such as a rowing machine, swimming or an elliptical trainer.
Nicole
Here is my MRI results, I’m getting two different option’s, what would your do?
There is a vertical tear near the posterior root medial meniscus with meniscal subluxation. Hyaline cartilage thinning and mild subchondral edema in the medial compartment.
2. Mild edema associated with intact MCL which may be due to recent or chronic strain.
3. Distal quadriceps and proximal infrapatellar tendinopathy.
4. Joint effusion and mild periarticular edema. Small Baker’s cyst.
Very few sports docs would operate on that… The scientific literature and sports medicine community would support non-surgical management. The edema in the bone (swelling of the bone due to stress) is likely what it bothering you. Surgery for the meniscus tear could actually make that pain worse. These root tears occur in an arthritic of degenerative knee. In most cases within 6 weeks you are starting to feel better.
Betty Petron
Great informative article, but doesn’t sound like there is much hope for a meniscus root tear to heal. I’ve had mine for six weeks and there is pain every day! Can a person get a total knee replacement to take care of the problem? Thanks
Most of these tears occur in the setting of an arthritic knee. A knee replacement is the ultimate treatment for painful arthritis that does not respond to any other treatments. This is something you should review with your Orthopedist
Kathy
In Oct 2016 I was diagnosed with a horizontal tear to the inferior articular within the posterior horn of maternal meniscus.I had surgery and have never recover and I am still in severe pain. In Jan 2017 I had a complex tear involving the posterior root and horn of the medial meniscus with large fluid filled defect and radial tear along the medial meniscus..3.5mm of peripheral extrusion. Frayed inferior meniscocapsular ligament. 11 X 21 mm subchondrial sclerosis and subchondral fracture along the medial femoral condyle. High grade partial thickness tear at the proximal origin of the medial collateral ligament. Could you please simplify this for me.Especially a subchondrial fx. and why would this happen when I had surgery.. Thank you for any help you can give me
The subchondral fracture can be thought of as a stress fracture. When you have a meniscus tear, and you also have some arthritis, the bones around the knee see more stress due to the loss of cushioning. Over time that will cause a stress reaction (bone marrow edema) or it can progress to a stress fracture. Unfortunately, this is not uncommon after a meniscus tear develops in a degenerative knee .. or after meniscus surgery.
Page C.
1.Degeneration and tearing of the posterior horn and body
of the medial meniscus including full-thickness or nearly
full-thickness radial tearing of the posterior horn at its
central attachment.
2.Mild free edge truncation/blunting of the body of the
lateral meniscus.
Small joint effusion.
3.Tricompartmental osteophytic spurring with chondromalacia
appearing most advanced involving the patella.
4.Stress reaction without stress fracture involving the
posteromesial aspect of the medial tibial plateau.
Classic MRI findings for a degenerative medial root tear. They usually occur in the setting of an arthritic or degenerative knee. The stress reaction is usually what hurts the most. Cane, crutches or a walker usually necessary to help get the pressure of the bone for a few weeks so the pain calms down. Vast majority of these are treated without surgery.
Good Luck
Brenda Fitzgerald
Im a PT with a few questions regarding post op “protocol” My 56 yo sister has been found to have a root tear (medial and lateral) and it has been suggested that she have a root repair. However, she has a failed TKA on the contralateral side (3 knee replacements in that knee in 3 years severe probs with chronic pain…..flexion 35/ extension -10). If the standard of care is NWB for perhaps 6 weeks….how would you suggest that occur. her contralateral knee quad strength is 2/5, buckles constantly…Im thinking primarily Wheelchair. Am I thinking correctly? She additionally is a single parent (widowed last year) and therefore single income teacher. The MD who saw her says she needs to have this done immediately or risk arthritis…but she is a teacher and can only do NWB for 6 weeks in the summer (her school is an old building and not handicapped accessible)…what is the risk of waiting the 4-5 mos?
Eric Christie
Thank you for the information Dr. Luke. I checked and Dr. Hunter has moved on to Texas. I am going to try to get a consult at the Cleveland clinic as well as one in Pittsburgh. My concern is that the doctors I speak with me not be familiar with or interested in salvaging my meniscus. Do you do any consultations over the phone if diagnostics are sent to you?
