
You have fallen, you can not move your arm, and you have been told that you have a rotator cuff tear. Do you need to consider surgery to repair your rotator cuff?
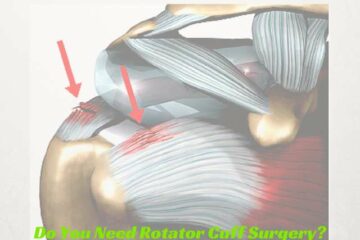
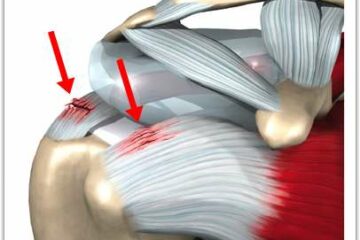
Types of Rotator Cuff Tears
In our first Expert Series post we explored the cause of rotator cuff tears. What explained that the majority of rotator cuff tears are due to degeneration or attrition of the rotator cuff. Simply put- your rotator cuff tendon simply wore out.
Alternatively, trauma, such as a fall, or an accident can also cause a rotator cuff tear. When it comes to managing patients with traumatic rotator cuff tears most Orthopedic Shoulder surgeons are in agreement. There is a significant difference in the management of acute traumatic tears of the rotator cuff, versus the more common degenerative or attritional tear that we see. As discussed in our last Expert Series post, the initial treatment of a small degenerative tear is nearly always non-surgical.
Do We Recommend Surgery for Traumatic Rotator Cuff Tears?
In this post, our experts will discuss their thoughts on the management of traumatic rotator cuff tears.
Marty Leland, MD: Website, Twitter, Facebook
This depends on the activity level of the patient, how much pain and weakness they have, how long has it been since the tear and if they are starting to see any improvement or are things staying the same or getting worse. Night pain is also a sign that a patient has a higher likelihood of needing surgery. Also, the larger and more retracted the tear, the more I worry that they will not get better unless they have surgery. If I have a patient in their early 40s that works in heavy labor with a traumatic rotator cuff tear that has not shown any signs of improvement in 4 weeks, I might get an MRI right away and then discuss arthroscopic surgery. However, if I have a 70 year old retired patient of low physical activity that tore their rotator cuff slipping on the ice, I definitely want to try a significant course of non-operative treatment before discussing surgery.
Jeffery Berg, MD: Website, Twitter
I always try to fit the treatment to the patient…not the patient to the treatment, so I don’t have absolute rules. If the patient is younger than 65 yo healthy and active, I will almost always recommend surgery. If they are older and active, I will also usually recommend surgery. In patients that are less healthy, older and/or less active, I will consider nonoperative treatment but counsel them that their symptoms are likely to persist, progress or, even if improved over the short-term, could recur in the future. At that time, the tear may not be repairable or if repairable, will likely have a poorer prognosis for healing.
Scott Slattery, MD: Website, Twitter
When an acute, traumatic rotator cuff tear occurs and creates a sudden loss of function, I generally recommend surgical treatment. Patients do not tolerate sudden, significant tears as well as the slow, progressive degenerative tears. Several studies have shown that the best results, with acute tears, occur if the tendon is repaired within three months of the injury.
Derek Ochiai, MD: Website, Twitter
For acute, traumatic rotator cuff tears, I would recommend surgery. Typically, these tears can be more extensive and retracted away from the bone, making non-surgical intervention less likely to be successful. Also, acute traumatic rotator cuff tears in patients over the age of 40 years old can occur in combination with shoulder dislocations. If a patient over 40 has shoulder pain following a shoulder dislocation, I would have a high index of suspicion for a rotator cuff tear.
If you are a healthy, active individual who has slipped, fallen or have been in an accident and you have suffered a traumatic tear of your rotator cuff then your surgeon is likely to recommend a repair to give you the best chance at having a pain free, strong shoulder.
Once again I would like to thank our experts for their contribution to your education on the management of rotator cuff tears and shoulder pain.








Very informative article, but I still have some questions, please. I am a retired Army general surgeon, surgical oncologist, and some orthopedic experience in residency and as a missionary surgeon, buy my knowledge is superficial.
Some 47 years ago when doing a lot of swimming,(Australian crawl), I first developed right bicipital tendonitis. It was temporarily relieved by injections of a depot cortisone and local anesthetic. Over the next 40 years on several occasions I persuaded a colleague or I self-injected. Finally about seven years ago a highly respected Houston orthopedic surgeon did a rotator cuff repair with only partial success in that an osteophyte remains and with abduction and external rotation I feel the tendon snap over the osteophyte.
Tussling with cattle and a feed bucket some two weeks ago there was a forced abduction/external rotation after which I developed severe shoulder pain, inability to abduct arm more than 15 degrees, tolerable passive abduction, and only worsening. Next week I will have an MRI.
1. How is it as I have been told that a strain of the long head of the biceps is a part of a rotator cuff injury?
2. How important if at all is it that the osteophyte I still see on xray be removed as a part of the rotator cuff repair?
3. As a fit 75 year old who still wants to be active on our hobby farm and accustomed to several hours
of heavy work daily, is a 2nd repair a consideration? The joint space is reduced from a normal of 10 mm to only 8 mm, suggesting degenerated soft tissue.
I thank you in advance for your advice.
Hi Dr. Tolls…
In response to your questions …
1. How is it as I have been told that a strain of the long head of the biceps is a part of a rotator cuff injury?
The biceps runs from the arm up through the rotator cuff in a region we call the rotator interval. When people develop degenerative rotator cuff disease — or tendinosis — the biceps, due to it’s close proximity to the rotator cuff is often involved. Experienced shoulder surgeons understand this and often times can alleviate significant residual rotator cuff pain with a biceps tenotomy or tenosdesis.
