
Considering knee replacement surgery is a tough decision to make. Prior to taking the leap, many will try all reasonable alternatives to knee surgery before scheduling. Knee replacement surgery is a very commonly performed procedure that involves the resurfacing of the bones of the knee with metal and plastic pieces or components. While there is a wealth of information and advertisements recommending which knee replacement to have, and where to have it done, there is very little published about knee replacement surgery alternatives.
The most common condition leading to a knee replacement is Osteoarthritis. Osteoarthritis affects nearly everyone over the age of 60, yet it can also affect those of us in our 30’s or 40’s if we have a genetic predisposition or if we had a previous injury.
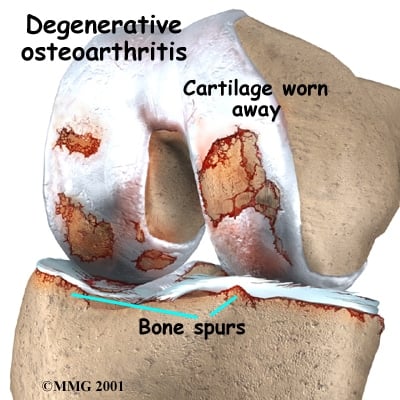
Osteoarthritis, by definition means that the cartilage cushion on the ends of your bones is wearing away. While there is no cure for osteoarthritis, the are many alternatives to surgery available to treat the pain associated with osteoarthritis and thus postpone the need for a knee replacement.
Why postpone a knee replacement? Well, a knee replacement is a big procedure involving numerous risks and a significant recovery period. Some of the risks associated with a knee replacement include:
- Infections
- stiffness
- blood clots, heart attacks and death
- loosening of the pieces or components
- instability of loose feeling in the knee
- injuries to blood vessels or nerves
- risks of anesthesia
Now, if your pain doesn’t improve with physical therapy, a knee compression sleeve, and certain supplements, then, in the right setting and after the failure of non-surgical treatments a knee replacement might prove to be your best option. But you may have a few years left with your knee, and since a knee replacement only lasts so long, the longer you have your own knee, the better the chances are that you will only need one knee replacement in your lifetime.
Related post: Should I have a knee replacement?
Knee replacement surgery alternatives:
There are many well proven alternatives to knee replacement surgery. Some are simple, some are more complex or invasive.
There is a body of literature that supports the use of various supplements and vitamins to potentially slow the progress of arthritis and diminish the inflammation. Some of those which have been studied include
- Chondroitin Sulfate
- Vitamin D : Not useful alone
- Curcumin
- Omega fatty acids
- minimizing sugar intake can decrease total body inflammation
The anti-inflammatories also have a role if you are able to take them.
- Ibuprofen
- Naprosyn
- Celebrex
- Meloxicam and others.
These medications can interfere with other medications like Plavix and Coumadin, and they can cause ulcers and kidney disease so be sure to check with your family doctor first.
Braces or Compression Sleeves: Compression sleeves can be effective in treating the pain associated with arthritis too. Simple neoprene sleeves will significantly improve the pain in many patients. It probably works through a biofeedback neurological mechanism, so if it’s tight enough to stay on, it is the proper size. Do not get a brace that is too tight. In this post I review the compression sleeves I see most often. Other braces that need to be ordered through your doctor can “unload” or take the pressure off side of your knee and transfer the stress to the other side of the knee. Since arthritis tends to begin on one side of the knee these braces can be very effective too.
Physical activity and physical therapy can be effective as an alternative to knee replacement surgery. In general, arthritic joints like to move. Activities such as rowing, walking, swimming or riding a bike are better tolerated. The stronger the leg muscles are, the less discomfort you tend to have. For those who have access to a pool… pool based exercises can be very beneficial for arthritis sufferers. Arthritic knees actually like to move… they become very stiff and painful from inactivity. Do I need to remind of that severe pain and stiffness is in the morning? ;-(
Ice can help alleviate the pain after a day of activity. Compression ice wraps can be used 15 minutes on, 15 minutes off to minimize the risk of frostbite.
Warm compresses to stimulate bloodflow to the knee can help, particularly towards the end of the day, or even early in the morning to help loosen up the joint before the day begins. Warm compresses can be used a few times a day.
Weight loss: For every pound you weigh, you put four to seven times that amount of weight across the knee on each step. So if you weigh 300 pounds, your knee is subject to 1200 lbs of force with each and every step. Therefore, even a small amount of weight loss can lead to significant improvement in pain.
A cane… yes, a cane. Get over it :-) ! They work. Use the cane in the opposite hand. o if your right knee hurts, use the cane in your left hand.
Injections as an alternative to knee replacement surgery.
If you have tried oral medications, braces, and exercise – and yet you are still suffering, there are a number of injections available to significantly ease the pain you are suffering from.