Thank you,
Dr. Eric Christie
Eric… There are many of us who are capable of fixing this out there. I do speak with people over the phone/skype — but can not offer formal medical opinions.
Email me at [email protected] if interested.
Eric N Christie
Dr. Luks,
Am I possibly a candidate for a repair? 45 yo male, physician, motorcycle accident 6 months ago. Fractured my right tibial plateau. It was repaired with plates and screws, After 6 weeks of being braced, I began PT and progressed to 115 degrees of knee flexion where I stopped. A MRI showed a medial meniscus extrusion despite the interference from the metal. My hope is that a surgeon can repair this and get me more flexion. I am an avid runner and cyclist and want to do whatever I can to maximize my recovery.
I am in PA and my surgery was performed in Pittsburgh. I am also close to the Cleveland Clinic. Do you have any referrals of doctors in this area.
Thank you,
Eric
Hi Eric..
Root tears of the medial meniscus are often degenerative in nature. Those we tend to treat without surgery.
Root tears that are not associated with OA, and felt to be traumatic can be repaired. A meniscal root repair may not improve your flexion if it is due to arthrofibrosis from the trauma which led to your fracture. Chris Harner in Pittsburgh is worth seeing. I do not know anyone personally in Cleveland. Good Luck
Rex Sidnam
Good day Dr. L. Less than a week ago, an MRI revealed a complex posterior root attachment medial meniscus tear in my R knee. In the data above, you stated, “If the root of the meniscus is torn, then the entire meniscus becomes non-functional. The meniscus needs to be well anchored to the tibia in order to function as a shock absorber.” Then you later stated, “The body of evidence about the treatment of root tears of the meniscus is growing. Three questions…1. If the entire meniscus is non-functional, what does that do to your quality of life? I enjoy hiking. With this tear, if I don’t have surgery, would I ever be able hike again. 2. When you state the body of evidence about treatment is growing, how so? 3. I reside in Fredericksburg VA. Do you have any recommendations regarding Doctors in this area, Richmond VA, or northern VA? Thank you.
Right… in the perfect knee with no evidence of arthritis, then fixing a root tear is advisable. In majority with medial root tears, significant arthritis is also present. Repairing tears in that setting doesn’t treat the arthritis, and the repairs frequently fail. It’s a difficult problem.
Dr Jeff Berg is a quality doc.
Rex Sidnam
Tx Dr L for the insightful expeditious response. One additional question…since the MRI report stated osteoarthritis in my knee, and since you said if arthritis is present, that the repairs frequently fail, what options does a person like me have, who prior to this recent tear was quite active, enjoying mountain climbing, hiking, etc., to be able to enagage in these activities once again? I am 67.5 years young. Thank you.
Rex Sidnam
Dr L, cannot see the Doc until 6 Dec. Since MRI that revealed the complex posterior root attachment medial meniscus tear, I’ve been icing the knee in AM and PM, elevating it when I can, and taking 800mg Motrin every 8 hrs. Prior to my forthcoming appointment, would it be OK to use a recumbent bike for 30 mins daily, and do light leg presses every other day? Thank you.
Lina
Dear Dr. Luks, Scheduled for surgery next week. Now after reading your article I am thinking that I need to meet with my doctor and look at other options. Please let me know what you think. Findings: peripheral 3rd vertical tear at the anterior horn insertion of the medial meniscus with adjacent septated parameniscal cyst. (Will not include all details of size of cyst) – There is tricompartmental osteoarthritis manifested by marginal osteophytes and cartilage abnormalities identified at the patellofemoral compartment. Thank you and God bless you!
I’m sorry that I really can’t say much without examining you and looking at your MRI myself.
I’m sorry that I really can’t say much without examining you and looking at your MRI myself.
Rob
I am a 58 yr male that had medial meniscus repair on left knee in 2014. I started running 26 miles a week as New Years resolution in 2015 and lost 60 pounds and have continued 4 miles x 6 days until several weeks ago with similar right knee pain. MRI resulted in medial meniscus root tear and scheduled for surgery Dec 5. I never thought to ask how many the same that I would never ask any other medical specialty professional. My concern is what I am reading regarding rehabilitation. I am not for crutches at all. I walked (hopped around) 3-4 hrs after my 2014 surgery I don’t have much patience and will reject the notion of no walking more than 1 or 2 days max. This 4-6 weeks stuff is unimaginable for me…not going to happen. That is my only hangup. Can you please tell me your recommended after surgery detail?
