
Root tears of the medial meniscus are being recognized on an MRI with increasing frequency. Most of you who have a root tear do not recall an injury to your knee. That is a degenerative meniscus root tear. A handful of you had a significant sports-related injury or ACL tear and find that you also have a root tear. How we treat these meniscus root tears will depend a lot on your age, how your tear occurred, the location of your root tear, and whether or not anything else is injured.
A root tear of the medial meniscus is a unique tear. Repairing a root tear of the medial meniscus requires a very different approach than a traditional meniscal repair. Root tears that occur after trauma and an ACL tear will require a meniscus root repair. This is in contrast to the more common degenerative root tear. Some degenerative root tears will benefit from a repair, and some may not. We can help guide you through that decision making. This article will discuss what root tears of the meniscus are and the thought process behind how we treat them.
The meniscus is a c-shaped cartilage cushion in the knee joint. It functions as a shock absorber and a stabilizer. Tears of the meniscus are prevalent. Root tears are not very common, but they are increasingly being recognized as a cause of severe arthritis. Your doctor must be well versed in root tears since they behave much differently than a typical meniscus tear.
What is the “Root” of the Meniscus?
The meniscus is attached or anchored to the tibia by two “roots.” There is a root attachment in the front of the meniscus and a root attachment in the back (posterior) of the meniscus. In most injuries, it is the posterior root attachment that is torn. Problems arise with root tears because if the root of the meniscus is torn, then the entire meniscus becomes non-functional. In other words, the meniscus needs to be well anchored to the tibia to function as a shock absorber.
How Did I Tear The Root of the Meniscus?
Many meniscus root tears occur as a result of trauma. Some root tears occur at the same time you tore your ACL. Other common causes of root tears might be a fall, slip on ice, or related to a sports injury. As we age, it is easier to tear the root of the meniscus, especially the medial meniscus root. Therefore you may tear the root by merely kneeling or squatting down. The average age of patients with root tears in my practice is between 25 and 65. The younger patients tend to have lateral root tears in association with ACL tears. The older patients tend to have medial root tears in association with early arthritic changes. Root tears that occur in association or with coexisting osteoarthritis are the most common form of root tear seen by orthopedic surgeons. Most of you will note that you knelt, bent your knee or twisted, felt a pop, and then noted increasingly more severe pain in the knee.
Patients with root tears of the medial meniscus often complain of giving way or instability. They are fearful that the knee will buckle or give-out. The onset of pain is often abrupt, and the pain is usually on the inner side of the knee, or in the back of the knee.
How Do You Fix A Root Tear of the meniscus?
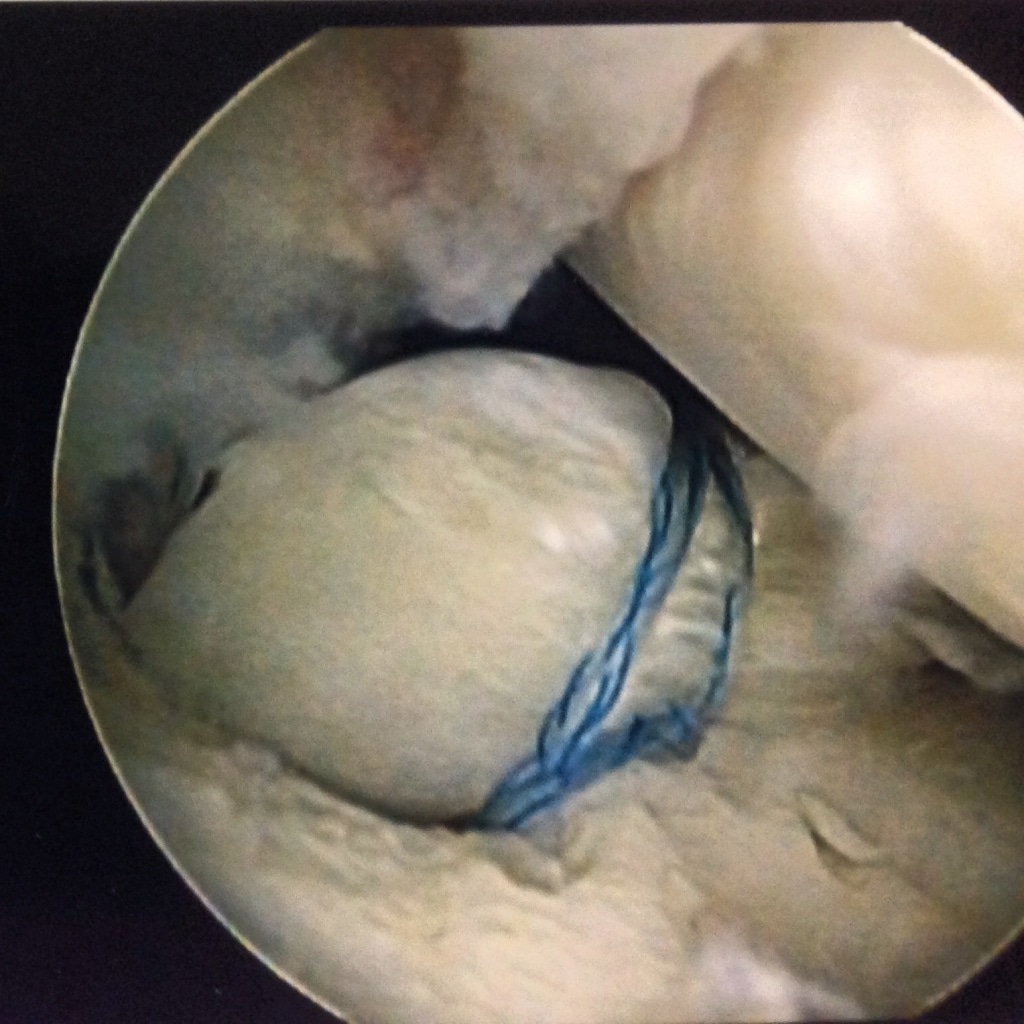 To fix the root of the meniscus, we need to pull the root against the tibia in the same place where the root was before your injury. The procedure is mostly arthroscopic. It is a technically challenging procedure, so please be sure that your physician has performed many of these. After we put a suture around the root of the meniscus, we drill a hole from the front of your tibia into the root area. We then bring the stitches out through the hole and tie them over the front of the tibia. Therefore we are pulling the root down into the tibia, and the stitching will hold it in place until it heals. In the picture above, you can see how the stitch is through the root of the meniscus, and the meniscus is being pulled down into a small hole I created to encourage healing.
