
Rotator cuff tendinosis is a very common cause of shoulder pain. Your rotator cuff tendons control the motion of your shoulder joint. They are four very important muscles and their structure can change with age, or because of your activities.
What is Rotator Cuff Tendinosis?
Tendinosis of the rotator cuff is a degenerative (genetic, age or activity related) change that occurs in our rotator cuff tendons over time. Rotator cuff tendinosis is exceptionally common. Although many people with shoulder pain will be found to suffer from tendinosis. Many, many people have tendinosis of the rotator cuff and do not even know it. Why rotator cuff tendinosis bothers some people and doesn’t bothers others is currently a question the orthopedic surgery community can not answer. Rotator cuff tendinosis is just as likely to be found in a professional body builder as it is likely to be found in a true couch potato.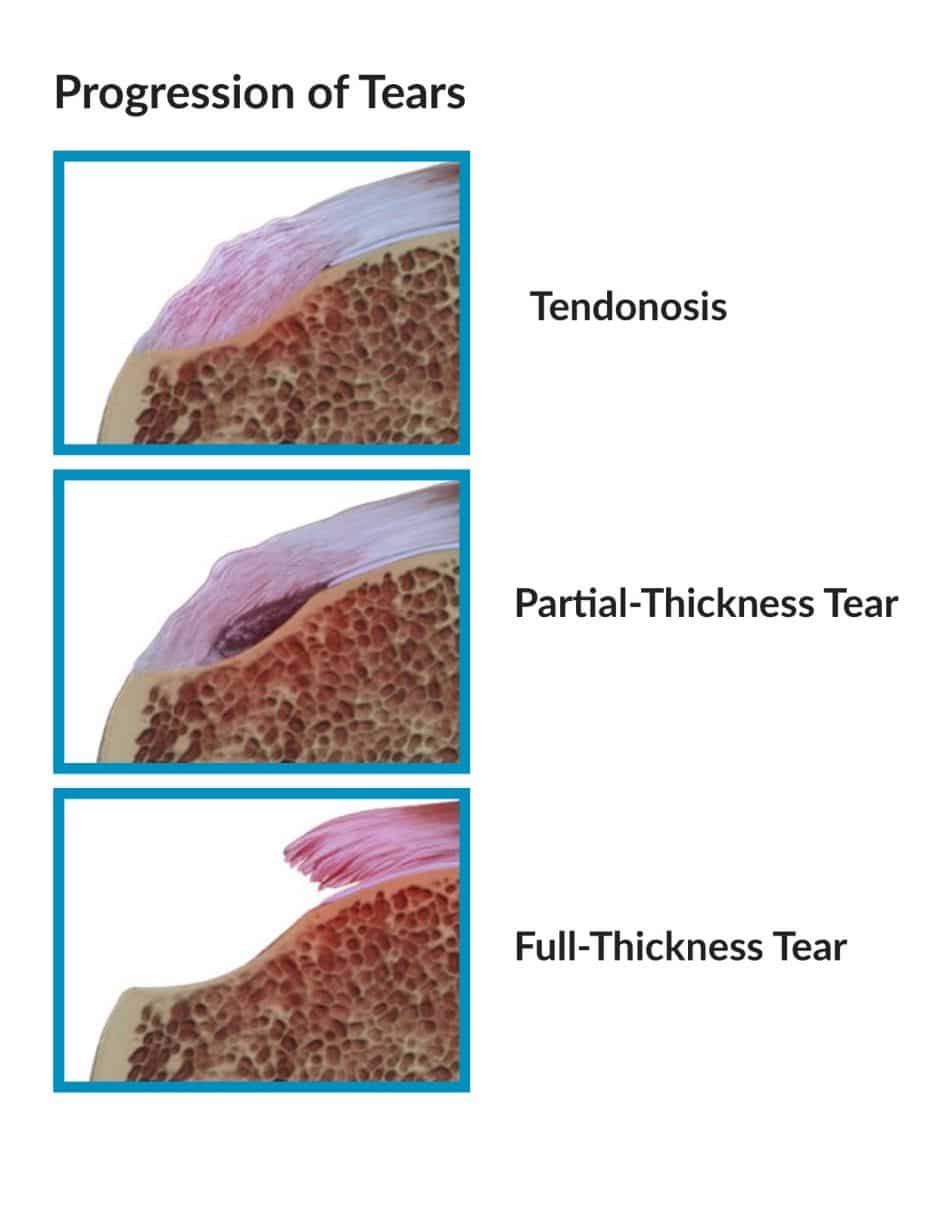
What does Rotator Cuff Tendinosis Look Like?