HI Rob …
Only a few medial root tears need surgery. If we do repair them it is important to be on crutches to allow them to heal properly. Some meniscal repairs (suturing back together) do not require crutches, but radial tear and root tear repairs do.
Good Luck
Brian Park
I have a friend who has a medial meniscal root tear posteriorly, in his right knee. We are in the Boston area. Do you know of any orthopedists who are versed with meniscal root repairs? Would it be advisable to look at New England Baptist Hospital or MGH? Otherwise, his primary orthopedist is considering a unicondylar knee replacement procedure.
Most root tears occur in the presence of a degenerative or arthritic knee. Often times the severe pain that occurs at the time of the tear settles down over the next 8-12 weeks. Most of these medial root tears do not need to be fixed because of the co-existing osteoarthritis.
jeff pine
Hello Dr Luks,
Last November I underwent a root repair after I tore my medial meniscus playing basketball. I am 60 years old and before my injury was running twice a week, playing basketball twice a week, and playing tennis once a week, and was injury free. Last month I had an MRI because in the months since the surgery I have not been able to run without a limp and I have experienced pain (only when running), and some instability in the knee. The MRI disclosed a cartilage lesion and a “failed root repair”. Apparently I do not have any type of significant arthritis in my knee. I’m wondering if I would be a candidate for a partial knee replacement to solve these two problems? Thank you.
So… the cartilage lesion might be an arthritic lesion (it commonly is). Many medial root repairs performed in the presence of any degenerative changes will fail. A partial knee replacement is an option for those with significant daily pain with walking, etc. It should NOT be considered a viable alternative if your desire it to return to running and basketball. That’s a lot of force on that small prosthesis.
Amir
Hi Dr. Luks,
Thanks for your recent post about “Root Tears of Medial Meniscus.”
My mother is 55 years old, she has pain in her right knee. MRI report and conclusion says
Mild joint effusion is seen.
ACL sprain at proximal portion is seen but PCL appear normal in shape and signal intensity.
Root tearing of posterior horn of medial meniscus seen but lateral meniscus appear normal.
MCL sprain grade 1 is seen but LCL appear normal in shape and signal intensity.
Bone bruising in medial aspect of tibial plateau is seen.
Should she go for surgery or not? Please advise what to do?
Thank you very much
Surgery is not usually recommended for root tears in the presence of arthritic changes. Let the pain from the bone bruise subside (stress reaction from the tear) — that’s usually what hurts most and it may take a few months.
Andrea Huntey
Hello Dr. Luks,
I just turned 60 and have been diagnosed with subacute minimally depressed medial tibial plateau subchondral fracture, and a partial thickness tear at root of posterior horn of the medial meniscus and have severe chondromalacia in the patellofemoral and medial compartments.
I am a travel agent and walk all the time in Europe (uneven streets) and the U.S .as part of my job
My Dr. tried a cortisone shot before my last trip and it did nothing. She says I do not need surgery. I now walk with a partial limp. She gave me a prescription for Naproxen.
I have been strength training for over 20 years and love to walk. Am I doomed to limp in pain? I love to be active and am afraid walking will increase my injuries. My Dr. said I can try some type of Cocks Comb injections (3 of them) but doesn’t think they will help. I have Kaiser as a health provider and am not sure if I need to go outside my network. (I live in Atlanta) Any advise is greatly appreciated. Andrea
The subchondral (stress) fracture is what’s bothering you. Injections won’t help that. Operating on that type of meniscus tear in this setting would be a mistake. You need to take the pressure off your leg until the edema (inflammation) from the fracture subsides…. This combination of issues – Root tear, stress fracture and arthritis are very common and many people will recover to a reasonable and functional level of activity within a few months. Like and “fracture” it takes time to heal.