To fix the root of the meniscus, we need to pull the root against the tibia in the same place where the root was before your injury. The procedure is mostly arthroscopic. It is a technically challenging procedure, so please be sure that your physician has performed many of these. After we put a suture around the root of the meniscus, we drill a hole from the front of your tibia into the root area. We then bring the stitches out through the hole and tie them over the front of the tibia. Therefore we are pulling the root down into the tibia, and the stitching will hold it in place until it heals. In the picture above, you can see how the stitch is through the root of the meniscus, and the meniscus is being pulled down into a small hole I created to encourage healing.
Do All Meniscus Root Tears Need Surgery?
The body of evidence about the treatment of root tears of the meniscus is growing. There is a generalized agreement that most medial root tears that occur in the setting of moderate or severe osteoarthritis should not be fixed. In these cases, the meniscus is usually degenerative or wearing out. Studies have shown that if these tears are fixed, they will commonly tear again in a very short time frame. If the arthritis is severe, then fixing the root tear may not alleviate your pain.
Root tears that occur in a severely arthritic knee should be treated with relative rest. Some of you may require a walker or crutches for limited weight-bearing. Many will benefit from the use of a compression sleeve, and after a month, a course of physical therapy.
Medial root tears with minimal osteoarthritis should likely be fixed or repaired. A successful repair will eliminate the sense of the knee giving way or feeling unstable. More importantly, fixing a medial meniscus root tear might slow the progression of osteoarthritis. But the critical issue here is that the severity of arthritis in the knee should be mild/moderate.
Root tears and ACL tears often occur together
Meniscus root tears often occur when you tear your ACL. If you have a traumatic root tear due to a severe injury, there is agreement amongst sports surgeons and orthopedic surgeons that these tears should be repaired at the same time that the ligament is reconstructed.
Do root repairs heal well?
Some studies show that a high percentage of these root repairs are successful, and there are studies that show that the success rate might be far lower. Many factors will often determine the success rate. First is whether or not you have anything else wrong with your joint… such as osteoarthritis. Other reasons for failure include lack of biological healing, resuming activities too quickly leading to a new tear, and over-tightening the repair, which could lead to a new tear somewhere else.
Bottom Line:
If you have a root tear as a result of a traumatic injury, be sure you see a Sports Medicine Trained Orthopedic Surgeon with experience repairing meniscus root tears. Some tears might be considered for repair, and others may not. IF you have osteoarthritis, and it is moderately severe, then having surgery for your root tear might not be advisable.
Hopefully, this has improved your understanding of meniscus root tears of the medial meniscus. Here is a review of root tears that might be worth reviewing.