 In this photo, the white round structure on the right is the top of the humerus. The frayed tissue just to the left is the rotator cuff. This patient was suffering from rotator cuff tendinosis and a partial-thickness cuff tear.
In this photo, the white round structure on the right is the top of the humerus. The frayed tissue just to the left is the rotator cuff. This patient was suffering from rotator cuff tendinosis and a partial-thickness cuff tear.
Tendinosis represents a structural change in the tendon at a microscopic level. This results in disorientation of the tendon structure and, ultimately, partial tearing as the weakened tendon gives way. The analogy I always use is your favorite pair of blue jeans. You wear them for years and then one day you feel a breeze down by your knee — you look down and there’s a hole. No trauma, no accident… the fabric just wore out.
Therefore, rotator cuff tendinosis is not the result of a single traumatic event. It is brought on by genetics, age and repetitive activity. We are not sure why some patients with rotator cuff tendinosis have pain, and others do not.
How Do We Treat Rotator Cuff Tendinosis
Many patients with rotator cuff tendinosis and partial tears do not require surgery and will respond very well to a coordinated physical therapy program to strengthen the remaining cuff tissue. Moist heat, Ice and anti-inflammatories can work well, too.
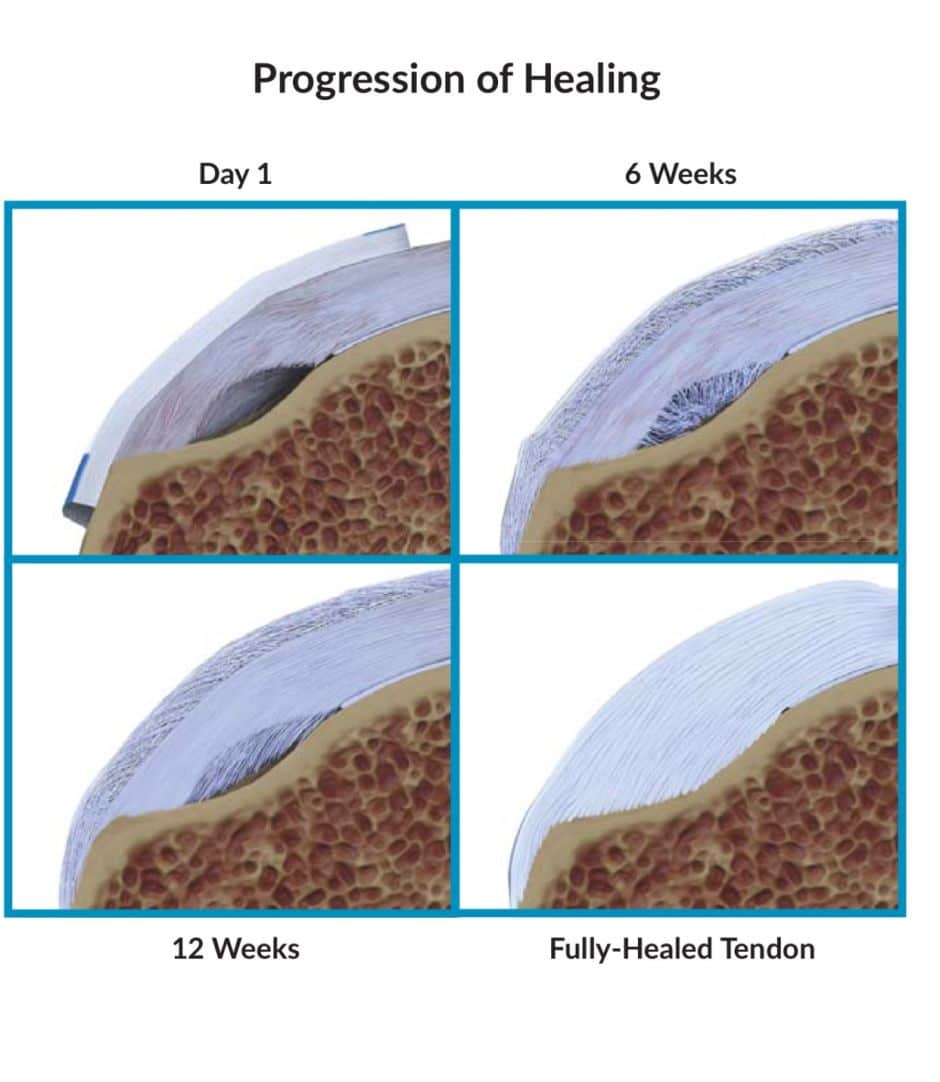
Rotator cuff tendinosis is a biological problem … our body is actually changing the tendon tissue. Only very recently have treatment techniques evolved to enable us to treat rotator cuff tendinosis that fails to respond to non-surgical measures. It is a technology developed by Rotation Medical and enables us to place a “bioinductive” patch over the area of tendinosis, which over a period of a few months has been shown to reverse the degenerative changes and heal your tendon.
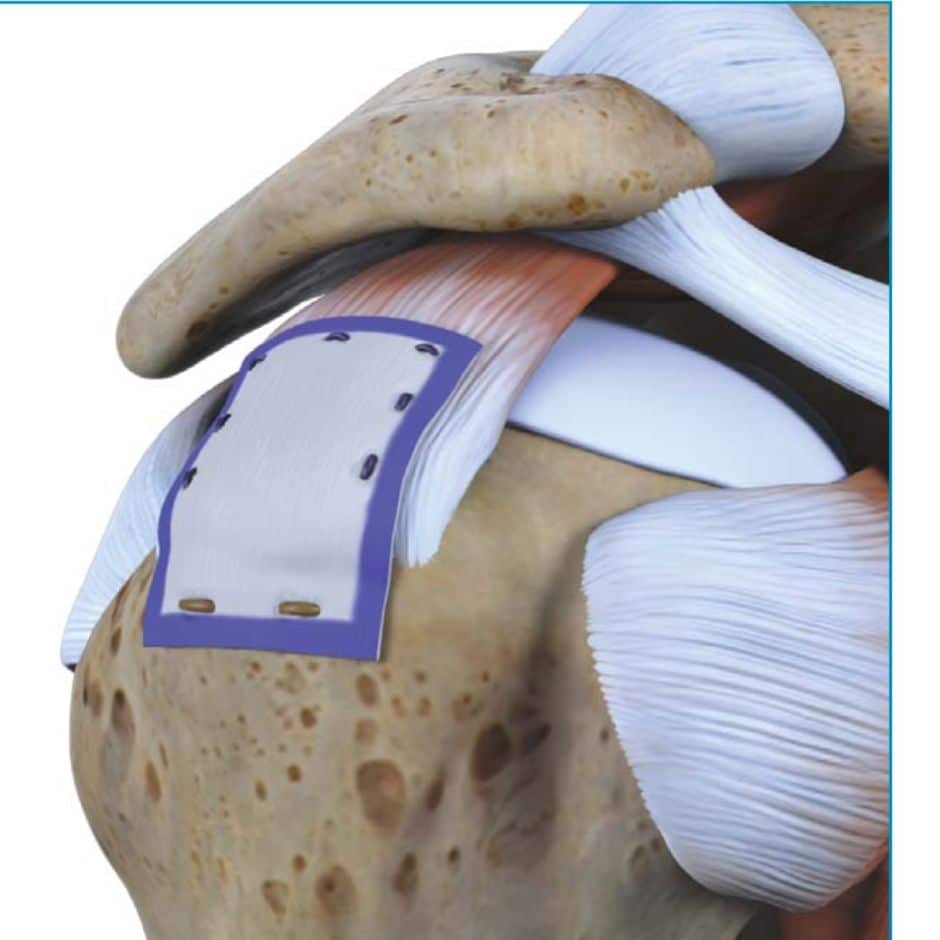
Over time, this patch will incorporate into the tendon and alter the structure of the tendon. Most patients .. in our series to date, have had significant relief, even after trying other surgical procedures first which had failed.
