
 A recent article in the New England Journal of Medicine has attracted a lot of attention… and it should. The article focused on a group of patients with meniscus tears and osteoarthritis. The goal of the study was to determine whether or not surgery was necessary when compared to a group of patients who only had physical therapy. Although it was not the best study possible, the results are encouraging…. depending on your perspective :-) Physical therapy is equally effective at treating patients with both meniscus tears and osteoarthritis as surgery is. Imagine that!
A recent article in the New England Journal of Medicine has attracted a lot of attention… and it should. The article focused on a group of patients with meniscus tears and osteoarthritis. The goal of the study was to determine whether or not surgery was necessary when compared to a group of patients who only had physical therapy. Although it was not the best study possible, the results are encouraging…. depending on your perspective :-) Physical therapy is equally effective at treating patients with both meniscus tears and osteoarthritis as surgery is. Imagine that!
The issues, however, run deeper than those studied by the authors. Those issues include:
- Why were the MRIs performed in the first place?
- Why is it easier to get permission for an MRI and surgery than it is to get permission for physical therapy?
- Kudos to Dr Jen Gunter for her thoughts on this!
- Why do many patients expect an MRI for every joint ache or pain?
- Why do providers agree to order that MRI?
- Are we treating MRI findings— or are we treating patients?
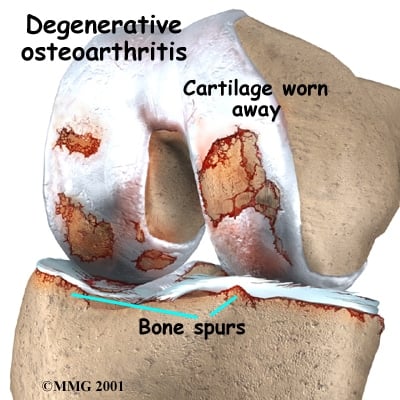
 A meniscus is a cushioning disc found within our knee. We actually have two menisci. Osteoarthritis involves the loss of “articular” cartilage from the ends of our bones. As that cartilage erodes away our bones become exposed, and when the bones on opposing sides of the joint rub together… it hurts — occasionally it hurts A LOT.
A meniscus is a cushioning disc found within our knee. We actually have two menisci. Osteoarthritis involves the loss of “articular” cartilage from the ends of our bones. As that cartilage erodes away our bones become exposed, and when the bones on opposing sides of the joint rub together… it hurts — occasionally it hurts A LOT.
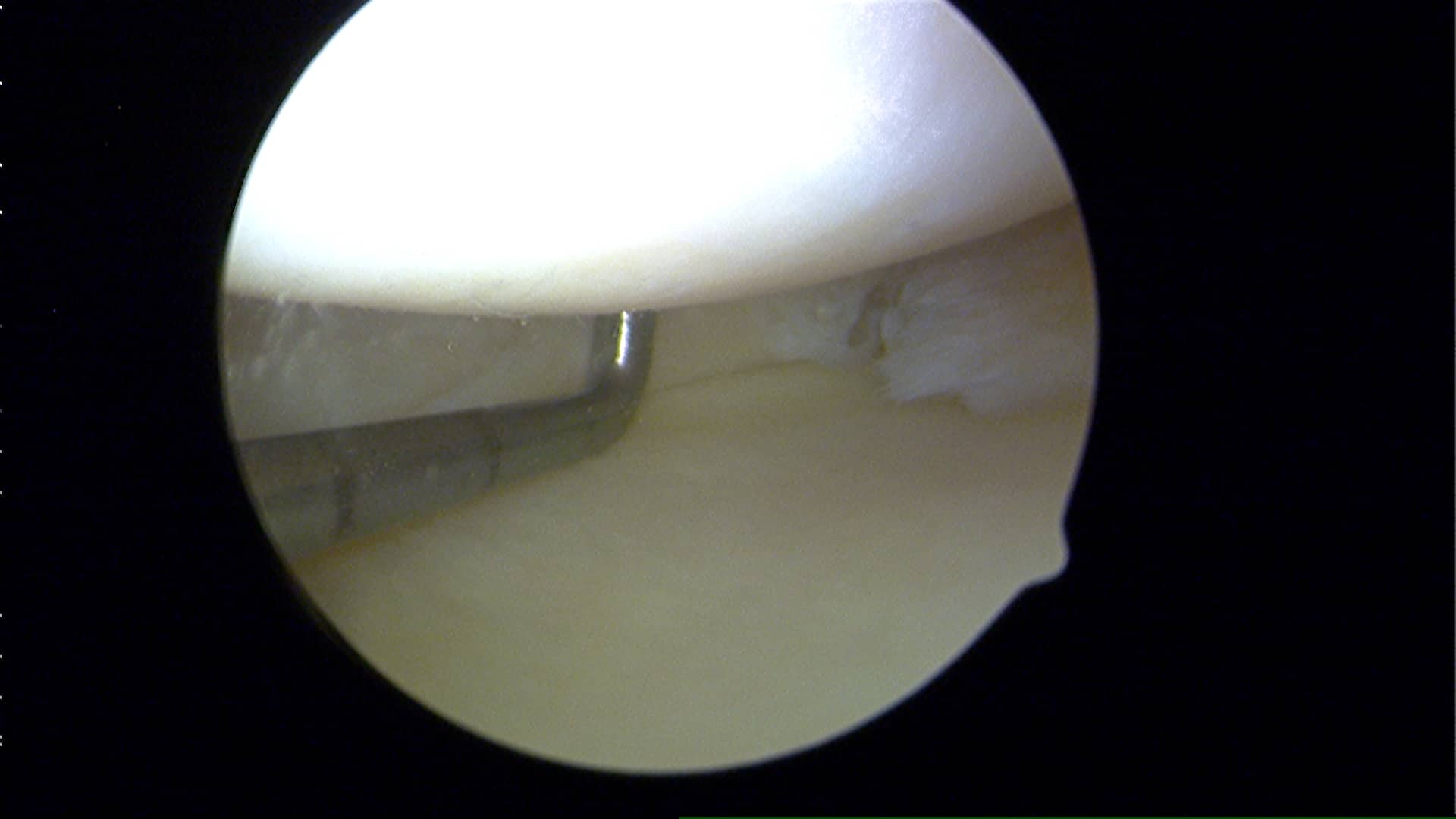