Hello, Dr. Luks.
Is a “meniscocapsular separation” the same thing as a root tear? I’m finding little information online about this condition.
I just turned 40 years of age this August. I am female and live in Texas, with a fairly active lifestyle, or at least…it used to be. On April 19th of this year, I bent awkwardly – think bad form on a lunge – and I heard the dreaded pop/snap and knew/felt something was wrong. I was able to walk for about 72 hours after the incident, but, not thereafter.
My MRI Impressions, dated 05/11/17 read:
1. Meniscocapsular tear of the medial meniscus about the posterior horn.
2. Low-grade strain within the medial head gastrocnemius muscle.
3. Very low-grade cartilage within the lateral facet of the patella.
4. Small knee joint effusion.
5. Enchondroma measuring 5.6 mm within the femoral diaphysis.
Everything else, according to the MRI findings, seems intact, normal or relatively preserved. (Though I confess, there’s a nagging dull ache on the top left of my knee cap – is that related to the lateral facet of the patella in the findings? And a dull ache on the back of my knee, as well. I think I’m also possibly developing a Baker’s Cyst at this point).
Despite the pain lessening, which is good, my injury was almost six months ago, and I’m still not recovered. I’ve used mostly crutches in this period of time. Indeed, it took a while for my leg to be able to extend fully/have my foot touch the floor. I saw two separate orthopedists who both opted for conservative treatment. I have done physical therapy which got me back to full flexion. My pain has decreased. I am now able to stand, but I still present with quite a limp when I walk. So, my distances are short. I still cannot climb stairs without assistance and I can still feel that the …inner-mechanics of my knee, if you will…. are “off”. My ortho doctor told me he’ll see me again in November and maybe we’ll see “if surgery is worth the risk”.
I’m quite frustrated if not a bit scared.
Dr. Luks, is a “meniscocapsular separation” the same thing as a “root tear”? And would you advise surgical repair on this or shall I keep going the conservative route and see how I keep progressing? My quality of life has definitely been impinged. I just don’t know if this will ‘heal’ on its own or if I should try surgery to restore the function and kinematics of my knee joint. Also…what’s the proverbial shelf-life of my MRI? I wonder if a new one was taken today, it would show different results.
I truly hope to hear from you.
Thank you in advance for your time and your informative website.
Sincerely,
-Suzanne
So, a menisco-capsular (you might also read about RAMP lesions) separation is not a root tear. An M-C separation is a very peripheral tear of the meniscus. They are rare in 40 somethings… usually adolescents have these. Assuming the radiology read is accurate these are usually very repairable tears. Did your doc agree with the radiologist? I would gather a few opinions on the type of tear… either way, both MC-separations and root tears, in a young active person without arthritic changes are generally amenable to repair.
Good luck
Thank you so much for your reply, Dr. Luks!!
I feel honored….
I am not acquainted with RAMP lesions so…. onward goes my personal research! I had the feeling my injury was a rare case. (My age and my not presenting with any ligament tears being the chief reasons).
My doctor, whom I seem to be visiting every other month or so since April, did agree with the radiologist, at least, with regards to the M-C separation. But, beyond suggesting conservative therapy, nothing else has been mentioned except: “When you return, we’ll decide if surgery is worth the risk”. [guLp]. Sounds….ominous.
I don’t know if six-months is an expected time frame to still be dealing with all of this?… It’s the not being able to walk very well; tenderness/a lump behind my knee; and the slight tenderness at the soft area to the left of my left kneecap that are still lingering. (Obviously, it’s the lack of functionality that I have that’s driving me crazy). I’m very afraid of surgery creating other problems; but, with your reply and my lack of wanting to stay where I’m at, I will move forward.
Many thanks again, Dr. Luks. I wish I could see/thank you in person.
Cheers,
-Suzanne
Dr. Luks,
I am a very physically active 57 year old female. I was diagnosed with breast cancer in May 2016 and have undergone chemotherapy, radiation and a lumpectomy in 2016. I have been going through Herceptin Infusions since January 2017. I have developed Osteopenia. I have continued to exercise in whatever form possible throughout my treatment. I had a small right knee meniscus tear that I had repaired in March 2016. In September of this year I felt a pop while walking into a grocery store. I have been diagnosed with a left knee medial meniscus root avulsion with surgery scheduled in 2 weeks. My surgeon wants to do an aspirin regimen for 2 weeks post surgery and my oncologist wants me to take a blood thinner due to a previous DVT during my chemotherapy. Any suggestions?
