
Severe pain on the inner or medial side of the knee can be disabling. Many people with terrible pain on the inner or medial side of the knee do not recall any injury. There’s often a similar story or history given by our patients with regard to the onset of severe knee pain.
One day you felt a click or pop in your knee. A few days later you can barely walk. You are usually between 45 and 75 years of age. After kneeling, or squatting to pick something up, you felt a pop inside your knee. You have some pain in the knee, but immediately after the pop, it wasn’t terrible pain. The next day the pain is worse, and the strain on the inner part of your knee continues to worsen to the point that you can not walk. Now your knee starts to swell. Why has the pain on the inside of your knee further exacerbated over the last few days?
Although not described as a terrible triad in the scientific literature, over my 20 years of experience I have heard this story often enough to know what the list of diagnoses will be in this situation. After speaking with you for a few minutes and a brief exam, the diagnosis is often clear. The triad of issues that arise in this situation is a common cause of severe medial knee pain or pain on the inner side of your knee in people between 45-75 years of age.
Your knee MRI will often show a:
- Root tear (Radial tear) of the medial meniscus
- mild or moderate knee arthritis
- bone marrow edema, or an insufficiency fracture in the inner part of the knee.
Those three findings on your MRI are related to one another… in other words, these 3 findings are associated with one another. These three findings are what I refer to as the Terrible Triad of (medial) knee pain. It is an under-recognized set of issues and it is often poorly understood by patients I see for second opinions.
The Terrible Triad: Part I – Meniscus Root Tear
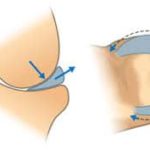 The meniscus plays a crucial role as a cushion inside the knee. It distributes the stresses of walking very efficiently. The root is where the meniscus attaches or is anchored to the bone. The meniscal root attachment degenerates (or wears out) in our knee just like many other tissues in our body. That’s why it will pop and tear while only squatting down or twisting while walking. The trauma or energy needed to tear the root of the medial meniscus in an adult is small. That was the straw that broke the camel’s back. This post goes into more detail about root tears of the medial meniscus. These root tears initiate the process that will then cause the other two components of this terrible triad to worsen.
The meniscus plays a crucial role as a cushion inside the knee. It distributes the stresses of walking very efficiently. The root is where the meniscus attaches or is anchored to the bone. The meniscal root attachment degenerates (or wears out) in our knee just like many other tissues in our body. That’s why it will pop and tear while only squatting down or twisting while walking. The trauma or energy needed to tear the root of the medial meniscus in an adult is small. That was the straw that broke the camel’s back. This post goes into more detail about root tears of the medial meniscus. These root tears initiate the process that will then cause the other two components of this terrible triad to worsen.
The Terrible Triad: Part II- Osteoarthritis of the knee
 The degeneration of the meniscus root causes it to “tear.” When the tear occurs, the function of the meniscus is lost. That loss of cushioning function causes an increase in stress on the bone. The meniscus usually distributes the force of weight-bearing evenly across our knee joint surface. If the root tears and the function of the meniscus are lost, then the force of weight-bearing will concentrate is small areas on the joint surface. That will overstress the cartilage and lead to arthritis. In the terrible triad, many of you will also have at least mild osteoarthritis. Osteoarthritis of the knee implies that you have lost some of the articular cartilage which covers the ends of the bones in the knee. That cartilage also cushions the knee.
The degeneration of the meniscus root causes it to “tear.” When the tear occurs, the function of the meniscus is lost. That loss of cushioning function causes an increase in stress on the bone. The meniscus usually distributes the force of weight-bearing evenly across our knee joint surface. If the root tears and the function of the meniscus are lost, then the force of weight-bearing will concentrate is small areas on the joint surface. That will overstress the cartilage and lead to arthritis. In the terrible triad, many of you will also have at least mild osteoarthritis. Osteoarthritis of the knee implies that you have lost some of the articular cartilage which covers the ends of the bones in the knee. That cartilage also cushions the knee.
The Terrible Triad: Part III- Insufficiency fracture
It follows that if you tear the root of the meniscus the stress in the knee increases. You already have arthritis, so the cartilage cushion was thin and less protective. All of this causes an increase in the pressure within the bones in the knee. In many of you that will lead to a stress fracture or an insufficiency fracture. Those insufficiency fractures of the knee cause a ton of inflammation which shows up on an MRI as bone marrow edema. It takes at least 1-3 days or more for the stress fracture to occur following a root tear. That’s why the pain worsens over the next few days after you felt the pop.