What most people in their 40s and up do not realize is that many of you have meniscus tears, and perhaps even a rotator cuff tear and yet you have no pain. Which meniscus tears hurt and why is an area we’re still studying. There are many different types of meniscus tears. Most tears are degenerative because our parts wear out… and surgery for degenerative tears without loose flaps is very rarely necessary.
If you sustain an injury and your knee hurts… you stand a really good chance of feeling better if you allow the body to heal itself. On occasion we need some assistance and that might mean a visit to your primary care doctor. Hopefully your provider can offer you some tips to set you on the path to recovery… but very rarely should an MRI be ordered (or asked for) soon after the initial injury. MRI’s should be used to confirm diagnoses… not to make a diagnosis. They are most useful if you have failed non-surgical treatment and we are considering surgery. Even in the realm of professional athlete injury management the issue of over-utilization of MRIs has gained a lot of attention .
Given the insight gleaned from this paper, your primary care doctor should likely start you in physical therapy if they suspect that you have suffered a meniscus tear, and your X-rays show evidence of arthritis. But our primary care docs are getting squeezed… they need to see too many people each and every day just to be able to keep their doors open. That leads to rushed visits, easy scripts for MRIs and premature referrals to specialists. That opens the door for a specialist to then recommend an operation based on the MRI findings… and not necessarily because they are treating you as a patient. Many variables need to be considered whenever surgery is being thought of as the primary treatment modality. Your MRI finding is but one small consideration in that “shared decision making process“.
The big picture… many patients will have meniscus tears that will marginally affect their quality of life, if at all. Not all weekend injuries require an MRI … time heals most injuries alone. Surgery is not necessary for all meniscus tears. Doctors need to commit to be willing to spend as much time talking about the non-surgical treatments for meniscus tears as they do trying to explain what the surgery entails. While surgery might ultimately prove to be the proper course of treatment to pursue for certain meniscus tear… it should only follow a course of failed non-surgical treatments for your meniscus tear and osteoarthritis.