Coleen
Thank you for your reply. It is a difficult decision especially with a wedding coming up. As a side note and another consideration is that I have hereditary hemachromatosis which can produce crystals within the joint and cause damage. Dr. said that he would be able to see if there is any of this during surgery. I’m thinking that I should go ahead with it and let he get a better look inside joint to rule out any other issues plus it hopefully will help and I won’t have any instability issues and it will be healed before wedding. With my luck, if I don’t have it, my knee will probably buckle the day before or day of wedding. One final question…Is there blood supply in the root so that it can regenerate? I read that there are parts of the meniscus with blood supply thus they can heal? Sorry…that’s actual 2 questions. Thank you again.
Coleen
Hello Dr. Luks from Naples, FL. orginally from Boston, MA. Been in Naples 3 years. I am 52 y.o. active female. Previously (2004) bi-lateral compartment release all 4 sections of calf muscles from Chronic Compartment Syndrome. 2 previously meniscus surgery on both knees (2007-2009). A month ago my left knee swelled, became painful aching, unable to bear weight going up and down stairs. However, since then my knee has become stable again but it still does swell and I have swelling above knee cap. Also, after walking on it for a couple of hours it begins to hurt. I have found an orthopedic sports med doctor, Dr. Guerra, who is supposed to be the best and does some of the sports teams in area. I didn’t asked about how many horn roots he has repaired however. His recommendation is a partial medial meniscectomy. He believes that the horn root is intact at one end of the root with some detachment and tear on the other side. He said that he does not want to touch the lateral meniscus so to keep as much cartilage as possible on that side. My major concern is the root tear which he said doesn’t have a good prognosis if it is a complete tear. I believe that he is going to try to shave any detached edges of the root and leave it. I just don’t want it to tear completely and then have to have an additional more drastic surgery in the future. Is there anything that can be done now to stabilize the root to reduce this possibility? What would you recommend under these circumstances? Thank you so much. Any suggestions will be helpful. Side note….My daughter is getting married in Jamaica on November 11th. Dr. Guerra and his PA were great about scheduling me in as soon as possible so it can heal as much as possible before wedding.
MRI results shows….
CONCLUSION:
1. Partial medial meniscectomy. Recurrent tearing involving the body and posterior horn root is suspected with fragmentation and maceration of the root and inferomedial displaced flap noted long the undersurface of the body. Regions of a least intermediate grade chondromalacia involve the posterior weight bearing and posterolateral weight bearing medial femoral condyle and less so medial tibia.
2. Horizontal trizonal cleavage flap tear extends from the anterior horn to the posterior horn of the lateral meniscus with subtle free edge and inferior articular surface communication suspected at the anterior horn-body junction.
3. Thickened MCL for which chronic sprain is favored. Dissectiong Baker’s cyst and semimembranosus bursitis are contributory.
4. At least intermediate grade to high grade patellorfemoral chondromalacis.
DETAILS:
Medial Meniscus posterior horn and body is small for which meniscectomy change is favored. Remnant tearing involves posterior horn root and less so posterior horn and body. Horizontal trizonal cleavage flap tear involves lateral meniscal body. This tear measures 3-4 cm in length and extends from the anterior horn to the posterior horn. Subtle inferior articular free edge communication is suspected at the anterior horn-body junction. Clinical correlation will be necessary to determine the significance of this finding.
Chrondral thinning and irregularity involves the posterolateral weight bearing medial femoral condyle and less medial tibia. Posterior horn root of medial meniscus is fraying and irregular. Subtle inferior displaced flap along the undersurface of the medial meniscal body is demonstrated. Regions of recurrent tearing within the meniscus are suspected.
Most medial meniscal root tears are degenerative — as such most are best treated non-operatively. If non-operative care doesn’t result in relief and arthroscopy can be considered, but the results are mixed… meaning that it might work for some (especially those with loose flaps), yet it might not work to alleviate pain/swelling. Difficult decision making.
Julie Vander Linde
Doctor I thank you for your research and comments. I have a MRT to the posterior horn. I am 53, play competitive tennis and do boot camp multiple days a week. In January I felt some irritating tweetkng in the knee. I continued my activity until March when I was slipping my shoes off and I collapsed, the knee filled with blood. Following draining the blood and a cortezone shot I was doing really well. Now 5 months later I believe the cortezone shot is wearing off and I have swelling of the knee and discomfort streightening it. I have not been able to run and if I do any high impact stuff I really swell and am in pain to even walk. I am considering PRP or other injectables. What do you think? I am leary about surgery because after the tear I was on crutches favoring my left leg for about 6 days while I waited for the cortezone to start to work and I felt my other knee degenerating. Also do you know any experts in the Chicago area?