You can read more here about this approach to treating shoulders with rotator cuff tendinosis.
Do you have questions regarding an Orthopedic injury or longevity?
Do you want to talk to an expert who can listen to you for 45-60 minutes and explain the options in detail?
Dr. Howard Luks offers remote guidance sessions to review your X-ray or MRI images and explain your options.
Dr. Luks has also received hundreds of requests for educational sessions on the topics discussed in his book, Longevity Simplified.









Debbie Ball
Dr. Luks,
I have a tear in my rotator cuff, and a torn lining in my left shoulder. In my right shoulder, I have a torn ligament, bursitis, tendonitis, and arthrosis. I’m attending therapy sessons at the moment. If the therapy sessons don’t heal these problems, and my orthopaedic surgeon is not familiar with the patch process that you use, will you accept an out of state patient to receive this surgery?
Yes, we have helped out many from around the US and abroad.
Ronald Yates
Your website was very informative. According to a recent MRI, I have severe tendinosis of the supraspinatus tendon trace partial-thickness articular surface tearing at its insertion and severe tendinosis of the distal infraspinatus tendon with a small articular surface tear at its insertion. A small amount of delamination is also noted. The remaining cuff tendons are normal.
I also have full-thickness cartilage loss at the anterior inferior glenohumeral joint. Moderate cartilaginous thinning w/o focal defect throughout the remainder of the glenohumeral joint.
I was especially interested in the “bioinductive” patch treatment you reference on your site. Given the description of my problems would I be a valid candidate for that kind of treatment?
Perhaps… certainly something worth talking about with your surgeon.
debbie mckinney
I have a full thickness tear of my posterior supraspinatus right side. I opted for autologous stem cell/prp treatment to try to avoid surgery. It’s been 6 weeks, and I have now lost all internal rotation and my pain is severe. Went back to the doctor who did an US and he found biceps tendon effusion. I feel I am way worse than before the therapy both in terms of pain and range of motion. The doctor wants to do more PRP injections which I am open to, but am afraid that things might be made even worse. I don’t know what to do at this point. Any suggestions?
Early in the process of developing a frozen shoulder people will have pain, but no loss of motion. As the weeks go by they lose motion and have pain as well. Perhaps you should see a second opinion or your first Orthopedist to determine if you have a frozen shoulder… which is not typically treated with PRP. This post on frozen shoulders might be worth reading…. https://www.howardluksmd.com/orthopedic-social-media/frozen-shoulder-diagnosis-options-treatment/
LuAnn Krothe
Hello,
I am a 56 yo extremely active nurse. I run marathons and half marathons as well as competing in other distances. I also lift weights but haven’t lifted heavy in years. I had chemotherapy and radiation for breast cancer 8 years ago. Had shoulder pain three years ago w a large rotator tear. Had surgery and didn’t go well. Surgeon had to go back to repair things at six months. Thinking radiation had a part in this. I’ve had opposite (good shoulder) shoulder pain for a year w cortisone inj twice into shoulder capsule via ultrasound. Mid December intense pain wo relief after cortisone and bicep pain as well as rotator sleepless nights. Backed off push ups and pull ups and had a MRI arthrogram.
Report is as follows. High grade near circumferential tear of glenoid labrum. Thinning of cartlidge w superficial fibrillation at the glenoid humeral head motion defect disallows detailed cartlidge anatomy.
Severe AC joint osteoarthritis w loss of normal subacromial fat. Subacromial sub deltoid bursitis.
Tearing of the biceps labral anchor. Severe intra-articulate biceps tendonosis w intra substance tear. Medial subluxation of proximal biceps tendon. Biceps tendon is present win the groove and shows severe tendonosis and intra substance tear most prominent at its proximal aspect.