Do you have questions regarding an Orthopedic injury or longevity?
Do you want to talk to an expert who can listen to you for 45-60 minutes and explain the options in detail?
Dr. Howard Luks offers remote guidance sessions to review your X-ray or MRI images and explain your options.
Dr. Luks has also received hundreds of requests for educational sessions on the topics discussed in his book, Longevity Simplified.
There are many different types of medications or substances available for injection.
The workhorse of the injections is cortisone. This is a steroid and can not be injected too often, but it can make a warm, swollen, painful arthritic joint very comfortable in a very short period of time. There are risks associated with steroids, especially in diabetics where it will cause a rise in your blood sugars. While steroids are useful for acutely painful arthritic knees and people who are truly miserable, there are other injections you should consider either instead of, or after the steroid cools down your knee a bit.
Gel injections… or Viscosupplementaion involves the injection of Hyaluronic Acid (HA) into the knee joint. HA is a substance found in abundance in normal knees, and for some reason arthritic knees stop producing as much. These injections involve putting the Hyaluronic Acid back into your knee over a period of 3-5 weeks. This is generally a very well tolerated injection and can result in relief of your pain for anywhere from 4-12 months. No, it will not work on everyone… but most people respond very well. Many companies manufacture HA and the name brands include Synvisc, Orthovisc, Supartz and Eufflexa.
Platlet rich plasma, or PRP, which involves the injection of a portion of your own blood into your knee has been scientifically proven to reduce the pain from osteoarthritis for up to one year or more. In the end… PRP and stem cell injections may prove to be the best alternative to knee replacement surgery… but the jury is still out. One important caveat… Most insurance plans do not cover PRP injections. It truly is the wild west out there with regards to pricing and preparation. The research about PRP continues to the this day… we are still unsure of the exact reason why it works and the best way to prepare it… but the currently available methods seem to work well. I have called many offices in my area and found that the price for a PRP injection into a knee can vary from $1000-$5000 – so please shop around and do not be afraid to negotiate.
Please note… an arthroscopy, or scope should not be considered a viable alternative to a knee replacement. Having a surgeon go in and “clean things up” is not generally very effective.
Ultimately, you may go on to require a knee replacement. Keep in mind, it should be YOUR decision when that moment should arise. This is a quality of life procedure and only you can determine if you are ready, and if you have suffered enough. Luckily, there are knee replacement surgery alternatives that can work to improve your pain, improve your quality of life and potentially hold off a knee replacement for years.






Barbara Lefleur
I have severe OAin my knee with bone on bone. I’ve had 3 shots of cortisone . First one lasted 1 year , second one 5 months and it is now 6 weeks since the last. When I went in for the last shot,as with the others, I was in agony for weeks. Couldn’t sleep , couldn’t bend my knee at all therefore had difficulty dressing and bathing,couldn’t sit as when I did I-had great difficulty getting up and walking.I took Ibuprofen almost around the clock . Stairs were impossible. At last visit I scheduled surgery . I am now still in the “honeymoon”phase with only occasional pain, very brief but severe at the time. I Don’t want to go back to the severe pain. I am 75 and a tennis player. I was unable to play prior to the shots.Advise?
HI Barbara… If you have severe pain that significantly impacts upon your quality of life, and it doesn’t improve over the long term with PT, injections, etc then discussing surgical alternatives presents itself as a reasonable option. Keep in mind…the research shows that you need to wait at least three months after your last injection before having surgery to minimize the risk of infection.
Alicia
Had meniscus surgery on right knee about7 yrs ago. Did fine for about 6 yrs. In last year discomfort going down and recently up stairs. Also increasing stiffness after sitting. Last week knee popped out whengetting off couch. Extreme pain but didnt fall. Dont usually have much pain and even after that was minimal pain in a few days. Saw ortho docto yesterday and said i was bone on bone and recommended TNR. Have big trip(long flight) coming up end of July this year and I am concerned wont be healed enough Thinking of waiting till i come back in sept. But i am also concerned this might get real bad before or during trip ???
A knee replacement is an elective surgery… and it is performed for issues relating to your quality of life. It is not the surgeon who determines when you need a knee replacement, it is you who determines when you need a knee replacement. Most patients wait until the pain in their knee is affecting their quality of life so much that they want to move forward with the surgery. Often times these “exacerbations” settle down after a few weeks. Many patients, even those with bone on bone arthritis will respond to wearing a compression sleeve and physical therapy to keep the leg strong.
Good luck to you !