Questions? Why don’t you come in and discuss your options. :-)










Nice article!! I see this things a lot in my chiropractic practice!!!
Thanks for stopping by Fabio. I have this discussion 20 times a week. Glad to see there’s evidence coming out in support of non-operative care for meniscus tears in the setting of concomitant osteoarthritis.
Dr Luks
I have been watching some of your videos online about meniscus tears.
I was recently diagnosed with a meniscus tear (using MRI). I have RA and not osteoarthritis. I am 44 yrs old. My knee filled with fluid and my doctor extracted it twice over 2 weeks. The third time he recommended and MRI. I do not have pain in the knee but there is some fluid. I also take pain meds for RA so I am not sure if that suppresses the knee pain.
My report reads as -” Posterior horn medial meniscal tear, small joint effusion. There is a vertically oriented signal in the posterior horn of the medial meniscus communicating with the tibial and femoral articular surface. No displaced meniscal tissue is present. There is mild thinning of the articular cartilage of the medial compartment without focal chondral defect or osteochondral lesion. the medial collateral ligament is intact. The lateral meniscus is intact. Mild Marginal spurring of the lateral femoral condyle is present”
I am wearing a knee brace to avoid surgery immediately. I am avoiding any activity that will put stress on the knee. Will I be a candidate for arthroscopy?. It has been about a week with the brace. How long should I wait before deciding on a surgery or get the fluid extracted again? Is it any different if I have RA and not osteoarthritis?
Thanks for reading and your time.
I am happy to read this article, I was just told that I have meniscus tears and arthritis on both knees and the first course of action was surgery.
I declined and asked that to be the last resort. This article makes me feel comfortable with that decision.
Thanks
Dr Howard,
I have just seen my surgeon (1 month) post op after acl and meniscus tear injury.
He reconstructed my ACL (I am 43) and left untouched 2 small tears of the lateral meniscus and one 1.2 cm tear of the medial meniscus. My question is how would the lateral tear affect me (arthritis wise in the future . Are they likely to increase even so they appear to be really small ?)
Also how significant is a 1.2 cm medial meniscus tear left unrepaired ? My surgeon mentioned that I might need surgery to repair it in the future as it might get bigger.
At the moment I would say this tear is slightly symptomatic but not much. My physio said that as part of my rehab I will do some cycling which is likely to smooth the edge of the tear and make it none symptomatic. Is that correct ?
Also with a large medial meniscus tear is that likely to affect how my meniscus work and created OA in the near future ?
Some tears we know if left alone will heal or likely not bother you. Some tears we need to treat. That’s a judgement call at the time of surgery.
Good Luck
Thanks. Howard for your reply. How do you base your decision at surgery time ? For example before surgery I thought I didn’t have any symptoms as I was walking in straight line. Now I am for example crossing my legs and can feel some pain on the inside of the knee ( I assume this could be my medial meniscus tear). I am a bit paranoid about getting OA as I am only 43 and active. My surgeon also said that at my age a suture was probably not going to work as I am too old. Is it not worthwhile trying or is it doomed to fail anyway. My thought behind this is if it works then I have a fully functional medial meniscus instead .
What are the risks of leaving a large tear in situ ? Is it still better than doing a partial menisectomy ?
I am reading that the progronosis of getting OA after knee reconstruction and partial menisectomy is very high but if the meniscus is intact then it is not much better.
In the case of an ACL tear and meniscus tear . During knee reconstruction how do you know which meniscus tears if there are more than one are degenerative and or acute ? Is that only based on the symptoms given by the patient ? What happens if the patient is not clear about the symptoms based on the fact that there is a lot going on in the knee after an acl tear.
Great question… At the time of surgery we are able to tell. We assess the quality of the meniscus itself (soft or firm: frayed or a clear tear), the location of the tear, the type of tear and can determine if it is repairable or not. A lot of attention recently has been focused on fixing tears we once believed would not heal — such as horizontal cleavage tears.