Rotator Cuff: supraspinatous high grade full thickness tear. Insertion fibers intact and a separation of 2.2 cm between the torn margins which are frayed and irregular. Measures 1 cm in anterior posterior dimension. Severe supraspinatous tendonosis. Mild muscular atrophy. Partial thickness Infraspinatous articulate sided tear if the conjoined tendon. There’s minor is normal. High grade full thickness tear of the subscapularisw severe tendonosis. Normal marrow.
Waiting to see orthopedic surgeon. Pain is intense. Last two weeks unable to lift my arm. When I do bend my arm at elbo intense bicep pain. I do not take pain meds or NSAIDs. Just wandering if they can patch these tendons w major multiple tears and how so they great the labral tears and arthritis. Realize the osteo is a remnant of having chronic tears for a long time. I am 5’9 and 125 lbs extremely for and just need to run. I really don’t want to hear the words reverse shoulder replacement. What are your thoughts with these results. Also could 6 months of chemotherapy and radiation caused some of this damage. Thanks for your time.
Hi …
This is a complicated case. You have many potential pain generators. Without examining you I cannot offer specific treatment advice. This should be used more as an education and serve as something to assist you with your research and with your discussion with your doctor.
Given the OA, the labral tear can likely be ignored (most labral tears at our age can be ignored). The rotator cuff issues appear to be relatively straightforward and repairable. Often times we will place the patch over a more traditional repair. The subscapularis might require a small open procedure. Given the medial subluxation and degeneration of the biceps your surgeon might recommend a biceps tenodesis. In order to bypass all the degeneration in your biceps many would choose a sub-pectoral tenodesis.
Good luck !
Chris
Thank you for this helpful information. I live in Westchester county and recently had an MRI that revealed rotator cuff tendinosis with a small partial thickness articular surface tear infraspinatus and minimal partial thickness tear supraspinatus with no full-thickness tear. I will be following up with my doctor next week but wondering if you could offer a second opinion based on this MRI or if I would need another.
HI Chris… We will not likely need a new MRI. I would be happy to see you.. .we are on Bradhurst Avenue in Hawthorne. 914-789-2735
Howard Luks
Lillian Loggans
Thank You so much Sir! I do appreciate the work you do. I am a retired Medical Record Administrator and a Medical Staff Coordinator. I am very appreciative of the work that our Physicians perform every day and certainly you are one of the best in your work. Thank you for sharing this information.
Lillian Loggans
Dr. Luk: I am a patient at the Southern Bone and Joint Specialist in Hattiesburg, MS. I had to cancel two appts. for shoulder repair due to torn rotator cuff due to other medical problems. I am 84 years old and I am interested in the patch you are doing. Would you be kind enough to let me know if there is a doctor at the Southern Bone and Joint, and if not, where the closes to Hattiesburg, MS that they are doing this procedure. I am not able to sleep in a bed because I can only sleep on my sides due to an enlarged hiatel hernia that pushes my lungs under my heart and I cannot breath good. I really need and would definitely do this procedure if I can find a MD that can perform it safely (of course, anything is always possible) and I can be close to home where my family can be of help.
Lillian Loggans
[email protected]
HI Lillian ..
The company is called Rotation Medical. They can be found online and can assist you in finding a surgeon near you.
Good Luck !
jeisenbrey
Very informative! After 4 months of trying different things due to the insurance requirements (x-ray, Meds, PT, MRI-finally for an actual diagnosis) I was diagnosed with tendinosis of the rotator cuff. Actually in both shoulders but only symptoms in one. Per my doctor the next step is cortisone shots. However, prior to that I am taking ibuprofen three times a day, using a “tens” machine once a day and will start basic PT exercises again. Based on the info I have given (and I know it is not much) but in your experience would swimming be okay to incorporate during the healing process?
Thank you sir.
Denise Rowe
Can you answer with some options with caveats ( 1….2..3) based on your experience of how you might possibly approach this? I need your insight.. Thanks
Denise Rowe
I am a 55 year old female, African American.. I am a nurse practitioner working in primary care. Spring 2015 I had arthroscopic surrgery on the left shoulder after a a heavy door slammed into my outstretched hand left me with severe impingement syndrome , large joint effusion and a frozen shoulder that prevented overhead and behind the back movement. Extensive debridement and removal of 2 large bone spur at AC and distal clavicle was done. I had intensive PT for 8 weeks and the left shoulder is now back to normal.