Thanks,
Sheryl
You need to discuss this at length with your surgeon. I can not comment on this. A prior DVT increases the risk of a future DVT.
Dr. Luks, what do you think about partial (not complete) chronic/degenrative root tears of the posterior lateral meniscus in younger patients who don’t have any signs of arthritic changes in the knee? A few surgeons have told me that partial root tears cannot be repaired (only complete root tears can be), and that a patient’s options would either be partial meniscectomy or leaving it alone. In general, do you know if this is true, or is it possible to repair a partially-torn posterior lateral meniscus root?
Thanks
Most all of the literature in this area is written about complete root tears. There are no scientific studies on the management of partial root injuries. If it is a partial tear, it might not be the source of your knee pain?
Dr. Luks,
Thanks for the info; that’s what I figured (in terms of there being no studies that have been conducted on the treatment of partial root tears). The partial root tear actually occurred almost 3 years ago. I probably tore it from running every day. It seems like it has “healed” to the point that the only noticeable symptom is snapping when I twist my foot into the ground (thus twisting the knee as well), along with a loud pop that sometimes occurs when I repeatedly flex and extend the knee (the pop usually occurs just before the knee is fully extended). It doesn’t really hurt, but it does feel like an “adjustment,” almost like popping your knuckles.
I still run 4 days/week (7-9 miles each time). I usually don’t feel any pain at all during the runs, but there may or may not be mild pain (almost like an icy-hot around knee but nothing sharp) feeling later that day. During some weeks, I will be able to do my runs and not experience any pain afterwards, and I will start to think that it is healed. During other weeks, the pain is more noticeable but never severe. It seems to be more likely to get sore afterwards if I ran hills or uneven surfaces. Also, it’s hard to explain, but it sometimes feels more like something small is tugging/pulling at the back of knee, rather than actual pain.
In fact, I would say the pain itself is easily tolerable. I am just afraid of tearing the root even further (a radiologist said he would estimate that the tear was a pretty small portion of the root) or of developing arthritis if I keep running.
The surgeons I have talked to seem to think it is an unusual root tear case (Dr. LaPrade took a look at my x-rays, and his PA told me that it wasn’t a textbook root tear and there was no extrusion). The radiology report also said there was no arthritis and no other issues. It makes me wonder how I got the injury in the first place (never had any other meniscus tears, all ligaments are fine).
Do you think it is a bad idea to keep running without getting surgery? I am 29 and would like to continue to be able to run 4 days/week, so if surgery would be the best alternative to pursue for long-term success, I’ll definitely consider it. So far, one surgeon wanted to do partial meniscectomy immediately then recommended a wait-and-see approach when he looked at a follow-up x-ray a few months later and said it looked “a little better.” Another surgeon said he wouldn’t recommend surgery since the tear is small, unless it gets to the point where it bothers me on a severe level. Of course, even though the pain is mild enough to push through it, I just don’t want to make things worse.
What a wealth of info you have relayed. I thank you for that. I had medial meniscus root repair January 31st. I am 68 years old, very active with, according to my orthopedic surgeon, no arthritis. I was non weight hearing for 6 weeks following surgery and have been going to my twice a week. My concern is the pain and swelling behind my knee and on the medial side of my knee. Am I hoping for too much too soon? How long is normal recovery for a root repair? Thanks for your response.
These recoveries are always longer than we expect…. some swelling is normal. Some pain behind the knee might be normal too. My root repairs take 3-4 months minimum to feel that they are happy after the surgery and are able to return to some sports and activities of daily living. Intense running sports, tennis, etc I usually delay a return to until nearly 6 months after surgery to minimize the risk of reinjury.
Thank you Dr. Luks for all this information. I’m 67, overweight and losing, working out slowing and increasing to become more fit. Lots of quad work and some squats. Had some pain in right knee but assumed osteoarthritis. Kept going with stairs and bike and elliptical. On Easter, popped my knee going upstairs. Can’t put weight on it. MRI: Findings suggestive of a meniscal tear at the root attachment of the posterior horn medial meniscus. Mild medial subluxation of the body of the medial meniscus, and mild free edge fraying of the body medial meniscus. Free edge tear involving the body of the lateral meniscus. Complex meniscal tear involving the anterior aspect of the posterior horn lateral meniscus near its root attachment. Scoping scheduled in a week with surgeon who recently scoped other knee. Options?
A scope may or may not be a good idea… Hopefully, your surgeon plans on actually repairing (suturing) the root!
Sorry Dr. Luks. I thought ‘scope’ was short for arthroscopic repair and not just look. He plans to probably repair the meniscus and remove all the feathers. Thank you for your response.