2. How important if at all is it that the osteophyte I still see on xray be removed as a part of the rotator cuff repair?
The concept that bone spurs cause rotator cuff disease was actually never a peer reviewed concept. It caught on in the 70’s. Was disproven throughout the 90’s and well into the early 2000’s. The bone spur is not the cause of your pain … nor the cause of rotator cuff disease. Tendinopathies exist throughout our body … the achilles, tennis elbow, the patella tendon in a jumpers knee etc. So why should tendinopathy in the shoulder be thought of differently :-) Anyway… I have a few posts in the blog section near the top on rotator cuff tendinosis you may want to read.
3. As a fit 75 year old who still wants to be active on our hobby farm and accustomed to several hours
of heavy work daily, is a 2nd repair a consideration? The joint space is reduced from a normal of 10 mm to only 8 mm, suggesting degenerated soft tissue.
Particularly for someone with a cuff that is degenerating… the article on the treatment of rotator cuff tendinosis might appeal to you. The distance between the acromion and humeral head is not static. If the shoulder girdle is tired from exercise, activity or injury — and the rotator cuff is weak, the distance will decrease. If we exercise athletes with normal rotator cuffs their distance will narrow transiently as well.
I hope this clarifies some of your questions !
Thank you for your service ! :-)
Howard Luks
I am a reasonably fit 70 year old female. 18 months ago I had an accident and presented with painful shoulder when I reached in front on myself. I had some trouble sleeping at night. After MRI it was found that I had near full-thickness tear of the suprasinatous with delamination noted.
Partial tear of the subcoracoid tendon.
Moderate subcoracoid bursal effusion present. Normal inferior glenohumeral ligament complex. Biceps pully is intact.
This has been a long process and I finally have a date for May for repair. The problem is my pain level is now almost nil and I have almost full ROM . No pain at night now. I have spoken with friends of mine who are GPs and they have advised me not to go ahead as they feel I don’t need the surgery and could be more disabled afterwards. What do you think, and what should I say to my surgeon, he is a very respected sugeon and I don’t want to upset him.
Don’t worry about our feelings :-) We have tough skin.
Hi Dr Luks,
I am a 55 y/o woman working as a caregiver. My job requires a lot of heavy lifting. I had an on the job injury of my shoulder Jan 2015, had an MRI on July and seen by doctor in August. MRI results are High grade partial tear and tendinopathy of supraspinatus wit bursal side fraying as well. Insertional tendinopathy of infraspinatus and tendinopathy of subscapularis tendon. Also type II SLAP tear.
I had cortisone shots, PT and manipulation under anesthesia. I still have pain and I am going under surgery in two weeks.
My questions are:
Should I go ahead with surgery? Will surgery be effective for me to recover? Will my shoulder be fine after surgery? Please, give some advise, since I am still not sure if I should have surgery.
Thank you in advance for your words.
I can’t offer treatment advice since I haven’t examined you. Sorry. But second or even third opinions are often worthwhile.
Dr Luks. I am a 75 year old woman, not very active and live alone. Several months ago i tore bith rotator cuffs. My orthpod did not feel that i was a. good candidate for surgery Due two other health conditions . for safety purposes my son-in-law would like for me to learn to shoot a handgun but I’m concerned that recoil might hurt my shoulders again. they are still both moderately painful especially at night and I don’t want to do anything that will retear or cause more problems. I think my hand strength may be a problem Also. Am i bring foolish to want to do this?
Fixing rotator cuff tears at your age does carry with it a much lower success rate. Health issues can impact your recovery from anesthesia and the overall surgery as well.
Dr. Luks,
My husband, Chuck, is 86. He walks briskly 2 to 3 miles a day about 5 days a week. He enjoys working at household tasks in our new condo. We travel, and hiked around the Pompeii remains in Italy this fall. He wants to go back to riding his bike.
He has low blood pressure and sees the doctor annually. He is on no medications, but does take supplements.
He has some sleep apnea, and a c-pap which he does not use.
He comes from a family of 8 children. Of those who have died, 3 were in their 90’s, one died in her 70’s of cancer. Of the 4 still living they range from mid 70s to 93.
On Christmas Eve day he slipped on the ice while walking the dog. He fell hard and could not get up. The left shoulder was dislocated and he was put under briefly to put it back in place. He had an MRI Dec. 28th.
Because they could not contact us by phone, we did not get the mri results until we saw the orthopedic surgeon on the 4th. The doctor told us he had a rotator cuff tear. Then he began warning us that surgery at his age carried too much risk, that infection was more likely at his age, that his shoulder might never heal, and asked how often Chuck would need to lift his arm over head. So we asked if he would not recommend the surgery and he said he would not care to do it.
So we came home and later in the afternoon we got the letter from the MRI clinic saying: “1) he has a complete tear of 2/4 of his rotator cuff muscles. 2)this requires surgery in for him to have shoulder function again, 3)please follow up with orthopedist Kiesau on 1/4/17 as scheduled.
Since then I have followed up to schedule a new opinion.
I have read your complete column found on this site. Chuck is reading about the surgery itself. Would you dismiss the surgery out of hand or proceed with getting another opinion. Do 86 year old men ever successfully opt for this surgery?
Dr.Luks, I am coming up on age 77 and I would do this in a heartbeat, so I need perspective.
Elizabeth Moore
There are so many variables that go into surgical decision making. His age is just one consideration. A second opinion seems logical.