The bone marrow edema caused by the insufficiency fracture causes severe pain. The meniscus is not the most likely cause of pain in this situation. Bone is a confined space, and it can not expand. If you have inflammation and swelling in the bone, then the pressure in the bone will increase. That’s why an infected tooth hurts so much, that infection is in a tight space, so the pressure rises, and it is the pressure that hurts so much.
The terrible triad hurts a lot. That usually leads to a visit to your doctor or an Orthopedic Surgeon. An MRI reveals the findings I mentioned earlier.
Treatment of The Terrible Triad of Medial Knee Pain
Most of you who have all three of the findings I mentioned above will usually have very severe pain. For some of you, your Doctor will focus only on the meniscus and recommend surgery to remove the torn meniscus.
That is not recommended as the best way to proceed if you have a degenerative root tear in the presence of osteoarthritis and bone marrow edema. If your doctor recommends surgery to “clean out” the knee, the research shows that the operation often fails to alleviate your pain, and increases your risk of needing a knee replacement.
Why does your knee hurt so much! It is often the bone marrow edema or inflammation in the bone from the stress reaction or insufficiency fracture which is causing your pain. Usually, time and limiting weight-bearing can improve that pain. It may take 1-3 months for the pain to subside. A subchondroplasty for bone marrow edema may help some people feel better. Determining who might benefit is often a challenge. And infections or complications from a subchondroplasty can be hard to manage.
Meniscus root repairs for severe medial knee pain
In a knee with mild arthritis and persistent pain due to a root tear of the medial meniscus, a repair of the meniscus root should be considered. Make sure that your Orthopedic Surgeon knows how to perform meniscus root repairs. They are not easy to perform, and some surgeons only remove these torn pieces. During a root repair, the meniscus is sutured back to its attachment in the bone.

Focusing on meniscus preservation and restoration of more normal force distribution will offer you the best chance of long term success. If the arthritis is moderate to severe and your pain persists despite rest and limited weight-bearing, then a knee replacement might prove to be your better option.
The bottom line is that treatment recommendations need to be individualized to improve your chance of success and minimize the risk of worsening arthritis or the risk of having unnecessary surgery.










This was so helpful, my knee pain is so severe. Your symptom checker convinced me to see my Dr., I have OA. & Had spinal, & cervical fusions. Metal plates & screws.
I’m glad that you found it helpful
I do not want a knee replacement yet!! I’m too young., I’m 59yrs.
Completely understood !
Thanks for your posts, I’m hoping they can shed light on my increasingly hopeless knee and/or hip injury…
How bad are stairs in a home with these knee conditions (age 68)? I am thinking of buying a stair lift, as advertised on tv, to ride up the stairs. I am concerned that the moderate osteoarthritis and meniscus tear will be exacerbated by the stairs. Thanks!!
Without examining someone or assessing their abilities I can not tell you if that purchase is worthwhile or not.
Good Morning Dr. Luks,
Thanks for your excellent articles. Surgeon wants to do surgery to repair/remove partial meniscus. Previous meniscus repair in USMC. Pain has worsened over past 6 months. Biggest complaint is sleeping or lack thereof. From reading your articles my concern is the marrow edema. Any recommendations? Do you recommend a second opinion? X-Ray shows moderate osteoarthritis, MRI comments below. About 25-30 pounds overweight. Thank You.
Findings: Osteophyte formation and cartilage loss are identified in
the medial compartment. There are several large defects in the
articular cartilage of the medial femoral condyle with marrow edema in
the medial tibial plateau. Abnormal signal within the posterior horn
of the medial meniscus extends to the inferior articular surface on
series 3 images 9-10. It also extends into the meniscal body. The
lateral meniscus is unremarkable.
Definitely seek a second opinion… you have a highly degenerative knee. A straightforward arthroscopy is not usually successful in the long term in these instances.
It would depend on your exam … but you might be correct. Bone marrow edema is often the cause of pain, and an arthroscopy will not address that since it is due to the arthritic changes.
Good Luck