Joy Parrish
Hi there, thank you for your time to share your knowledge! I am 60, looking at bilateral tkr, I don’t have a lot of pain, but my knees are bone on bone and feel unstable or loose if you will. I get a klunking sensation through my entire body at times when I walk. Not clicking. Much stiffness. Would like to delay surgery but am I causing further damage by doing so?
the arthritis will continue to progress… but that’s not the reason to have surgery. This is a quality of life procedure. It is your decision as to when the surgery should take place. There are plenty of people walking around with bone on bone knee arthritis who do not need surgery. This is not an easy decision to make…
good Luck
Jeanie Thor
My mother is 96 years old and her knees are now totally bone on bone and it takes both my husband and I to get her up to even get to a bedside commode. Needless to say, I am not getting much sleep, as I have to sleep in her room and wake my husband to help every time she needs to get up. She can only lie down for a few minutes before she sits up with her legs on the floor, whimpering in pain. Her family physician says it is arthritis and bone on bone and that he does not think shots will help. He has just put her on pain patches and pain pills. My question is whether it would help the pain of getting up and back to bed and maybe even walking, if she had a knee brace? She does have a pacemaker, but other than that she is in good health and it is so sad that she must just sit on the side of the bed in her room for the rest of her life.
Hi Jeanie…
A compression sleeve might help a little. Not sure whether the “gel” shots would help her. It sounds aggressive but we have replaced the knees of 90+ year olds with good results. Sure the risks are higher… but it is a quality of life decision.
Sally
My right knee, too, is bone on bone. I was scheduled a couple of years ago for a total knee replacement and had to cancel because of family obligations that came up. Have been putting it off since. I am on my feet 5 to 6 hours a day working and 70 years old. Should I consider microfracture surgery before total replacement?
Probably not… but I can’t give a formal recommendation unless I see you in the office.
Helen yettaw
I am not a patient of Dr luks…but I am a patient of a good orthopedic doctor in Tampa, Fl. I elected to go the brace route…I am wearing two offloading braces….I am so happy and totally pain free…even my night pain that was at one time was so bad is no longer there….Helen Yettaw
Elisha Dellios
Dear Dr. Luks,
Thank you so VERY much for offering a comprehensive, clear and thoroughly helpful explanation of the alternatives to knee replacement surgery. My mother is considering the surgery, and I, like any daughter would, want to be able to help her make a wise and informed decision for her best well-being.
Thanks to intelligent, well-educated people like you, who are generously sharing their knowledge, we will make those better choices! I wish all the best to you and yours. Thank you! Elisha
Lee Lord
My right knee is bone on bone”. I had a shot 3 months ago and no pain right now. I want to know if I’m damaging anything by holding off? I’m 70 yrs old.
Not necessarily. Many people with severe arthritis are walking around without much discomfort and able to put off surgery for now. Each case is different… so a good exam and a sit down and deep discussion with your surgeon is needed.
david london
Teriffic site. Having knee replacement next month myself (82)
Back on the links by next Jan. Roll on 2017
David (UK)
Michelle
Hello Doctor,
I’m a 43 yr old woman that had a knee give out while walking and could’t put weight on it (right knee dropped out while walking but didn’t fall) 4 months ago. Had an MRI and the results say I have a “partial tear of the anterior root attachment of the medial meniscus with medial extrusion of the medial meniscus. Deep fissuring of the cartilage in the medial tibiofemoral joint compartment with subchondral marrow edema and small marginal osteophytes. Deep fissuring of the cartilage with delamination and patellofemoral joint compartment.” The doctor said I also have “advanced arthritis” and a standing x’ray showed joint narrowing only on the medial side of my right knee. I believe the arthritis is from when I tripped & fell on both knees on the sidewalk about 6 years ago. They just felt really bruised inside and eventually it went away. I just finished 3 Synvisc shots about 3 weeks ago that didn’t provide any relief. I get this weird bone snap feeling in the inside front corner of my knee sometimes. I don’t know if that’s a bone hitting bone on the medial side or if it’s from the partial meniscus tear. I would love your opinion and perspective on advice. Do you think arthroscopic knee surgery would help? Thank you!
Robert N
I am 70 years old and have bone on bone bilateral knees. In 9/15 I had triple bypass surgery followed by a watershed stroke. I would like to know about alternative treatments since I am high risk for surgical procedures.
Penny
Hello,I have both knees with osteoarthritis and both are bone on bone with meniscus tears(was dx with right tear in 2007) I just had a Mari on the left and it is most likely the same issue with my left knee, the orthopedic dr that I saw said I need scopes on both knees to clean them out and I need to work with him to lose 20 lbs and he can buy me some time because I am only 54 and I am way too young for knee replacement…I am concerned about anesthesia and my asthma and also if this will even make me feel better or improve that I can walk again,I have lost 8 lbs so far but can’t exercise because of the instability. I would appreciate your thoughts…Thank you so much
Arthroscopy in the setting of bone on bone arthritis is usually not effective. Losing weight can produce significant improvements in knee pain due to OA. 54 is not too young for a knee replacement … but that doesn’t mean you should have one. Injections, certain braces or compression sleeves, PT, weight loss etc are all useful alternatives. Arthroscopy is not considered a useful alternative in managing the pain of severe arthritis.