I have been having gradually worsening left shoulder pain over the last 6 months , only thing I can thing of that may have-hurt me in retrospect Is working out on elliptical machine with a lot of resistance on the upper arms. Didn’t think I was hurting myself. I have pain in humeral head terrible with over head movements, painful arc at 90 to 120 degrees, nighttime pain in anterior shoulder over biceps, anterolateral deltoid and postero lateral supraspinatus. I have terrible night pain and cannot sleep much due to the pain. The anterior shoulder joint is now visibly swollen and tender to deep palpation. I have been on regular NSAIDS for more than 3 months per advise of my PCP who told me I had bicep tendonitis, and to rest it. I have been using ice and heat as well. My range of motion in trying to move my left arm behind my back is severely limited, I can get my left arm to the lower part of the left buttock only and no further. Had X-ray 2 weeks ago which showed soft tissue swelling but no boney deformity, fracture or boney destructive lesion.
MRI reads as follows:
Bonesand bone marrow: normal bone marrow signal is seen within the glenoid. You will head posterior lateral demonstrates bone marrow edema surrounding several developing sub cortical cysts. Acromial clavicular articulation demonstrates no diastasis or subluxation but there is edema within the joint space as well as a edema within the superior and inferior capsule.
Biceps: long head of the bicep courses to insert in the labral biceps anchor.m there is mild tenderness is of the intra-articular course of the long head of the biceps. The Short head of biceps insertion the coracoid .
Labra: intra substance degenerative changes are seen involving the anterior superior labrum along with the blunting of its margins .
Rotator cuff: the teres minor muscle and tendon are unremarkable.The infraspinatus muscle and tendon are unremarkable with the exception of a portion of its humeral head insertional fibers which demonstrate mild tendernosis. Supraspinatus muscle is unremarkable.Supraspinatus tendon demonstrate more extensive tendonosis of it’s posterior lateral fibers and to lesser degree it’s anterolateral humeral head insertional fibers.The subscapularis muscle is unremarkable as is the subscapularis tendon. Mild amount of subacromial subdeltoid bursitis is noted.
IMPRESSION: tendonosis of the posterior lateral fibers of the supraspinatus tendon as well as the entire lateral humeral head insertional fibers of the supraspinatus tendon. Mild tendinosis of a portion of the humeral head insertional fibers of the infraspinatus tendon D2 which multiple small foci of bone marrow edema arsine surrounding developing sub cortical cysts. Mild subacromial sub deltoid bursitis. Tendinosis involving the articular course of the long head of biceps tendon . Blunting and intrasubstance degenerative changes involving the anteriorsuperior labrum. I chromic clavicular joint fluid and capsular edema but without diastasis or subluxation .
I am in a lot of pain,, I cannot take opioids and do my job, the shoulder joint feels pretty stiff. My PCP says I need to be scoped to clean up the damage. What is you opinion on what I need to do next?
nothing there screams that it needs surgery. Without examining you i can’t say what treatments I would recommend first.
Brigid
I’m 68, last January I shoveled my driveway of the one and only major snow fall we had, 14 ” …it took me all day. Since then I’ve had right arm/shoulder pain. MRI a couple of weeks ago indicates tendinosis. I did PT in the spring when I self diagnosed the problem as biceps tendonitis but got no improvement. So now I’m wondering if going back for more PT with the proper diagnosis will work? I’m relieved that there is only a minor tear but would like to find a good treatment plan soon. Acupuncture has been suggested in other websites. What else Vann I do? Brigid
Therapy and possible injections are a good place to start if the pain is due to tendinosis.
kiki
I Slipped on ice and fracture my bone in then thumb and started to have pain in shoulder , had a MRI of the shoulder and this is the finds. can you tell me is there a tear in my rotators cuff?
Findings:
There is no glenohumeral joint effusion. There is no significant fluid in
the subacromial/subdeltoid bursa. No evidence of labral tear on this
noncontrast MRI. The cartilage is within normal limits.
