
Degenerative meniscus tears are very common. Many adults over 55 have one and will not know it. Surgery for degenerative meniscus tears is rarely necessary. Most research shows that people do just as well with physical therapy. This post will carry two messages, both equally important. First, surgery is rarely necessary for degenerative meniscus tears. Perhaps even more important is that once your knee feels better, and it may take several months, you should try to return to your normal activities.
Think about this second statement for a moment. If you had an episode of knee pain, and you had an MRI which revealed a degenerative tear; even though you now feel better you may not return to being active because you are afraid of harming your knee. Arthritis and other conditions worsen, even if you are at bed rest. Meniscus degeneration and tearing are no different. It is more of a biological issue than a mechanical issue. Meaning that you cannot stop the process, so you might as well remain active.

Why would you want to slow down your activities which are decreasing your risk of diabetes, obesity, dementia, hypertension, heart disease, and stroke? Rest comes with a heavy burden with respect to your overall health.
Recent research about degenerative meniscus tears and surgery:
The meniscus is a cushion inside your knee. It aids in the stability of the knee and minimizing the stress across the knee, thus minimizing the risk of developing osteoarthritis.
Meniscus tears are incredibly common. Although meniscus tears occur in all age groups, they are most common in adults over 55. There are many different types of meniscus tears. By far the most common tear is a degenerative tear of the posterior horn of the medial meniscus.
An article published in the New England Journal of Medicine out of Finland studied patients with degenerative meniscus tears. They studied whether the results of an arthroscopy (surgery) was better than a sham surgery (where the patient is brought to the operating room and thinks they had the surgery).
As published in the NY Times, The authors found …
A popular surgical procedure (arthroscopy) worked no better than fake operations in helping people with one type of common knee problem (degenerative meniscus tear), suggesting that thousands of people may be undergoing unnecessary surgery.
The Wall Street Journal posted a similar article, and led off by saying…
A fake surgical procedure is just as good as real surgery at reducing pain and other symptoms in some patients suffering from torn knee cartilage
These findings are not new, but in this environment perhaps they will shine a light on the over-treatment of degenerative meniscus tears. In 2007 a study showed that the results from an arthroscopy for a degenerative meniscus tear were not superior to a supervised exercise program.
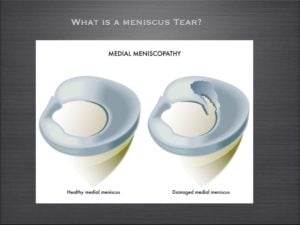
What is a degenerative meniscus tear?
Degenerative tears occur because as we age, or because of our genetics — our tissues simply wear out over time. A degenerative tear is frayed, worn out tissue that looks like the worn out area on the front of your blue jeans. It has very little character, and the tissue is thin, soft, flexible, and looks worn out when we view it at the time of surgery. Most of these changes we see in the meniscus we consider to be “age-appropriate.” We accept thinning hair, the need for glasses, slower running times, and so on… but none of us expect that our internal structures are showing signs of aging too.
For many many years, I have spoken to people about the fact that many meniscus tears, especially degenerative meniscus tears do not often require surgery.
Do I Need Surgery For a Degenerative Meniscus Tear?
Many patients are under the assumption that because something is torn, therefore it must be fixed. That is not the case for many issues in Orthopedic Surgery. This paper on the non-surgical management of degenerative meniscus tears versus surgical management is yet another in a series of papers that supports the non-surgical management of degenerative meniscus tears, especially in the setting of osteoarthritis. Despite how severe your pain is at the onset of your symptoms, typically within a few weeks, your knee feels much better if managed by physical therapy, ice, heat, and anti-inflammatory medication (if you tolerate it).