Gloria
Is it ok to keep going with knees bone on bone. Does it cause more damage to the bones. Are the bones being wore away as rubbing together. Does the pain come and go as at this moment not a lot of pain. Also what is meant that “you can burn past the pain” mean. Thank you
Usually not Gloria.. there are certain bone loss patterns that bother us as surgeons, but in the vast majority of cases such as yours there is little risk in carrying on until you deem it’s necessary to proceed with surgery.
J. Bynum
Does scar tissue from a knee surgery performed over 40 years ago create complications in a total knee replacement that I am scheduled to have next week? I have read that people with limited range of motion because of older surgeries will have more difficulty with physical therapy and that the knee may not bend as much as it did prior to TKR. I am 55 years old and the pain in my knee decreases the quality of my life, i.e., I cannot hike, kayak, walk any distance without swelling and pain afterward. I just don’t want to have more pain and less range of motion than I do now after having the TKR. Please advise.
It can have an effect. Your range of motion going into a knee replacement is predictive of your ROM when you are all finished with your recovery. Now, is it possible that you can work hard and push hard and potentially increase your motion further, sure… but research is based on statistics — so your motion might be limited after surgery.
Barbara Hale
Doctor, Could you tell me if you know anything about the injections to the knee that are referred to as doner injections. Nutrient rich amniotic tissue from healthy donors of their placenta after delivery . I am a 79 year old lady who is active and have worn my knees out. This has been mentioned to me as I fear knee surgery. Thank you,BH
I can’t… I know of them… but I have not seen any relevant research on them
Rachek
I have a question about braces. What in the hell kind of alternative is that? Walking around with a brace for the rest of your life is highly unrealistic and uncomfortable not to mention that it looks awful. How do you wear it? Over, under clothes? I had a brace and it was uncomfortable and it was a nuisance and i limped along and was embarrassed to be seen.I didn’t want to live that way. No one wants surgery but friends of mine have had knee replacement and walk around normally without a cane or a brace.a brace is a horrible alternative unless u want to drag your leg and limp around, not my idea of life.
Rachek … After practicing for nearly 18 years I find it very interesting to see what people will choose to do to avoid surgery. Some have no choice and failed all options. They happily or reluctantly proceed with surgery. But no surgery is without risks and many knee replacement patients regret having surgery. In addition, the thought of surgery is simply too much for some to contemplate and they will try every last possibility before even entertaining the thought of entering an operating room. Others might choose to have their surgery sooner rather than later and “move on”. This is a very personal decision for each patient. That’s why I shared the options that many patients consider… and often tell us that they have had success with. Sleeves of the tommie copper variety seem to be most common and best tolerated. They are also less cumbersome and bulky and for many they are quite effective. Your point is well taken, and common among many from within our younger patient base.
RAGeorgeadis
Hi Dr. Luke
I had a total knee replacement 2 years ago with little improvement. I have a lot of numbness at the lateral side of the knee that radiates down the leg
My surgeon is recommending arthroscopic in that knee replacement. Is this normally done and what risks are involved.
thank you for your I formative column.
Numbness on the outer side of the knee after a knee replacement is normal. Numbness on the outer side of the lower leg could be an issue with the peroneal nerve … or the low back. Unlikely that an arthroscopy will help address numbness. Pain — perhaps, but without examining you I can not comment further on treatments in this forum.
Robin Denise Wormsley
I have a question about Knee replacement vs microfracture repair. I injured my knee at age 57 , after physical therapy attempts fail to relieve pain, I was told I was going to have my knee scoped to fix a possible tear. I had this procedure at age 58. I woke up to being told I had a microfracture procedure. I was not even told about this prior to the surgery . I had never heard of it before and it was never discussed. My husband was told I would need a total knee replacement. My question is this what is the success rate of this microfracture procedure for patients in their late 50’s early 60’s . Is it better to do the replacement?
It’s not very effective at our age… especially if the loss of cartilage is extensive. Whether a knee replacement is needed is more of a quality of life decision. It can’t be done for at least 3 months after your surgery or last injection anyway… higher risk of infection.
