
You have fallen, you can not move your arm, and you have been told that you have a rotator cuff tear. Do you need to consider surgery to repair your rotator cuff?
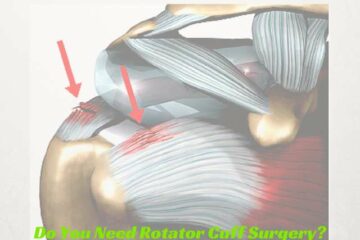
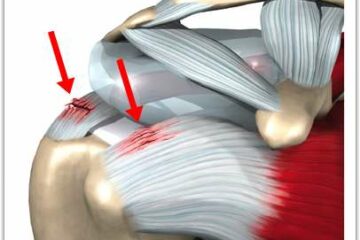
Types of Rotator Cuff Tears
In our first Expert Series post we explored the cause of rotator cuff tears. What explained that the majority of rotator cuff tears are due to degeneration or attrition of the rotator cuff. Simply put- your rotator cuff tendon simply wore out.
Alternatively, trauma, such as a fall, or an accident can also cause a rotator cuff tear. When it comes to managing patients with traumatic rotator cuff tears most Orthopedic Shoulder surgeons are in agreement. There is a significant difference in the management of acute traumatic tears of the rotator cuff, versus the more common degenerative or attritional tear that we see. As discussed in our last Expert Series post, the initial treatment of a small degenerative tear is nearly always non-surgical.
Do We Recommend Surgery for Traumatic Rotator Cuff Tears?
In this post, our experts will discuss their thoughts on the management of traumatic rotator cuff tears.
Marty Leland, MD: Website, Twitter, Facebook
This depends on the activity level of the patient, how much pain and weakness they have, how long has it been since the tear and if they are starting to see any improvement or are things staying the same or getting worse. Night pain is also a sign that a patient has a higher likelihood of needing surgery. Also, the larger and more retracted the tear, the more I worry that they will not get better unless they have surgery. If I have a patient in their early 40s that works in heavy labor with a traumatic rotator cuff tear that has not shown any signs of improvement in 4 weeks, I might get an MRI right away and then discuss arthroscopic surgery. However, if I have a 70 year old retired patient of low physical activity that tore their rotator cuff slipping on the ice, I definitely want to try a significant course of non-operative treatment before discussing surgery.
Jeffery Berg, MD: Website, Twitter
I always try to fit the treatment to the patient…not the patient to the treatment, so I don’t have absolute rules. If the patient is younger than 65 yo healthy and active, I will almost always recommend surgery. If they are older and active, I will also usually recommend surgery. In patients that are less healthy, older and/or less active, I will consider nonoperative treatment but counsel them that their symptoms are likely to persist, progress or, even if improved over the short-term, could recur in the future. At that time, the tear may not be repairable or if repairable, will likely have a poorer prognosis for healing.
Scott Slattery, MD: Website, Twitter
When an acute, traumatic rotator cuff tear occurs and creates a sudden loss of function, I generally recommend surgical treatment. Patients do not tolerate sudden, significant tears as well as the slow, progressive degenerative tears. Several studies have shown that the best results, with acute tears, occur if the tendon is repaired within three months of the injury.
Derek Ochiai, MD: Website, Twitter
For acute, traumatic rotator cuff tears, I would recommend surgery. Typically, these tears can be more extensive and retracted away from the bone, making non-surgical intervention less likely to be successful. Also, acute traumatic rotator cuff tears in patients over the age of 40 years old can occur in combination with shoulder dislocations. If a patient over 40 has shoulder pain following a shoulder dislocation, I would have a high index of suspicion for a rotator cuff tear.
If you are a healthy, active individual who has slipped, fallen or have been in an accident and you have suffered a traumatic tear of your rotator cuff then your surgeon is likely to recommend a repair to give you the best chance at having a pain free, strong shoulder.
Once again I would like to thank our experts for their contribution to your education on the management of rotator cuff tears and shoulder pain.








I am an active 59 year old male who slipped and fell on the ice and injured my left shoulder. An MRI showed the following:
1. Full thickness tear of the supraspinatus tendon with tendon retraction. Partial thickness tear of the infraspinatus and subscapularis tendons.
2. Superior and posterior labral tear.
3. Large glenohumeral joint effusion with debris.
4. Mild osteoarthrits of the glenohumeral joint.
I am currently trying physical therapy for 30 days to avoid surgery. I am reluctant to have surgery since I developed a DVT when I had ACL replacement surgery 17 years ago. I am fearful of developing a blood clot again. Are my fears warranted? Is there anything that can be done either pre or post operative that can reduce my chance of a blood clot?
Hi Mark … yes. In patients at high risk for a recurrent DVT we will often start “blood thinners” or aspirin therapy after surgery and continue for a few weeks. It doesn’t bring the risk to zero, but it does diminish the risk. It also adds the risk of bleeding to the risks of surgery…