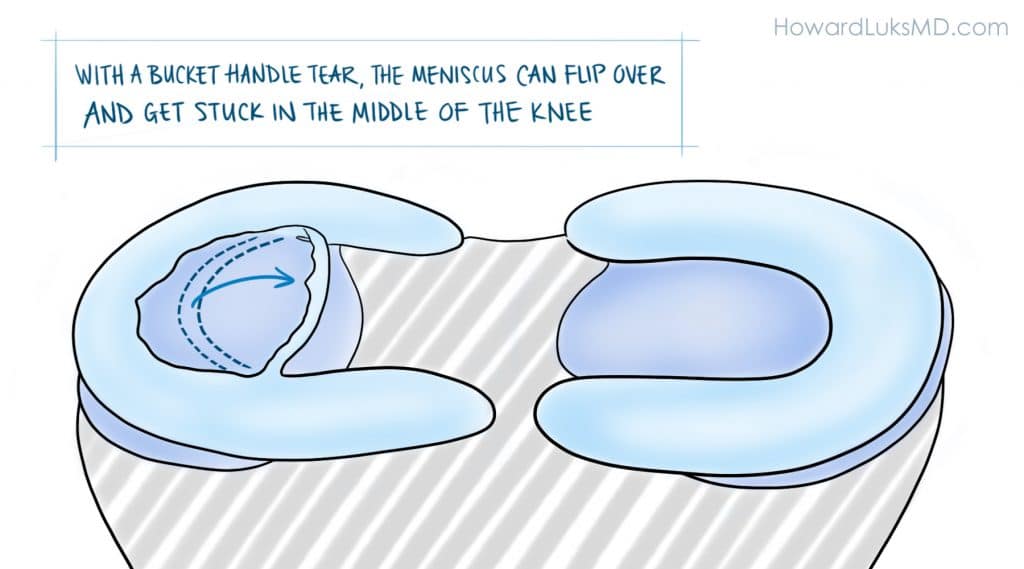
It must be pointed out. The authors of the paper studied degenerative meniscus tears. They did not study the more unusual “radial”, “flap”, or “bucket-handle” tears that can occur in the meniscus. These other tears can be far more “unstable” and produce mechanical symptoms such as instability, buckling, and giving way. In those instances, a meniscal repair, or removal of the torn flap will more than likely be necessary.
This was an important article about the management of this type of meniscus tear, but more studies are necessary. The take-home message is simply that all meniscus tears do not need surgery. Degenerative meniscus tears are usually managed well without surgery.
Have realistic goals about your recovery.
Very few of your orthopedic issues will resolve in less than 3 months. Many of you were told that if your pain persists for 4-6 weeks you should consider surgery. I would suggest that you wait longer than that. With 25 years of treating people under my belt, I can tell you that the majority of people were glad that they waited longer before moving forward with surgery. Surgery might actually bring you closer to a knee replacement. Surgery for degenerative tears will not decrease your chances of developing osteoarthritis. If you do choose to proceed with surgery for a degenerative meniscus tear it should be because:
- your pain persists after a lengthy period of non-surgical management,
- it was a quality of life decision…
- and your surgeon told you that you have little or no arthritis in your knee.
When your visit with your doctor be sure to ask what type of tear you have. If you possess a degenerative tear, without any of the “mechanical” symptoms we mentioned — you should pursue non-surgical treatment at first— and a few months later I think you’ll find that you’re glad that you did.









Dr Luks,
Please give me some advice.. I’m a 32 year old healthy female who enjoyed more than anything to jog and go for runs. I suffered a fall on some water an an amusement park and I hit my knee extremely hard. X-rays showed no fractures but I got an MRI done which impression reads grade lll tear of anterior horn of lateral meniscus and Grade II signal of the posterior horn of the medial meniscus. I haven’t ran in over 4 months which is such a great loss to me. I just want to run that’s all I want. I don’t particularly want surgery… What has been your experience with this type of injury. I have minimal if any pain.
Most noticeable discomfort or limitation noted is when I squat just right or sit in an Indian style postion which I change up right away to protect my knee… PLEASE HELP
[email protected]
why aren’t you running now? Pain? Fear? Being told not to?