Anne Summer
Thank you for responding to so many individual requests regarding our diseased knees! Last year, at age 56, after about 10 days of extreme stress, my right knee became incredibly painful – to the point of my not being able to stand. My ortho doctor said the long, banana-shaped swelling on the side of my right knee was a cyst that would return if drained, therefore, surgery was indicated.[Am also knock-kneed, with right leg becoming a “kickstand”] An MRI was done (torn meniscus?); I had knee surgery. After the procedure, the physician said that I didn’t have a cyst after all (it wasn’t there when I woke up and, he “had never been more suprised in the operating room by what he found- compared to what he thought he would find”). When I asked what he DID find, he said, “a synovial response, just like the MRI indicated”). This answer did not satisfy me.I believe the nurse said a meniscus repair was done. After 3 rounds (6 visits each) of PT, I stopped. While my knee pain was practicallly gone, the accompanying arch-of-foot pain, buttocks pain, and calf cramps remained. I went to another Ortho doc when the knee pain returned as well. He eliminated the spine as cause of my other symptoms, and has begun a series of cortisone injections about every 8 weeks. He says I am not bone-on-bone yet, but I am concerned about how much longer cortisone should be continued (the injections work, until they DON’T). He says to expect TKR within 2-3 years – shots for that long? Also, he says, “I did 5 knee replacemnts yesterday, I know what I’m doing”. This concerns me, as this feels like assembly-line surgery to me. DO I NEED TO LOOK FOR A THIRD ORTHO SPECIALIST? Am currently overweight, history of TIAs, seizure disorder under control with minimum meds. Otherwise, only 2 years ago, I was very active, including aerobic- and Zumba-dancing three times weekly. Not anymore.
Arthritic knees typically do not like being operated on. They are very “cranky”. A knee replacement will be necessary when you think it is necessary. Many of our patients have noted significant improvement in their pain with certain knee compression sleeves. In addition, many take Tart Cherry Juice
which is proven to work in many with arthritic knee pain.
Good Luck
Diane James
Hi I am 58 yrs old fit lady I have been told by my surgeon that I have no cartlige on the left side of my knee and very little on the left side, she says because of my job and the long hours I am standing on my legs I will now need a replacement knee. I have had three clean out and repairs done the last one I’m still recovering from, as I have to return to work soon as a chef could u please advise me as to which knee brace I should wear as mmy knee feels very unstable.
many of our patients like the Bauerfeind knee braces
Tanya
I’ve had multiple (17) surgeries from a compound fx of tibia/fib years ago. Osteomyelitis as a bonus. I’m 52 active but suffering from knee pain now. MRI shows all kinds of damage. My surgeon said he wants to do arthroscopic procedure to look closer. Said I’d need replacement but no one would want to touch it because of the osteomyelitis. I don’t like pain meds but can’t get relief otherwise. What do I do? .
It’s true that osteo in the past, carries a much higher risk of infection in a future knee replacement. There are ways to minimize the risk of infection, but you need to see a revision joint surgeon who has experience in this area. This is not a knee replacement for your average orthopedist to be doing.
Good Luck
scott
I have been diagnosed with a degenerative cartilage condition in my left knee. Is there any way to replace cartilage? I have heard of a gel that replaces the cartilage etc. if not what options are there.
Hi Scott …
There is a lot of misunderstanding about the various injections we can offer you. The “gel” injections do not restore the cartilage, nor reverse the arthritic process. They simply make the knee feel better in many — not all who have them.
PRP/Bone Marrow and stem cells. In this situation, the injections can slow the progress of arthritis, but injecting PRP or bone marrow will not reverse the arthritic process — Many people who have had PRP, etc injections feel better for many months after the injection… and again, some do not have any improvement.
Tee Young
I hsve a complicated bakers cst that ruptured causing massive leg swelling with mega pain.MRI shows osteoarthritis some meniscus tear and joint effusion 3 months ago I had no knee problem.is injection possible instead of knee replacement that was suggested
Colleen Ursi
My husband had the stem cells implant on his knee. He had the bone marrow taken from his hips and injected into his knee. He was in a car accident and tore the cartilage so they said he was a good candidate because it wasn’t wore out. He has less than 6% body fat so he is NOT over weight. He is very active but has problems with his knees going down stairs and running. He loves to run and wanted to run again. He had the stem cell procedure done July 20 2015 it cost $5,500 apx. He said he hasn’t seen much of an improvement he still cannot run and still has pain. When I ask him if there has been an improvement he never gives me a straight answer so I would say there is not. Although the Doctor said he could see improvement up to two years and it hasn’t been a year yet so we will see.
Rose
Hi Dr. Luks,
I had my left leg ACL & MCL repaired 12 years ago (turning 40 soon). I don’t remember what it was called but I do remember they used my hamstring to reconstruct the ligaments. The past few years I have noticed my left leg is considerably crooked giving that side a “knock kneed” look. Is there anything I can do to either correct it or stop it from happening? I’m very active and I feel as though it’s starting to slow me down – plus it just looks ridiculous. I’m also very concerned that it will affect my hips. Thank you in advance!
That is a very complex problem. In some cases we can/should and do correct it. In other cases (especially if severe arthritis is present) we can correct it.. but we shouldn’t— because we can correct it when a knee replacement is performed. So… bottom line- you need to find a sports doc who is willing to sit and work with you in determining the best course of treatment.