There is moderate supraspinatus and infraspinatus tendinosis. There is
mild subscapularis tendinosis. And subscapularis tendons are intact. No
full thickness rotator cuff tear. Satisfactory muscle bulk surrounding
the shoulder girdle. The long head of biceps tendon is intact within the
bicipital groove.
There is mild acromioclavicular joint degenerative arthropathy with edema
across the joint and subchondral cystic changes and osteophyte formation.
There is no subacromial spur.
No mass lesions are identified in the suprascapular or spinoglenoid
notches. The fat within the quadrilateral space is preserved.
Impression:
Rotator cuff tendinosis. No full-thickness tear.
Nope… no tear. Just tendinosis… but tendinosis can hurt. Physical therapy is generally successful at alleviating the pain. Speak with your doctor about your options.
Jason larsen
Dr. Luks, I had a small gradual pain in the shoulder before and after lifting weights about two years ago and took NSAIDs which helped for the first couple of months but the pain keep getting worse(I continued to work out while taking NSAID’s) which lead me to take more and more NSAIDs. Long story short i took two months off any weightlifting activities and continued to experience pain(though the pain now was everyday and NSAID dont seem to help any) so I went to the doctor and had an mri done and he told me the Mri didn’t show “much” and said I was probably experiencing tendinitis. I did some RC strengthening which didn’t seem to improve the pain. Since then I have recieved a corticosteroid shot which didn’t help at all and had another mri recently. After reading online about tendonosis I asked the doctor if it could be that and he said, “tendoosis and tendinitis are basically the same thing”. Another doctor in the same building told me tendonosis is a age related thing and I was to young to have it. I am now taking all the X-rays and mri’s to another shoulder specialist in another city. My question is, is tendonosis visible on an mri?
Yes.. tendinosis is visible on an MRI… and although young, it can be the source of pain. So can subtle instability and many other issues at your age. You need a good exam… not another MRI.
Diane Porritt
Dear Dr Luks
A recent MRI scan gave the following Clinical Report:
“There is an 8mm area of high signal in the distal insertion of the supraspinatus is some signal change and a small subdeltoid subacromial bursa. The infraspinatus has a normal appearance. Thereis an inferolateral acromion with no bony spur. No bone marrow bruising. Biceps tendon is in the correct position. Superior label tear propagating interiorly keeping with SLAP lesion. Biceps anchor is normal.
Comment: Partial tear of the supraspinatous and interior superior labral tear (SLAP Lesion).
I am 64 years old and very fit however, an outstretched hand fall 2 years ago, followed by a pull from a husky dog running away with me, finally followed by throwing a heavy bag on my shoulder has all compounded to pain in my right rotator cuff. Still have full range of movement though. In your experience would I need surgery as I am being recommended to have?
Would you have any advice please? Thank you in anticipation. Diane
What surgery are they proposing? What treatments have you tried already?
Jerri
Dr. Luks,
After having knee surgery a few year ago I injured my shoulder from possible over use because I had injured both knees and couldn’t bear weight on either and relied on my shoulder. One day I was lifting myself up to stand and heard a pop and burning sensation in r. shoulder. After this I couldn’t lift my arm up for two months and I have been delayed on getting an mri due to insurance delay. Its been 2 1/2 years now and in a few weeks I will be getting an MRI done. Will the injury still show up? I still have pain especially sleeping at night, while driving a car, lifting and drop things I try to hold in the same arm as the injured shoulder. All the dr are pretty sure its rotator cuff. How possible will it be to fix the issue now since its so long since the acute injury happened? How do you know its rotator cuff or tendinitis?
thanks
Jerri
By the way love your informative site thanks for taking the time to post about these conditions.
Thanks Jerri !
The “injury” will still show up despite the long time since you hurt it. Usually our exam and your history tells us whether or not we are dealing with a rotator cuff tear, tendinosis, or something else.
Our ability to repair tears is affected by the passage of time… but not in all instances. And there are many tears that do not require surgery. Good luck with your MRI… feel free to stop back after you know the results.