Brian Cole at Rush
Linda
My recent MRI report of my knee indicated that I have a radial tear present within the medial meniscus involving the posterior horn at the root insertion along with meniscal extrusion, accompanying high-grade chondral loss throughout the medial compartment with moderate medial side osteoarthritis. Chondromalacia with high-grade chondral loss within the patellofemoral compartment with moderate osteoarthritis. I understand that they do no want to do repair surgery because of the extensive arthritis present. I currently suffer with great pain and locking posteriorly to the point at times where I cannot bend the knee and medial knee pain. Would arthroscopic removal of some of the meniscus minimize some of the pain? The surgeon initially indicated that the only way to fix it would be to receive a knee replacement due to the extreme arthritis. I do understand that a replacement may be needed in the end, but would a partial removal of the meniscus be beneficial? Any input would be greatly appreciated. Thanks.
Very hard to answer that without seeing you. In this situation one of three possibilities. The surgery might improve your pain, it might not change a thing… and it also stands a chance t making your symptoms worse.
Arnold
I am a 73 year old workaholic that is not overwieght. I knelt on one knee and when I came up that knee, left knee, popped. I could barely get back into the house due to the pain. After doctor visit and MRI, the doctor called and said that I have an “amputated meniscus tear-severe and torn cartilege”. I was told that surgery is needed. I know there is some new gel that can be injected into the knee. Do you think I MUST have surgery or will the gel work ?
Sounds like a root tear… common, and usually associated with a degenerative knee. Meaning that you usually have osteoarthritis in addition to the root tear. “must” is simply a word that shouldn’t surface often when talking about meniscus tears. These are usually quality of life decisions. As I mention … most studies show that people with arthritis and root tears tend to do OK without surgery.
Judi Mottle
Dr Luks,
I’ve been doing much research since reading my MRI results and see that you are by far the most expert in my condition.
The MRI states “complete degenerative radial tear at the posterior root attachment of the medial meniscus with partial peripheral extrusion of the medial meniscal body”.
I am 69 years old and are fit (workout 6 X wk). In your opinion is surgery the option for my condition?
Do you know any expert (as you) in this type of surgical technique in the Bergen County NJ vicinity?
Thank You
I do not know of any Judi …
some of these root tears should be repaired, others shouldn’t. Your X-ray, MRi, exam and complaints help us make that determination.
Annie Gunn
Your direction would be greatly appreciated:
MRI – Demonstrates full-thickness tear of the posterior root inserction of the medical meniscus with mild peripheral extrusion of the meniscus posteror horn.
Fraying and blunting of the free edge of the lateral menisus body with no evidence of tear.
Grade 3 patellofemoral chrondromalacia
Grade 2 chondrosis in the medial and lateral tibiofemoral compartments.
Doreen king
I currently have a root tear and my doctor has done 2 under the supervision of his mentor. How do I find someone in CT who has done many since it is such an unusual injury?
unfortunately you need to ask the surgeons about their experience.
michelle
Hi Dr. Luks,
I’m a 61 year old female (5’2 and 127lbs). My knee had been hurting on and off for 4 mos after some dancing. Then one day I ran up the stairs and felt a pop in back of knee and couldn’t put any weight on it. Was on crutches for a few days, then a cane. Now, I can walk with very little, and often no pain, sometimes with a cane for extra support. MRI shows medial meniscal posterior root tear, with full thickness avulsion with a gap of 6mm. Moderate medial extrusion of the meniscal body. Mild chondral thinning and fibrillation of the medial compartment cartilage. Mild reactive edema posterior medial tibial plateau. Intraosseous ganglion cyst of the posterior to central medial tibial plateau. Said cyst has been there for many years. Can this be managed without surgery? I’m not an athlete, but do like to walk.
Nancy Kornegay
Thank you for the informative web site, Dr.Luks. I was recently diagnosed via MRI with full-thickness tear of the medial meniscus posterior horn root ligament. All ligaments are intact. I am 58 years old, not overweight, and I have always been very active. I live in the Houston area. Do you know of any specialists in this type of injury in my area? I understand this is not a garden-variety injury. I want to determine if I am a candidate for surgical intervention.