Gregory Dick
Dear Dr Luks.
After having my left knee scoped for meniscus tear in 2013, my MRI results indicate tears in my right knee, and as my orthopedic MD advised a TKR, I scheduled a bilateral for end of May next month. The cortisone shot giving the day of the MRI made me feel like a million bucks for about a month, now it is wearing off, and the pain, stiffness and inflamition is back. At 260#, I could stand to lose 50 #s, but exercising agrivates the knees and the catch 22 is a viscious cycle. Tack on 8 hours of standing on concrete daily and I hope you can feel my pain. I am really at odds – At 52 yrs old, I do not want to get into a sedatary weight gaining lifestyle, but I feel I am moving into the direction of TKR due to daily pain and stiffness. If I could eleviate the meniscus pain, and constant inflamation, I feel I could postpone surgery for a long while. I am taking Meloxicam, which helped at first, now not so much. Could you please advise – not looking forward to knee replacement surgery – pretty attached to the ones I have ;-( but need some type of relief soon
Sincerely Greg
Tough situation Greg. Most people with severe arthritis also have meniscus tears. Treating the tears has an equal chance of doing nothing or making you worse or making you a little better for a period of time. The decision making depends on how severe the arthritis is, what type of symptoms you have etc… that is all ways beyond the info I can provide you in this type of forum and requires and in person evaluation and exam.
Patty
Thank you for this info!
I had scope for meniscus tear at age 18 and ACL reconstruction at age 23, at whIch time I was told there was already arthritis starting. I’m now 50 with pretty significant osteoarthritis and bone spurs. My mom has had both knees replaced.
I wonder why with so many intricate and complex medical advances there hasn’t yet been developed a way to duplicate or replace cartilage (so people don’t need their knees replaced).
I’m holding out. :-)
Great question ..
Cartilage is a very difficult tissue to work with. Also, arthritis is multifactorial — it’s not just the loss of cartilage, the bones changes shape, bone spurs grow and the chemicals in the knee become hostile to cartilage survivability. So, there are many things that need to be addressed…. we will get there over time.. but not any time soon :-(
Jenny A
Hi Dr. Luks
I was a runner 20 years ago (hurdler in college = trama to same knee over and over). I’m 41 and have been diagnosed with advanced lateral patellofemoral osteoarthritis and small joint infusion (and a small cyst) via an MRI. I went to the hospital of special surgery and they recommended an arthroscopy, lateral release. The dr said I would be able to run again, 99% chance. My question is do you believe this is the best option given my diagnosis? I feel like it’s a temporary solution and could be accomplished with stretching and strengthening?
Hi Jenny ..
Sorry to say .. but a lateral release doesn’t have a very good track record — especially if the arthritic changes are advanced.
Ricky West
Dear Dr. Luks, First thank you very much for your online column. It is invaluable. To my question: I am a 57 year old with mild knee arthritis (more than 2 miles a day causes significant pain in evening) following a meniscectomy. Synvisc One did not provide much benefit. I can’t find any literature on whether it is worth trying again. I am also looking into PRP after reading your comments above. Kind regards, Ricky
Dick
I am 75. X rays have shown bone on bone for quite some time in both knees. I am somewhat bowlegged probably more so due to this condition. I ride a bicycle nearly 100 miles a week, with minimal pain. Getting up out of a chair or standing or walking for any length of time is painful. In reading all the above options the conformis knee solution looked the best for me. I live in Tucson AZ. Can you recommend anyone in this area or southern CA, or Phoenix, that does this procedure. I know without seeing my x rays you can’t know for sure but do you thing this procedure would work.
regards
DIck Walker
[email protected]
I happen to like the Conformis technology very much. You should consider calling the company to see if they have a surgeon in your area. Good Luck !
Mansukh Patel
I have OA in both knees, Left knee has more than right knee. No bone to bone yet. I read many articles on when TKR should be considered. There was a thirteen points/question to decide if TKR needed. My answer to 7 question was “yes”. I had a steroid injection in left knee, helped for three months. I was prescribed Meloxicam (Mobic) but did not use constantly (used only for a month) since I felt they may impact lever or kidney. With every day biking, my right knee does not feel pain during daytime because of mobility. I am scheduled to have both TKR in November 20, 2015
My left knee pain is reduced 80% when I apply pharmacy compound Diclofenac/Baclofen/Cyclbenzaprine/GA/Bapentin/Lidocaine (H) 35-2%-2%-6%-2%. All pharmacist told this is very good cream with very minimum side effects.
My concern is: (I am 62 years, 254 lbs, with past TIA (in 2009)
1) Is it always come backs to have both knee TKR even though one knee OA condition is better than another knee?
2)Exercise and reducing wait helps in reducing pain and may avoid TKR possibly two years for right knee. Eventually left knee will be bone to bone and later right knee. So is it advisable to delay surgery considering I will be more old with less physical strength to cope physical therapy?
