
…and we should NOT think like mechanics.
Orthopedists and Twitter
Thanks to an orthopedic colleague, Dr. Katherine Burns, the Orthopedic community and any other interested parties on twitter were given a chance to observe for the first a well done live tweeting of an orthopedic meeting — focusing predominantly on the shoulder. Now, those of you have been around twitter for a long time, and certainly those of you who attended many healthcare meetings, and certainly healthcare marketing meetings clearly know that live tweeting of events is nothing new, however, from an orthopedic perspective — this was a big leap forward.
We are not mechanics… We treat patients, not MRI findings
The one upsetting issue is a theme that I see repeated over and over in the realm of orthopedic surgery, both in resident education, in what many people are told in offices around the world, as well as the focus of much of the literature that I read in the realm of shoulder surgery. That is the issue of *Mechanical Thinking*. Something is broken or torn so I must fix it!
A not insignificant focus withing the orthopedic literature — and certainly most of this meeting which was live tweeted focused on how to fix something, what techniques could be utilized to fix something, and what the overall results were from utilizing those techniques. The didactic sessions were followed by a laboratory session where the surgeon attendees were actually able to perform the surgery on cadavers in order to hone their skills. That’s all well and good. HOWEVER, this assumes that surgery was *necessary* or advisable in the first place. There was very little discussion centered about who needs surgery, when they need surgery, or why they need surgery.
A Patient Centric Approach
I received many questions through my website and certainly in my office in the form of second opinions where people put forth the issue that surgery was being recommended to repair a rotator cuff tear – – – yet they had relatively little if any discomfort. Many people offered that their pain was having little if any effect on their quality of life … and important Shared Decision Making principle. These were typically situations where they most likely had shoulder pain for a short period of time and were referred for an MRI (perhaps a little early), a rotator cuff tear was identified and purely mechanical thinking led to the recommendation for surgery. Since the recommendation, most of the patients who presented had already realized significant improvement in their pain and they were wondering whether surgery was indicated.
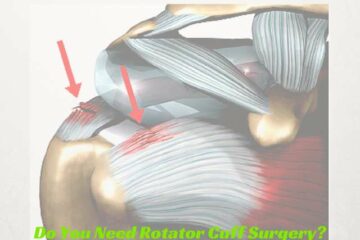
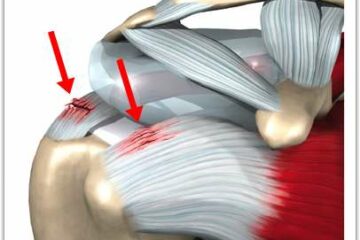
Orthopedic surgeons have been taught in the past that most tears *need* to be fixed. Again, mechanical thinking – – – if something is broken, we must fix it. We now know that this is probably not true. Why don’t I use the word probably? I use the word probably simply because we don’t have enough evidence to say with absolute certainty what tears need to be fixed and which tears do not need to be fixed. Very few surgeons would argue that acute or posttraumatic tears of the rotator cuff truly deserve to be fixed. However, many tears, or in fact most tears of the rotator cuff are attritional in nature — this is where the tissue simply wore out. The analogy that I frequently use is — your favorite pair of blue jeans you’ve been wearing for years. You look down one day or you feel a breeze around your knee and you look down and there is a hole in the front of your bluejeans. Did you rip it purposefully, did you lean on it or kneel on it or inflict some form of trauma to your pants :-) ? No, the tissue, or in this case the fabric simply wore out. So if that tissue is wearing out and we choose to repair it what’s the likelihood that the tissue has the ability to heal? If it is *successfully* repaired – – – because the tissue is degenerative, what’s to prevent it from simply tearing again? Once again, we simply do not have good answers to those questions.
Do I *need* surgery?
The same issue came up with labral tears. There was a lot of discussion about techniques to be utilized to fix labral tears, what techniques should be utilized in various age groups, etc. The number one number question in my mind, however, was not well addressed. That question of course is — “Do labral tears need to be fixed?” In many situations the answer is clearly yes. If your shoulder is unstable or dislocating then you need to have your labor repaired to minimize the risk of re-dislocation. If you are an overhead athlete and you sustain a labral tear, do you need to have that repaired? Occasionally the answer is yes. Unfortunately, some recent literature has shown that the vast majority of high-performance overhead athletes are not able to return to their prior level of function following a labral repair. Are surgeons informing these overhead athletes about these facts? There are many surgical success stories where we are clearly able to return a high-performance athletes back to their usual function. But it does not appear that labral surgery in this unique patient population is often successful … in weekend warriors and many high school or college players, a repair appears to be successful. But the margin for success is not high.