Thanks much
Hi Nancy… I do not know anyone in the Houston area. I would start with the academic centers and call their sports medicine departments to see which providers may be able to help you.
Linda subissati
Thank you for your reply Dr Luks, it is much appreciated. Take care.
Linda subissati
Hi Dr Luks, I am a 56 yr old female and I weigh 160 lbs. The results of my MRI indicate the following: 1. Full thickness radial tear at the root of the medial meniscus. 2. Moderate joint effusion with minimal synovitis. 3. Moderate patella femoral and medial tibia femoral compartment chondropathy. 4. Mild lateral tibiofemoral compartment chondropathy. Should I have surgery or not? Please give me your advice. Thank you very much.
The research would say to tread lightly with these tears since the arthritis is likely to be more of an issue for you.
Viselly
Dr. Luks, Thank you for reply. Can you please let me know non-surgical option. Thank you.
Viselly
Hi Dr. Luks, I am 45 years old and 252lb. My knee started hurting after normal walk. I just got my MRI report and conclusion says that (1) Complete radial tear through the posterior attachment of the medial meniscus with mild extrusion of the body (amputated meniscal root). (2) Large joint effusion with synovitis. (3) Early degenerative changes are most pronounced in the medial compartment. Should i go for surgery or not? Please advise what to do? Thank you.
These cases are usually managed non-surgically because of the arthritis
Theresa trimilove
Does a complete tear of the posterior meniscus with flap require surgery?
Flap tears which are causing “mechanical” symptoms — popping, catching, locking, severe sharp pain might go on to require an arthroscopy. Not always, but more often when compared to degenerative tears.
Ernie O.
Hi Dr. Luks,
Thanks for your recent post about “Root Tears of Medial Meniscus.”
My wife was just diagnosed this morning after getting her MRI on Monday. Last Friday she had an x-ray which obviously showed no breaks or anything else.
At 54, my bride LOVES to run. She does not run fast or for that long. She runs a 5K about 2-4 times a week and has done two half marathons. She just started running about three years ago since a bad shoulder hindered her weight lifting.
This rehab/surgery/etc.really needs to go well since she this is all she has left.
Do you know anybody who lives close to Rochester, NY that you recommend?
Thanks so much for your time,
Ernie O.
HI Ernie …
I’m sorry… I do not know of anyone in the Rochester region.
best of luck to your wife!
Catherine
Thank you so much for your reply. That is correct – the MRI shows nothing else wrong with the knee and no osteoarthritis. Are you experienced in this surgery? My orthopedic surgeon has only done it twice. So far I haven’t found anyone else here who has performed it. Could you possibly recommend a surgeon in Memphis?
Catherine
Dr. Luks,
I really appreciate your informative site! I am 44 years old. I used to play tennis once a week. Last month I began running about 2 miles a day for the first time in 3 years, in an attempt to get more in shape and lose weight. I have since lost about 15 lbs. with about 25 more to go. After running just a few times, my left knee had some pain. Following my last run, the pain was severe and my knee felt swollen and stiff. Each day afterwards it was better. However a week later, walking was uncomfortable and suddenly I felt excruciating pain in the knee and it seemed to buckle. A few hours later I received a cortisone injection which helped tremendously for about 10 days. Since then, I do feel twinges of pain throughout the day. An MRI showed “posterior horn of medial meniscus radial tear centrally vs. posterior horn meniscal root ligament avulsion”. The MSK radiologist and my orthopedic surgeon are both now leaning toward the interpretation of the root ligament tear. I am devastated by this news as I have never experienced an injury. It is hard to hear that surgery is not a good option. I plan to begin physical therapy immediately. Would you advise pursuing surgery or trying to strengthen my leg through physical therapy? If I do not pursue surgery, would you advise discontinuing tennis? My knee does not feel weak, as if it would buckle. I am so unsure of what to do because I’m hearing a variety of opinions. Thank you so much for any advice you can offer!
Certain root tears might benefit from surgery… especially those where the X-rays and MRI show little or no evidence of osteoarthritis or “joint space narrowing” .
Sheila
How do you know if it is a root tear?
An MRI will show a tear involving the root attachment of the meniscus.
Sheila
I feel your pain. In the same boat. Devastated!