3) My both legs are bowing and considering right knee is better is it advisable to do both knee replacement at same time or do only left knee replacement (in 2015) and right knee later in (2016 or 2017). I know/read risk verses benefits of two TKR verses one TKR. If I do it separately then I am thinking to do it in 2016 to pay only one deductible.
The person who decides when their quality of life is suffering enough that they want surgery is you. A bilateral knee in someone with TIA, possible cardiac disease, etc is riskier. More people die after a bilateral then after a staged procedure.
Tate Price
Hello Dr. Lurks,
I am 31 year old former professional athlete. Due to two terrible knee injuries in my left knee, I now have terrible degenerative arthritis in the lateral portion of my left knee. I am bone-on-bone with large bone spurs throughout the knee. I visited the Mayo Clinic and was told a TKR is inevitable and there is very little that can be done in the short term to help resolve the pain. I also visited Dr. Stone in San Fransisco and he recommended a Makoplasty partial knee resurfacing right away. I am curious about your experience with both Makoplasty replacements and non-surgical or minimally invasive surgical procedures to help with pain. What is the youngest patient on which you have used a partial knee replacement? Any insights as to the shelf-life of Makoplasty or Conformis? Other than that, what have you used in the past to help with somewhat severe OA pain?
Hi Tate…
Except to minimize pain there is no rush into performing a unicompartmental replacement. Mako, Conformis, etc… when well done, they all have the same lifespan. It’s very difficult to tell you how long it will last. Placing them into a 31 year old versus a 60 year old will lead to different issues. You will try to be far more active. So it may last 10 years, or 15 years … we simply do not know.
I perfer Conformis over Make simply because it preserves more bone and the implant is manufactured for you. A Mako uses an off the shelf component, and a semi-robot to burr the bone before putting in the implant. The conformis doesn’t require the same bone cuts and preparation.
A Vaughan
Hello. I am so at a loss. I was told I have arthritis in the center of my knee and the cartilage is gone in the center. My dr. recommends Microfracture surgery but I haven’t read any good reviews and those I know that have had this surgery said it didn’t help. Now my dr. said he will just scope the knee since I am against microfracture.I wanted a partial replacement but he said at my age, 44, he doesnt recommend it. What would you suggest or think? Thanks
FYI: MRI says full thickness chondral loss at medial femoral condyle and medial tibial plateau. Injury at medial meniscus, etc.
Very unlikely that an arthroscopy would be beneficial with bone on bone changes.
a partial might be an option, but without examining you or seeing your xrays I can not give you any medical advice.
Das fe Subhendu kumar
My wife have trouble both knees with O.A . please tell me why surgeon ask me , you should have 3 consecutive sterile urine before TKR is that really necessary?
thank you. waiting for early reply
That is a bit aggressive … women often have “colonization”. She can have bacteria but she can’t have an overwhelming infection.
Kay
In searching the net for alternatives to knee replacement, everything I am reading, I already know and am implementing. I had been doing fine for a couple of years, even not needing any injections. Then, I went to get in my car and just a small little twist resulted in me not being able to bear weight on one leg when I went to get out of the car 5 minutes later. That was about 6 weeks ago. Recent MRI shows my knee is bone on bone with severe arthritis, large Baker’s cyst, enchondroma, and of course the medial meniscal tear, but the pain seems to be from the meniscal tear mainly. My doctor says if I didn’t want the knee replacement they could go in and try to do somewhat with the meniscal tear but at this point I don’t know what to do. I take Ibuprofen every day, use ice, try to do exercises to strengthen my leg but the pain is still there. I was told it may never heal. I don’t want a knee replacement if there is any way possible I can do other things to avoid it but if this tear is not going to heal, what do I do. All these other chronic issues with this knee were there before the tear and I was doing okay, so this tear has caused everything in that knee to “wake up” with fluid, pain, swelling.
You can find me on Curely where I can answer questions by text or email … Join me there. http://www.curely.co/
CathyB
I had Symvisc 18 months ago and it helped enormously for 17 months. Had another last month. Have other medical problems and have lost 2.5 stone as a result. Seem to have more pain this time due to an injury to the knee but am still walking better than before the first injection.
Sharon harris
What are your thoughts on makoplasty
Hi Sharon… I am a very big fan of partial knee replacements in the right patient and in the proper setting. A makoplasty is just another way of doing a partial knee replacement. I find the custom partial knee replacement more interesting than Mako … look into the Conformis Knee solutions.