I have not ran for fear of causing further injury. I am waiting to see an orthopedic MD to tell me what I should and shouldn’t do.. I’m willing to do my part.. Physical therapy., or even not running for as long as suggested if that is what will help… I’m looking for direction as to what to do or expect.. The times I have had to do some quick running minimal pain maybe mild soreness..I’m a linear runner maybe some incline no crazy sports just easy cardio for maintains health and weight… What do you think?
Hi Howard,
Thank you very much for this really helpful information on degenerative meniscal tears. I am a physical therapist in my early 50s, have run many marathons, last half marathon in March this year. I think I have a degenerative meniscal tear, no locking, giving way or instability symptoms. With quads strengthening, etc and once pain symptoms have reduced would I be able to carry on running? I am aware that without the protection of the medial meniscus I may develop OA changes in future years.
Thanks again,
Rob
IF it’s not bothering you then there is no reason not to run. Most runners in their 50s likely have degenerative meniscus tears but simply don’t know it.
Hi Dr Lukas
i had inside meniscus repair few days ago and i am non weight bearing for 4 weeks i have to be in the brace all the time what i am worried about is as i was sitting on my sofa i my leg was straight and i put the hill down when my hill touched the floor i felt the pinch where actually my meniscus was repaired do i need to be worried about that?
Thanks
not really , no. Many of us don’t brace and allow motion. Some still immobilize. You will feel all sorts of unusual feelings as your rehab progresses. Follow your docs instructions and good luck
Hello again Dr Lukas
Thanks for letting me know it means a lot for me ! just want to ask you something else regarding my knee 2 weeks post op today and my knee is still hot and as i said had inside meniscus repair i do get aches/pain on the lateral side why is that pain over there is that normal or is something that i have to be worried about ? thank you again for you help!
Dear Dr Luks
First, a 1000 thanks and then some, not only for your truly excellent and mega-informative website but also for this global query/answer opportunity: amazing. All that has helped me hugely, to get through my last three really draining weeks, once I found your site. Thankyou for your personal and professional generosity and service.
I would so benefit from your input into the dilemma/decision I face with a medial meniscus bucket handle (?) tear. This is, most vitally, in the face of conflicting MRI interpretations, as well as conflicts both about surgery anyway, as you highlight, & in some other ‘reputable’ net research, even on naming of tears, thus on appropriate ‘fix-ups’. My aim is to be as well informed/prepared/responsible as possible for my 3rd (!) Orthopaedic surgeon’s consult, Wednesday morning, 21 Oct. My further aim is to avoid future total knee replacement forever, or defer hugely.
Add in to the mix, the 28 Sep eye-opening ABC TV Four Corners program,‘Wasted’: thought-provoking! It’s primarily about systemic problems in the Australian government’s health care system, highlighting knee arthroscopies (& more) but showing gaps & problems in underlying patient/doctor/specialist information & communication: well worth a watch for any thinking patient & others, I believe: http://iview.abc.net.au/programs/four-corners/NC1504H035S00 till 28 Oct.
I’m another of your Australian fans, Dr Luks, a 67 yr young female, 165 cm (5’6”), 59kg (130lb), sadly way-too-sedentary, with multiple ill health problems. They include spinal osteo-arthritis, early onset osteoporosis (if relevant), & I now know, osteo-arthritic knees. Recent history: Late August, I noticed right knee pain, including catching and twinging, touch-tenderness, giving-way, decreased leg usability and a ‘clunking’ intermittent noise (like smooth driving vs running over a kerb). Pain worsened some by week 5, though improving at first with anti-inflammatories. Though I worked out I’d been working outside, and noticed it from that day, I noticed no ‘event’.