Howard Luks
Darlene
I’m now a 55yr old female that was working as an overnight grocery stocker. It required me to do a lot of lifting and arm movement when stocking the shelves. I had tennis elbow and wrist surgery. Over a period of time my shoulder started to cause me pain. In 2009 I was to have surgery on my shoulder(rt) due to circumstances I didn’t.,the pain sometimes goes to the left but mostly on the right. I left my job of 28yrs because the pain has gotten much worse and because workmans comp has denied me I have no medication and after what I was prescribed doesn’t help the pain. Why is it that not doing anything still cause pain and is there any resource. I was told that the headaches is caused by it also, thank you for your help
Rotator cuff pain is frequently very severe at night. The night pain component can keep us awake, interfere with our ability to get a full nights sleep —> which leads to stress. We’re not sure why the rotator cuff hurts so much even at rest or at night, but it is a very common complaint among patients.
Dorothea
Here’s my history: I’m 33 and active in many different kinds of sports (rowing, skiing, swimming, going to the gym). Four days ago I felt a sudden pain in my shoulder when holding on (with my arm straight, flexed foreward) to a big rowing boat (for 14 rowers) when it moved with greater force than I had expected. Since then I’ve had a dull ache in my shoulder (also at night, but it’s not very severe and I still can sleep most of the time). I have full range of motion and no additional pain when moving my shoulder in different positions (abduction, adduction, internal and external rotation). I haven’t noticed any pain when trying to palpate (maybe a little tenderness at the subacromial space, but I’m not sure. I’m not good at palpating). My question is: can this be a tear despite any pain with movement of the shoulder, only at rest. What else can it be? Should I see a doctor and if yes, how soon? I’m now taking NSAIDs and resting the shoulder. Is it safe to take pain (or the lack of it) as an indicator for when it is safe to return to normal activities, like rowing. I’m quite worried and really appreciate your web page (I’ve learned so much from reading it) and you answering people’s questions so kindly.
Hi Dorothea…
The major offenders in that case are the rotator cuff, the labrum and the biceps. Without examining you it’s obviously impossible to say which it is. If rest, stretching, and perhaps routine over the counter medications are not improving your symptoms then after a week or two I would probably see an Orthopedic Surgeon who specializes in treating the shoulder.
Howard Luks
Stephanie
What a great website! I’ve learned more here than I have from my doctors and research combined. I have severe pain at night and when I googled it, I found your website. I have full thickness tears in both shoulders and a bone lesion. I am a school teacher am waiting to schedule my surgery date. I’m not pleased with my doctors bedside manner and am waiting to see if my insurance will approve another …healthcare is Mississippi is not easy and I have good insurance. I am afraid that my tendon retraction and atrophy is to the point where surgery may not can help. I am going back to explore more on your website and educating myself more.
Very kind of you Stephanie … Good Luck !
andrea
I have RSD AKA CRPS in my right foot and ankle and I go every 3 months for a lumbar block in order to keep it in check… when the shots wear off my foot starts to hurt and and freeze up … lately my shoulder was giving me problems so I had it looked at and after my MRI was told I had tendinosis… my question is this … is the reason I am having so much pain with my tendinosis because of the RSD? I dont have the swelling and the blotchy purple looking skin but the frozen range of motion and the pain and tingly feeling are there… maybe Im just paranoid because of the last RSD episode… (it was awful) and was brought on by Achilles tendon damage. Any input would be greatly appreciated as not many doctors are familiar with this disorder
Andrea … anyone with a history of CRPS is going to worry that any new discomfort is related… Completely understandable. While CRPS can occur in other areas, it is well known that tendinosis can cause fairly significant pain. Sometimes selective injections of the shoulder under ultrasound guidance can help determine what the source of the pain is.. and treat the pain as well. The hallmark of CRPS or RSD is pain out of proportion… the color changes and skin changes actually occur fairly late in the process. Your surgeon should be able to help you determine if this pain is related to the shoulder, the rotator cuff tendinosis or perhaps CRPS.
Good Luck1
HJL
Jalen
The power of health care and social media… and a firm digital footprint.
“A wonderful job. Super helpful information.”
Thanks Jalen…