Bruce
My legs are becoming more and more bowed out…you could drive a herd of cattle through my legs…I have lost over an inch in height because of this. My knees are getting increasingly swollen and painful, my right more than my left. I’ve seen ortho surgeons in the past and was recommended TKR as long as 10 years ago. I have aortic stenosis and am probably 3 years away from valve replacement. My cardiologist says I should go for the knee replacement(s), my ortho surgeon says it’s up to me…(of course). I just can’t seem to find a time which is beneficial for my healing and therapy post op. I live in the midst of a state forest, hilly…and have massive gardens, orchards, etc…and…in northern Minnesota where I live, 6 months of the year there is snow and icy paths to our house.
Actually, I’m quite afraid of not surviving the surgery, even though my cardio and ortho doctors say no problem. Any advice???
Bruce… I have that conversation day in and day out… it’s a very hard decision to make. There is never a great time to have major surgery. This is a quality of life decision that only you can make. Good Luck to you my friend.
John
Dr. Luks,
You didn’t talk much about stem cell injections. Where are we at on that front? What does the data show?
You’re right John … Stem Cell therapy is in it’s infancy. Some doctors are performing it… but good clinical research is lacking. Large studies are always conflicting… one might show improvement in pain, and the next doesn’t . We think that stem cells hold significant promise, but it’s the wild west right now. I linked to an article recently about them on our Facebook Page @ Howard.Luks.MD
Marion
I have been told that I am bone on bone on both knees and that my only option is knee replacement.
When I wrote my doctor about alternatives he sId he does not want to disillusion me.
I have had the cortisone injections and they are not lasting more than a couple of weeks.
The last time the fluid from the injection got on a nerve and I was in severe pain with nothing bringing relief for hours.
I cannot afford the down time for replacement and I can’t bare the thought of the pain of replacement either.
I am looking at bone marrow from my pelvic mixed with my blood to form stem cells for injection.
Can this work or am I delusional?
Marion … It may give you relief for a little while, but it will not reverse your arthritis.
Howard Luks
rob n
Dr. Luks,
I have OA and pseudogout, and the crystals have formed in many joints including my knees. I’ve been told I need KNR in both knees, but was wondering if orthoscopic surgery could possibly clean up the debris in my knees and delay the major surgery.
Rob … without examining you and looking at your X-rays I can not comment on that… sorry.
Joseph Rock
Hi Dr.Luks. My knee specialist told me I need TKR and it is scheduled for Mar 4th. I when to my PCP to get the normal pre-op stuff done. He recommended Celexbrex to help with my pain and losing weight (270) between the medicine and losing 10lbs my knees feel much better. I plan on losing a lot more has I get more active.I’am very scared.do you think I could delay this awhile? Thank you Joseph Rock
Of course you can delay the surgery !! The surgery is done because you want it done… not because we tell you you need it done. 99% of the time this is a quality of life surgery and is offered to patients who fail to improve with medications, weight loss, exercise, bracing, injection and physical therapy.
Good Luck ! Congrats on the weight loss.
John Trebilcock
First visited Orthopaedic Surgeon 2002, and have returned twice, together with obtaining other opinions. I am now 80 years old, and having difficulty walking. First O.S. will not operate for knee reconstructions, because I had comprehensive open heart surgery 2010. He does not believe in Synvisc injections, so will be seeing another O.S. next week to determine alternatives. There is only minimal discomfort when resting, but significantly more when walking, particularly under load. I am still playing golf twice a week with the help of a golf cart, but can only walk slowly from cart to ball using golf stick as a walking stick. I am buggered after 18 holes, but it beats sitting around feeling sorry for myself. If surgery is virtually mandatory, is it feasible to have an Epidural instead of full Anaesthetic, and would it be wise to have both knees done at the same time? Also should I continue to pursue Synvisc injections as a viable alternative?. The unbalanced walking is affecting the calf muscles in each leg, and the hamstring in my right leg, so my lower body is showing it’s age, but by brain and upper body are still in middle age
Your independent assessment would be appreciated.
Sincerely,
John Trebilcock, FINNISS, S.A.
Hi John … It is up to your cardiologist to determine whether or not your heart is healthy enough to undergo surgery. Many patients who we operate on have significant cardiac disease — yes, it elevates the risks associated with surgery, but it is rarely an absolute contra-indication. Many patients feel that Synvisc helps them. But this might be simply due to a placebo effect since almost all the well performed studies show no benefit of the Synvisc above and beyond the benefit of simple saline injections(control).
Having both knee performed at the same sitting might be too risky in you… again, something to review with your cardiologist.
Good Luck
Howard Luks
Rob Bruce
Thank for all that accurate advice,I was hoping that I could have a half knee replacement, so that I could keep surfing. But have had surgeons recommend I take pain killers and finally have total knee replacement.i am nearly ready for t k r now but still hoping for a miracle.cheers rob
Charles Howard
Exactly the same info I got from my M.D. ; thanks
Neil O'Connor
Good unbiased advice…on my way to needing something done with my stiffening knees but baulk at the idea of replacements just yet