So, by and large this was a good week for the world of Orthopedics and Social Media. There are many more orthopedic surgeons on Twitter and other social media properties. This will ultimately prove to be a *good thing* for people searching for quality orthopedic information.
Eminence vs Evidence Based Medicine and Surgical Decision Making
On the flip side .. due to the persistence of Eminence Based Medicine in the community and the issue of purely mechanical thinking — I simply suggest that you temper your decision to proceed with a recommended surgery until you obtain a very clear understanding and an adequate discussion about the evidence that exists as to why the suggestion for shoulder surgery is being made — prior to you considering surgery. Have a clear understanding of what shared decision-making principles are. Perhaps even utilize the multitude of shared decision-making tools which are available to you on the Internet. If your surgeon is either not willing or capable of discussing the evidence or going through a shared decision making process with you — consider a second opinion— or moving on.










Dr. Luks,
I’m a 55 yr old healthy male and former high school athlete. My MRI results show a full-thickness insertional supraspinatus tendon tear with less than 1 cm retraction and also a type II SLAP tear. The original acute injury likely occurred 30 years ago in college when I separated my shoulder in an intramural softball collision. I have five sons who have all played baseball, so I’ve done A LOT of overhead throwing and pitching batting practice my entire life. I aggravated my shoulder again last fall throwing way too much batting practice one day, and my shoulder pain will not go away as it had in the past when it got sore. I hope to continue doing a little throwing and also want to be able to play golf more as I get older. My shoulder pain is starting to wake me some at night and causing me to lose some sleep.
Based on all of the above information, would you recommend surgery?
Not necessarily … certainly not on the SLAP lesion.. those almost never need surgery in adults.
A degenerative rotator cuff tear is usually treated with therapy. Surgery is considered if PT doesn’t help minimize the pain and maximize function
My orthopedic surgeon insisted I do PT for 4-6 weeks. It helped a little. He then gave me a steroid injection. It didn’t help at all. That’s when he said an MRI would be a reasonable thing to do.The surgeon indicated the risk of not having it done is that it could eventually result in the need for a shoulder joint replacement. He said he could “trim” up the SLAP lesion while in repairing the rotator cuff tear.
I have a near full thickness tear of my subscapularus and a complex tear of my labrum. Can these issues be fixed at the same time during the same surgery?
Yes.. they can be. But, we often do not need to fix the labrum. The decision to fix the labrum depends on your age, injury, exam, etc.
Dr. Luks,
I am a healthy 74 year old male. Surgery has been highly recommended for the following:
Subacute full-thickness tear of the subscapularis tendon with partial retraction. Localized edema of the muscle belly and minimal fatty infiltration. Low-grade, probably chronic intrasubstance partial tears of the supraspinatus/infraspinatus at the footprint.
I am experiencing a decrease in the ability to use my arm (right and I’m right-handed) and have trouble sleeping at night from the pain. During the day, I have very little pain and can do most routine daily things.
Is the surgery recommendation a good idea? Thank for any input you may have.
The subscapularis is one of the two most important rotator cuff muscles. Most shoulder surgeons would manage a full tear surgically. But there are many variables that go into surgical decision making. The MRI result is only one variable. So I would consider a formal second opinion since I can not give you specific treatment recommendations.
I have a labrum tear in my shoulder I also have two bone spurs and bicep tendinitis. I’ve had four weeks of physical therapy and a Cortizone injection. It has helped some. My sleep at night is interrupted because of shoulder pain and my ability to lift something mid level and pour it is painful It is my primary arm of use. Right shoulder. My doctor is saying that I’m a good candidate for surgery to repair it. What is your thoughts? I’m nervous to get the surgery but I feel like I will not be able to continue to work and my sleep will continue to be interrupted unless I take pain pills or muscle relaxer. Thanks
Sv
That type of pain is rarely due to a labral tear and often due to rotator cuff tendinosis. But without examining you I can not offer anything more.
Good Luck
I am 55 years if age very active and have a torn labrum up near the bicep tendon. Would you recommend sugery.
Very very very few 50 somethings need surgery for a labral tear. The results of fixing a labral tear at our age are poor. So.. if surgery is entertained at some point then we usually recommend a “biceps tenodesis”. Hopefully you have a good shoulder doc who can explain your options to you. Most of us (Orthopedic surgeons) would initially recommend PT.