About three weeks ago, I sure did, though. 23 Sep: Favouring the knee, eg not squatting, I was sitting app. 6” (15cm) from the floor, rt leg stretched out, stood up: immediate, pretty severe pain. I didn’t notice any particular noise/sensation: just pain, continuing very high for hours. 24 Sep: MRI said right medial meniscus bucket handle tear, flipped anteriorly and laterally. MRI details below*.
It did not lock, & hasn’t, but I could bear no weight at all (& have been able to only this last week; two crutches till 15 Oct.) Oct 1, thankfully I now see, the scheduled meniscectomy/arthroscopy was cancelled very last minute (already prepped), from anaesthesia complications, ostensibly. O. surgeon left on planned leave, my extra pre-op queries still unanswered, no Plan B, though his staff had said initially it must be soon not on his return.
Trying to find an urgent low cost replacement, I was very fortunate to get phone-only opinion from a leading O. surgeon, via my GP. He generously viewed the report & scans online. He said: “Don’t operate unless locking; no use, maybe harmful, slow healing; actually parrot beak tear, ‘degenerate’ ” (or degenerative/degenerated). His word is uncertain but I understand could mean different things in your world. It sure FELT “traumatic” to me, though I understand the existing degeneration counts! This seems a bit more than ‘frayed’ though. This surgeon seems pretty ‘top of the tree’, up to the minute & leading edge, couple of associate professorships. It is he I’m now seeing Wed 21 Oct.
Meantime though: 2nd O. surgeon, in place from the search, saw me, said: bucket handle, no doubt, operate; radiology firm confirmed their original MRI interpretation (though the same doc); my GP states 8 out of 10 local O. surgeons would do the meniscectomy.
Oct 16: I’m walking, but with not-normal gait, mostly without crutch, with some caution, variable pain managed with very little pain killer (slow release paracetamol only); sharp twinges at times, when I ‘catch’ it, in calf raises, steps. Pain is only in front, seems below knee cap, & front lower inner corner of knee, including to touch.
All comment is so welcome, Dr Luks, to assist my best possible consult Wed. and then my final decision on surgery, but if possible including how a try-hard lay person gets to grips with differing diagnoses (!), whether arthroscopies are worthwhile just to confirm diagnosis, prospects of ‘un-flipping’, how a bucket handle can flip both forward and sideways. This is v. long as I’ve gone for detail, hoping it helps. THANKYOU.
* MRI report: “bucket handle type (sic) tear involving the posterior horn and meniscal body junction of the medial meniscus. The torn meniscal fragment has flipped anteriorly and laterally. A small parameniscal cyst abuts the posterior aspect of the medial meniscus. The lateral meniscus demonstrates minor degenerative change involving its inner free edge.” (Other bits – ligaments, tendons etc – then listed as ok.) “There is mild thinning involving the articular cartilage overlying the most medial aspect of the medial tibiofemoral compartment. There is a full thickness chondral defect involving the anterior aspect of the medial femoral condyle where there is associated subchondral bone marrow oedema. Articular cartilage within the lateral compartment is relatively well preserved. There is mild to moderate chondromalacia involving the retropatellar articular cartilage where there are regions of full thickness chondral fissuring involving the medial facet extending into the region of the patellar apex, where there is subchondral bone marrow oedema. There is moderately sized joint effusion associated with a small Baker’s cyst. Loculated fluid also surrounds the semimembranosis tendon insertions in keeping with semimembranosis (sic) bursitis. There are no intra-articuar loose bodies.”
Annie T
Thank you for the kind comments …and I’m glad the site helped :-)
A bucket handle tear can be a problem… even in people all already have some arthritis.
The surgeon you quoted is correct… unless pain, catching, buckling or instability might be best to leave alone. BUT … if you have catching, locking, etc then the risks of falling are real. Therefore you can consider an arthroscopy. Even in 60 somethings… if the tear appears acute at the time of arthroscopy there are instances when it can be repaired… thus you will feel better and not loose and meniscus. Your surgeon should be willing to consider a repair, despite your age, if the tear seems repairable.
Good Luck